
Abstract
Objective:
Dirofilariasis is a parasitic infection caused by filarial nematodes belonging to the genus Dirofilaria. Human dirofilariasis due to Dirofilaria repens has been widely reported from European countries. Sri Lanka is the most affected country in Asia with an infection rate of almost 60% in dog population. However, human infection of D. repens remains undiagnosed and many of the cases are not scientifically documented. Therefore, the objective of the present investigation is to document the presence of dirofilariasis infections in humans.
Method:
A 1 year and 10 months old boy from Ragama, Gampaha District, Western Province of Sri Lanka, was presented to a private hospital with a painless, non-pruritic and ill-defined subcutaneous nodule on his right hypochondrial region of the anterior abdominal wall for 1 week. On examination, there was a non-tender swelling measuring 2 cm × 2 cm in the anterior abdominal wall, with surrounding mild redness. The patient was referred for ultrasound confirmation.
Results:
The ultrasound scan revealed a hypoechoic nodular lesion measuring 11 mm × 6 mm in the anterior abdominal wall. Parasitological examination on the excised nodule confirmed the presence of D. repens measuring 10.5 cm in length having characteristic cuticle with longitudinal ridges.
Conclusion:
It is essential to record the human infections and increase the awareness about this infection, diagnostic tests and vector controlling measures, in order to reduce the disease prevalence through suppressing vector densities, proper diagnosis and patient care.
Keywords
Introduction
Dirofilariasis is a parasitic infection caused by filarial nematodes belonging to the genus Dirofilaria (Nematoda, Filarioidea, Onchocercidae). 1 It is caused by Dirofilaria repens, Dirofilaria immitis, Dirofilaria tenuis and Dirofilaria ursi. 2 D. repens generally inhabits the subcutaneous tissue of dogs, foxes and cats, while D. immitis mainly inhabits the right ventricle and pulmonary artery of the dogs and cats. 3
Human dirofilariasis due to D. repens has been widely reported from European countries such as Italy, France, Greece and Spain. 4 Sri Lanka is the most affected country in Asia with an infection rate of almost 60% in dog population.5,6 Subcutaneous nodules due to dirofilariasis occur in exposed areas of the body such as face, orbits, upper limb, lower limb, chest wall and male genitalia. 5
Adult female Culex, Aedes and Anopheles mosquitoes are vectors for this parasite, which take up the microfilaria while feeding the blood of an infected host. 7 Microfilaria develops in the Malpighian tubules of mosquitoes into the third stage larva and then migrates to the proboscis through the body cavity. The transmission takes place when an infected mosquito bites the dogs or other hosts including humans during a subsequent blood meal.3,8 There have been an increasing number of people infected by D. repens in recent year in Sri Lanka.9–11 Most cases are diagnosed only after excision biopsy. Limited cases were detected pre-operatively on ultrasonography as in this study and were subsequently confirmed with histology and parasitological investigation. 4
Case presentation
A 1 year and 10 months old boy from Ragama, Gampaha District, Western Province of Sri Lanka, was presented to a private hospital with a painless, non-pruritic and ill-defined subcutaneous nodule on his right hypochondrial region of the anterior abdominal wall (Figure 1) for 1-week duration. On examination, there was a non-tender swelling measuring 2 cm × 2 cm in the anterior abdominal wall, with surrounding mild redness. The swelling was firm in consistency. No similar lesions were detected in other parts of the body. No lymphadenopathy, hepatomegaly or splenomegaly were detected. Results of systemic examination were normal.

Photograph shows a subcutaneous lesion measuring 2 cm × 2 cm.
Hematological investigations including eosinophil count were within normal limits. The patient was referred to an ultrasound (US) scan. The US with a high-resolution linear probe (12 MHz) revealed a hypoechoic nodular lesion measuring 11 mm × 6 mm in the anterior abdominal wall. The magnified image demonstrated a coiled structure with parallel echogenic walls, which showed active movement within the nodule (Figure 2). Therefore, the present case was suspected as a subcutaneous nodule due to a parasitic worm.

High-resolution ultrasonography image shows linear hyper-echoic lesions, that is, worm within the subcutaneous nodule.
The nodule was excised under general anesthesia and the live filarial worm was extracted. Parasitological examination confirmed the presence of Dirofilaria repens measuring 10.5 cm in length (Figure 3) having characteristic cuticle with longitudinal ridges (Figures 4–6).
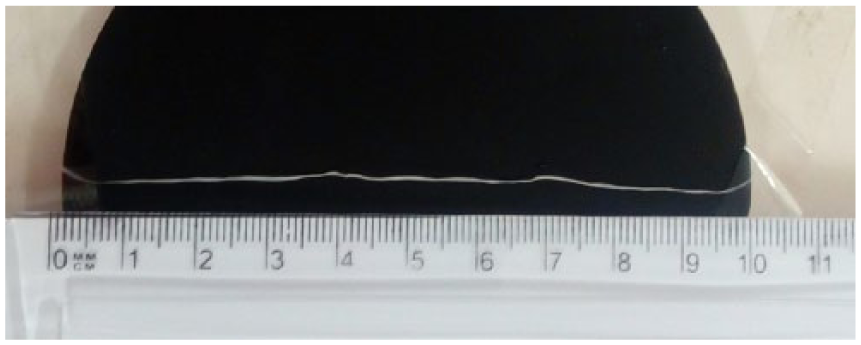
Adult worm of Dirofilaria repens (10.5 cm) recovered from the nodule.

Photograph on glycerin wet mount fixed with formalin shows multilayered cuticle with distinct longitudinal ridges.

Hematoxylin-eosin stained longitudinal section of D. repens worm showing thick multilayered cuticle and muscle cell layer.

Transverse section of D. repens with the arrangement of the longitudinal muscles and the multilayered cuticle.
Discussion
Human dirofilariasis was first reported in 1962 in Sri Lanka from a 15-year-old boy who had a live worm removed from the chest wall.12–14 There is an increasing trend of the number of cases, resulting the second highest in the world. 14 In Sri Lanka, there is no proper routine diagnosis or screening has been implemented to track the prevalence of the infections. Therefore, many of the cases remain undiagnosed or without notification. As in the documented studies, there have been 84 cases reported and they include three expatriates from Russia, England and Korea who were infected in Sri Lanka.9,13 Some studies conducted in Sri Lanka have evidenced that human dirofilariasis is caused mainly by D. repens. 14 However, D. immitis is not present in Sri Lanka although it is present in neighboring countries such as India and Malaysia. 9
According to the available literature, approximately 30%–60% of dogs have been infected in different regions of the country and mosquitoes such as Aedes aegypti, Armigeres subalbatus, Mansonia uniformis and Mansonia annulifera are responsible in transmitting the disease. 9 The worms detected in humans were unable to reach maturity. Therefore, it is unable to express larvae in the blood stream. This may describe the rarity of microfilaremia in humans. Since there are no microfilariae in the blood stream in many of the recorded cases, anti-filarial/anthelmintic medications are not effective.4,15 Therefore, complete excision of the nodule with extraction of the worm is successful in most cases.
However, the antiparasitic treatment is most likely effective to arrest the worm, allowing its subsequent removal since there is only one infertile parasite present. 16 If secondary lesions are suspected in deep body sites such as chest or abdomen, a course of ivermectin and diethylcarbamazine (DEC) may be advisable to prevent further invasive surgery. A course of chemotherapy may also be warranted after heavy exposure to mosquitoes in an area known to be endemic for dirofilariasis. 17 A novel approach for the treatment of cardiopulmonary dirofilariasis is targeting the Wolbachia rickettsial endosymbionts. Treatment with tetracyclines has been reported to damage D. immitis, even causing death of adult worms. 18
The most common presentations of dirofilariasis are subcutaneous and submucosal lesions. 19 Diagnosis is usually based on a high clinical suspicion in patients from endemic areas. Peripheral blood eosinophilia is an inconsistent finding and is dependent on the host’s immune response. 20 Enzyme linked immunosorbent assay (ELISA) for antibody response to D. repens somatic antigen is a useful adjuvant test in endemic areas with a strong clinical suspicion prior to surgery, 4 although it has been found to be negative in many cases. 15 A definitive diagnosis is secured on isolation of the worm. High-resolution ultrasonography is the imaging modality of choice, as live motile worms can be visualized in real time. 21
Although human infection with D. repens has been increasing in Sri Lanka and other parts of the world, many of them remain undiagnosed or unpublished. This can create a disease epidemic situation with the presence of potential vectors for transmission. Hence, there is need for increased awareness about this infection, diagnostic tests and vector controlling measures, in order to reduce the disease prevalence through suppressing vector densities, proper diagnosis and patient care.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the guardian of the patient for their anonymized information to be published in this article. Parents of the minor patient were legally authorized representative(s) to provide informed consent.