
Abstract
A tremendous need for sonographers and vascular technologists exists, however it would be informative to look back at a time when a similar demand occurred. A review of the history of sonography is provided and how it impacted the Center for Medical Ultrasound at Wake Forest University. This historical review also marks the rise of early sonography education and how it evolved into a range of options such as a 4-year Bachelor of Science degree, a 2-year Associate Science degree, or a multiweek certificate program. No matter the length of the program, or the style in which it is delivered, the following basic key ingredients are considered requisite:
• Access to newer model ultrasound equipment systems
• Dynamic classroom lectures (online, live, or a combination of both)
• Active clinical experiences under the guidance of an experienced and enthusiastic sonography expert, specific to a sonographic specialty (OB, cardiac, abdominal, etc.).
Without all these key ingredients, the educational program will not be effective and sustainable. Sonography is a visual science and vital to display images, for the interpreting physician. The sonographer and physicians must work closely as a unified team. An effective working team (physician and sonographer) allows for trading ideas and suggesting possible answers to the diagnostically difficult patient cases.
As we look forward to a tremendous need for sonographers and vascular technologist, it is important to look back at a similar time when sonographers and vascular technologists were in great demand. For those unfamiliar, here is a brief review of our history of the development of ultrasound and as a developing diagnostic imaging modality.
Ultrasound Experimentation: 1877–1947
The French physicist Pierre Curie discovered piezoelectricity in 1877, and this discovery was considered the birth of ultrasound. 1 The World Wars I and II, as well as the catastrophic sinking of the Titanic in 1912, advanced ultrasound’s development. During the wars, there was a need to detect submarines, and with the sinking of the Titanic, it underscored the need to detect objects under water. Paul Levins, one of the first students of the Curie brothers and Constantin Chilowsky, invented a device to detect submarines during World War I. The device they invented used the piezoelectric effect, which is the ability of certain materials to generate electric charge in response to mechanical stress. In addition, in 1914, Reginald Aubrey Fessenden, an inventor from Canada, designed the first working sonar equipment, in the United States. The sonar system was able to detect icebergs by releasing low-frequency sound and recording the echoes that returned. The underwater object detection and its physics are the very basics and foundation of early ultrasonic imaging. 2
In 1928, Sergei Sokolov, a physicist from the Soviet Union, presented the idea of using ultrasonic waves to find metallic flaws. Based on his work, he was referenced as the father of ultrasonic testing. In 1935, Robert Watson-Walt a physicist from England, invented the first pragmatic radar system to detect aircraft. 3 In 1942, Karl Theodore Dussik, a neurologist from the University of Vienna used ultrasound beams to traverse the head, and identify brain tumors. This method was called hyperphonography, and thus Dussick launched diagnostic sonography. In 1947, Dussik also constructed a machine to make pictures of the brain and ventricles using heat sensitive paper to record the reflection from the ultrasound transferal, these pictures were called “ventriculograms.” 3
The Ultrasound Clinical Infancy: 1947–1965
In 1948, the First Congress of Ultrasound in Medicine met in Erlangen, Germany, and the only presenters at that meeting were Wolf-Dieter Keidel and Karl Dussik. They discussed the use of ultrasound in diagnostic medicine and the other participants discussed the use of ultrasound in therapy. This was an important milestone because it paved the way for ultrasound to not only be used in military operations but also as a clinical application. 3 In 1949, George Doring Ludwig, was given credit for creating the first application of ultrasound, in the use of detecting gallstones, in animals. Interestingly, sonography remains the number one diagnostic imaging technique, based on efficiency and specificity, for the detection of gallstones. 4 In 1949, a radiologist named Douglas Howry refined a pulse–echo equipment system with spare parts from the Air Force radar equipment and radio stores. He also later added a 35-mm camera to record sonographic images. Two years later, in 1951, he and a nephrologist, Joseph Holmes, invented a B-mode linear compound equipment system 5 (see Figure 1). They also introduced the use of compound sonographic scanning, which allowed viewers to see inside the body in a cross-sectional mode and those early images were called sonograms.
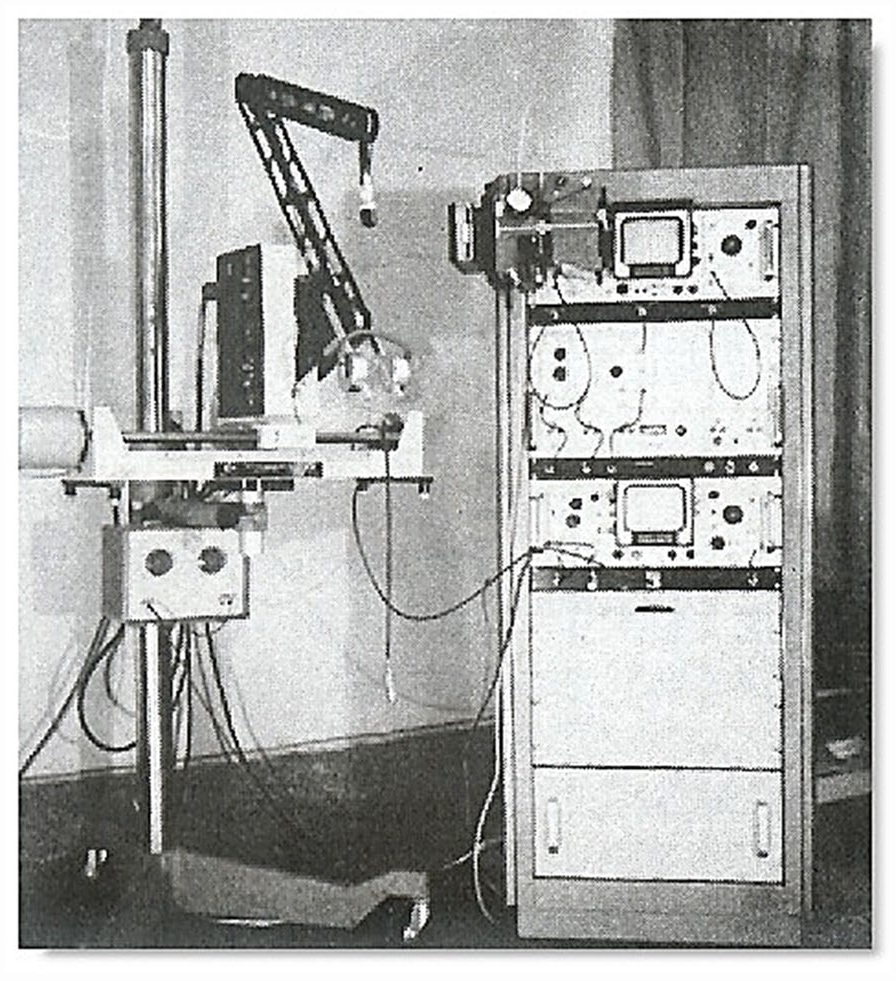
A Picker International articulated arm B-mode ultrasound equipment system (circa 1970). 5
In 1952, a professional group called the American Institute of Ultrasound in Medicine (AIUM) was founded “to support and encourage the use of ultrasound in medicine.” 6 This group “strives to continuously improve the quality of diagnostic sonographic services by offering a peer review process for providers to demonstrate that they meet nationally recognized standards and guidelines.” 7 In 1954, Inge Edler and Carl Hertz reported on the motion mode (M-mode) display. He performed it with a metal-flaw detector and the M-mode horizontal display, and it went on to be used to detect cardiac valve motion. In 1955, Shigeo Satomura, a physicist from Japan, and his team used Doppler shift methods in the study of the heart and the peripheral blood vessels. This would become the first clinical application of the Doppler effect. 8
In 1957, a Scottish engineer, Thomas Graham Brown and a Scottish physician Ian Donald, invented the first compound brightness mode (B-mode) contact ultrasound equipment system. 9 It came with a transducer which operated at 2.5 MHz. This revolutionized the imaging portion of sonography and allowed for increased resolution and improved image detail. Prior to this, the sonograms were black and white dots either on a white or black background, in a 1-dimensional plane. The compound B-mode equipment system allowed overwriting of the image, which produced more detailed images of the anatomy, whether it was the human abdomen or the fetus. Due to this invention, Ian Donald was later known as the father of OB/Gyn sonography. 4 In 1963, the first handheld compound contact B-mode equipment system was commercially introduced, in the United States. This was the beginning of some the most popular models of ultrasound equipment systems, to date.
The Ultrasound “Boom”: 1965–1975
Richard Soldner, Walter Krause, J. Paetzold, and P. Weiser, in 1965, developed a real-time imaging equipment system. Real-time imaging allowed for sonographic images to be created as movement was happening or in “real time.” An example of “real-time” was seeing a baby’s hand move in utero, on the ultrasound equipment system’s screen, as it occurred. This first-generation machine was called a Vidoson and this real-time system, was manufactured by Siemens Medical systems (Germany). 3 It was composed of three transducer heads “housed in front of a parabolic mirror housed in a water system and produced 15 frames per second.” 3 This development further refined real-time imaging and allowed for more frames per second. An analogy of how important frames per second is to sonography can be also noted in the movie industry The early silent movie films were jumpy and choppy due to the low number of pictures or frames per second. However, if you increased the number of frames per second, the motion or movement smooths out much like the modern cinematic films we enjoy today.
In 1966, Don Baker (husband of Joan Baker), John Reid, and Dennis Watkins invented pulsed Doppler electronics, which was used to correlate blood flow through the heart. 4 In 1969, the First World Congress on Ultrasonic Diagnostics in Medicine was held in Vienna, Austria. 4 This provided a global venue for sonography to be introduced into medical practice, as well as being taught to a large cohort of global educators. This identified need for sonography employees was a catalyst for the school of sonography at Bowman Gray School of Medicine and to meet the needs of the medical center and surrounding area.
In 1970, The American Society of Ultrasound Technical Specialists (ASUTS) was organized by six technical specialists for the purpose of facilitating sonography education. This would later become the Society of Diagnostic Medical Sonographers (SDMS). The SDMS was founded to provide education to its members and the medical community as to the science of diagnostic medical sonography. The first ASUTS annual meeting was held in Philadelphia, Pennsylvania in 1972, in conjunction with the 16th annual meeting of the AIUM. 10 In 1973, the occupation of diagnostic medical sonography was created by the American Medical Association’s (AMA’s) Manpower Division as a new allied health occupation. It was from this creation that the term sonographer was developed. This was highly influential in the naming of the credentialing body, the American Registry of Diagnostic Medical Sonographers (ARDMS). 10
Sonography’s Impact on the Bowman Gray Center for Medical Ultrasound, at Wake Forest University
In the years of 1975 through 1985, Wake Forest employees played an enormous supportive role in the development of the profession. 11 To put things in context, here are some interesting samples of the financial investments that were needed, to further sonography at Wake Forest. Based on communications and letters from the archives at Carpenter Library, in 1963, the cost for a sonogram and an echoencephalogram, were as follows: “Private patients, $10.00 if done in the department and $15.00 if done portable. And for service patients (outpatient) $5.00 if done in the department and $7.50 if portable.” This information was based on a letter to Mr Clyde Hardy and Dr James Toole from Dr William McKinney, dated November 20, 1963.
Sonography was growing very fast and further demand for sonography services were outlined in a letter dated May 9, 1972, for the execution of sonography services, within the hospital. The letter stated, The development of the laboratory, as you know, has been on a multidisciplinary basis with subsections assigned and personnel trained in the following areas: Neurology, Cardiology, Urology, and Obstetrics/Gynecology. These are active services at the present time under the direction of Dr. William McKinney, Neurology, Dr. Early Watts, Cardiology, Dr. William Boyce, Urology, and Dr. Stephen Anderson, Obstetrics/Gynecology.
So, in response to the worldwide need for educated sonographers, the Sonic Medicine Training School for Sonographers was created in Winston Salem, North Carolina, to meet the needs of the medical community for trained medical diagnostic sonographers. The report dated April 30, 1975, by Larry Ortman of management engineering specifically stated that more sonographers need to be trained, to meet the needs of the growing profession and the hospital. The concern was that the institution was losing money due to most of the clinical research being done by physicians and at that time, there were no sonographers available to train or to perform sonography. At that time, a conservative estimate was that it cost $30 per study for technical services and the hospital was losing about US$1200 per month. Administrators at the institution felt that it was vital and urgent that they hire and train sonographers. The only solution to their staffing crisis was to start their own school, which answered their defined need.
To explain this further, a memorandum to Dr James Toole, Professor and Chairman, Department of Neurology from Dr William McKinney dated May 9, 1972, outlined the present needs for sonography at the Wake Forest Bowman Gray School of Medicine. His letter stated, Services are provided on a day-to-day basis for midline echoencephalography, measurement of ventricular size, pericardial effusion, ventricular wall thickness, study of cardiac valves, placenta localization, fetal head-size, gynecological masses, and prostatic scanning. The laboratory will have on-line within the next month the addition of carotid artery scanning, liver scanning, aortic scanning, renal and bladder scanning, and other studies as they are developed in the Clinical Research Laboratory based on experience.
As noted, the need for sonographic services was growing at an unprecedented rate, locally.
Sonography required a unique three-dimensional understanding of the human anatomy. Up to this time medical anatomy, education had comprised of cadavers, two-dimensional paper charts and plastic models. A method of demonstrating the three-dimensional views was needed so graduates were faced with the interpretation of images and handling patient cases daily, as well as other newer radiology techniques. This made it necessary to innovate their education and require knowledge of three-dimensional anatomy. Dr Joseph Whitley, Chairman of the Medical Education Committee, (based on a letter from Dr William McKinney to Dr Joseph Whitley, dated November 21, 1975) stated the following, It is apparent that our graduates will be faced with daily interpretation of cross-sectional anatomy from the many new procedures being developed with diagnostic sonography and newer techniques of radiology. There will be many changes in the medical curriculum as these new techniques supplement and in some cases replace previous diagnostic studies daily.
The parallels to our current need for sonography and vascular testing are striking. Once again patients need a wide variety of ultrasonography services, and we are struggling to train and hire qualified sonographers and highly trained interpreting physicians.
Conclusion
Currently, there are many sonography programs across the globe which range from a 4-year Bachelor of Science degree, a 2-year Associate Science degree, or a multiweek certificate program. No matter the length of the program, or the style in which it is delivered, the following basic key ingredients are considered requisite:
Access to newer model ultrasound equipment systems
Dynamic classroom lectures (online, live, or a combination of both)
Active clinical experience under the guidance of an experienced and enthusiastic sonography expert, specific to a sonographic specialty (OB, cardiac, abdominal, etc.).
Without all these key ingredients, the educational program will likely not be effective and sustainable. Sonography has always been a visual science. It is vital to produce high-quality images but most of all it is important to understand human anatomy and pathology. This is vital in displaying images for the interpreting physician, in such a way, as to provide the interpreter a story from which they can assemble the final interpretation. The sonographer and physicians must work closely as a unified team. One must not be above the other, but side-by-side trading ideas and suggesting possible answers to the diagnostically difficult patient cases, presented to the team to solve.
Footnotes
Acknowledgements
I am grateful for Dr Joseph Woo’s permission for the use of ![]() for this publication. I thank my thesis committee at Wake Forest University; the thesis participants themselves; Diane Johnson the Senior Professional Librarian at Coy C. Carpenter Library of Wake Forest University, School of Medicine; and my family for all the assistance and continued support.
for this publication. I thank my thesis committee at Wake Forest University; the thesis participants themselves; Diane Johnson the Senior Professional Librarian at Coy C. Carpenter Library of Wake Forest University, School of Medicine; and my family for all the assistance and continued support.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.