
Abstract
Triplet pregnancies are rare, and monozygotic triplet pregnancies are even rarer. Triplet pregnancies present increased risk in every aspect of the prenatal course. The rate of triplet and higher order births, in the United States, was 78.9 per 100 000 and that rate has decreased from a peak, in 1998. Sonography plays a vital role in the diagnosis and management of all multifetal pregnancies. To further illustrate the importance of sonography, a case of spontaneous monochorionic triamniotic (MCTA) triplets is presented. This set of triplets were delivered at 32 weeks gestation without significant adverse neonatal outcome.
Multifetal pregnancies occur when either multiple oocytes are fertilized (polyzygotic) or when a single oocyte is fertilized and subsequently duplicates (monozygotic). The rate of triplet and higher order births in the United States is 78.9 per 100 000 in 2022 and that rate is down 58% from the peak rate of 198 in 1981. 1 The rate of polyzygotic pregnancies vary worldwide in different populations, being highest in Africa and lowest in Japan. 2 All triplet pregnancies account for approximately 1:7000 births. The rates of monozygotic twin pregnancies are relatively constant throughout different populations, being 1:250 for twins. 2 Higher order multifetal pregnancies (3 or more) are rarer, accounting for 1:100 000 for births. 3
In monozygotic multifetal pregnancies, the chorionicity and amnionicity is determined by the timing of the duplication of the zygote. 3 Duplication which occurs 1 to 3 days from conception will result in individual chorions and amnions, while duplication between 4 and 7 days will result in 1 chorion and individual amnions. If the duplication occurs 8 and 11 days following conception the result will be 1 chorion and 1 amnion, and if the duplication occurs beyond 11 days, the result is likely to be conjoined fetuses.
Case Report
A 21-year-old primigravida presented for her routine initial new pregnancy intake visit at approximately 9 weeks gestational age. Transvaginal sonography revealed a triplet gestation that appeared to be monochorionic. The patient was referred to the maternal fetal medicine department for evaluation of chorionicity and amnionicity. A transvaginal sonogram performed at 10 weeks demonstrated a single placenta and 3 amniotic sacs (see Figure 1). The diagnosis of a monochorionic triamniotic (MCTA) pregnancy was established at that time.
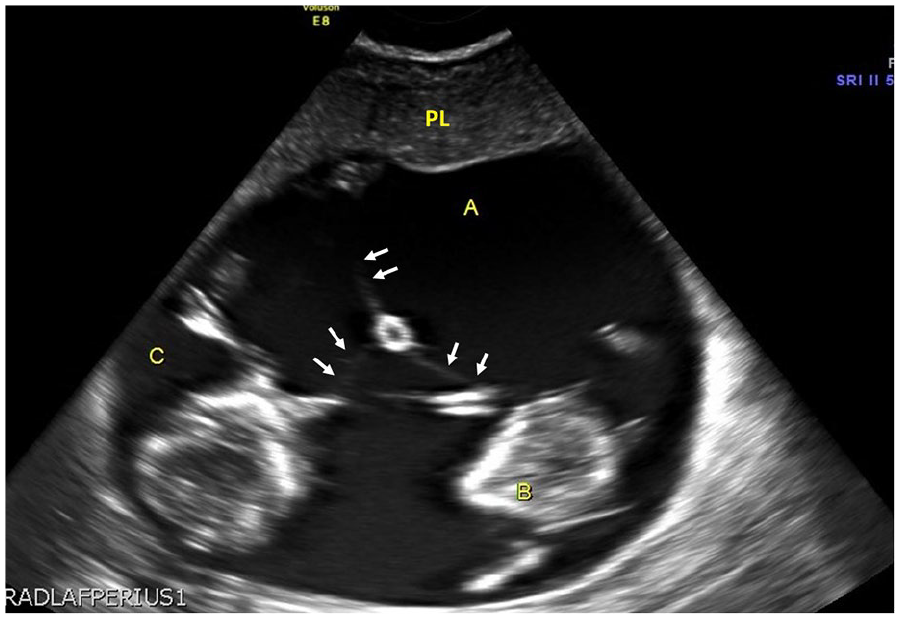
A sonographic image that demonstrated 3 fetuses (A, B, C), the dividing amnion (arrows), and the single placenta (PL), at 12 weeks gestation.
The patient was followed closely throughout her pregnancy utilizing standard protocols for twin-twin transfusion syndrome (TTTS) and twin anemia-polycythemia sequence (TAPS) surveillance, fetal growth monitoring, detailed anatomic surveys (see Figure 2), and a fetal echocardiography. In the third trimester, the fetuses labeled B and C both developed growth restriction. At 30 weeks and 5 days, all 3 fetuses were noted to have either intermittent absent end diastolic flow or absent end diastolic flow on umbilical Doppler evaluation (see Figures 3–5). The patient was admitted for monitoring and given a course of corticosteroids. At 32 weeks and 5 days the triplets were delivered by cesarean section.
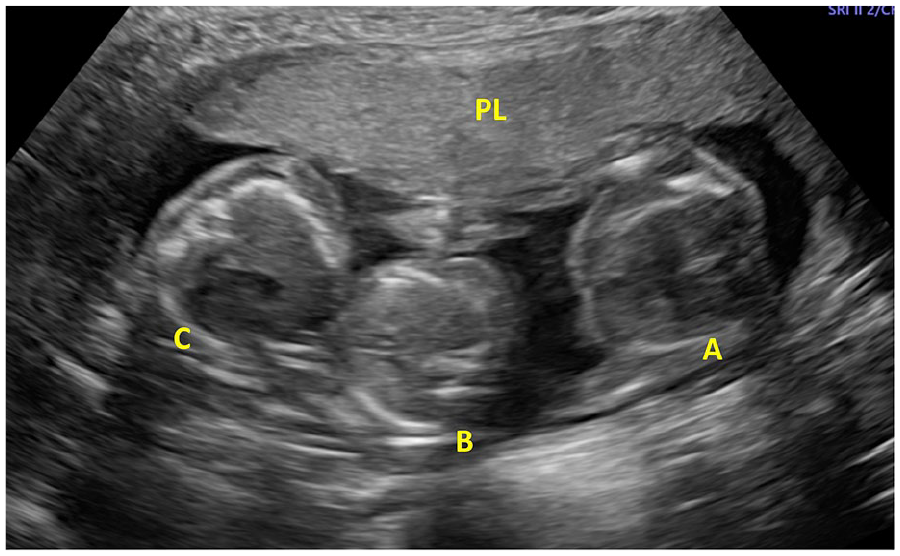
A sonographic image that demonstrated triplets (A, B, C) and placenta (PL), at 18 weeks gestation.
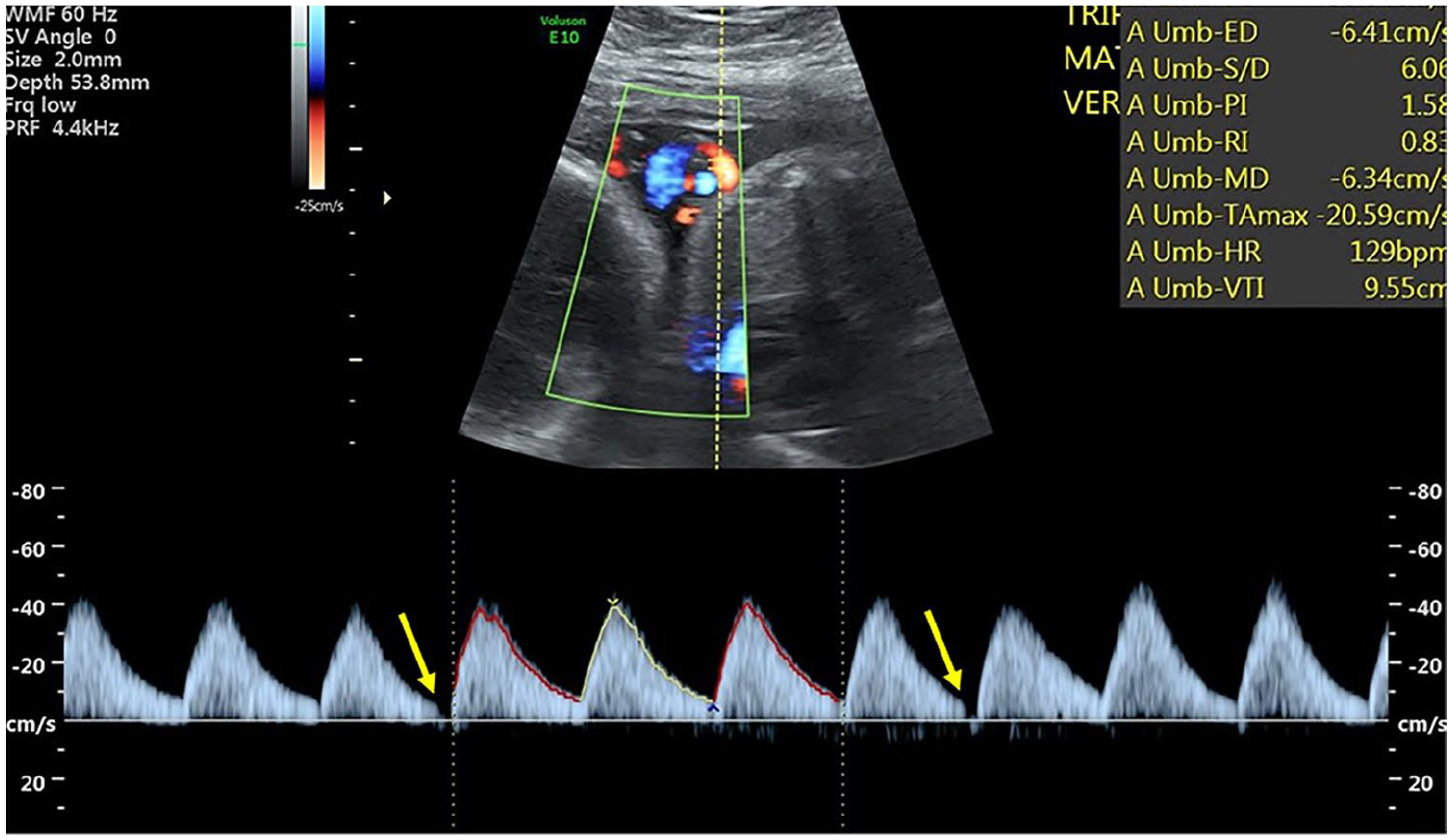
A triplex sonographic image that demonstrated intermittent absent diastolic flow in the fetus labeled as triplet A.
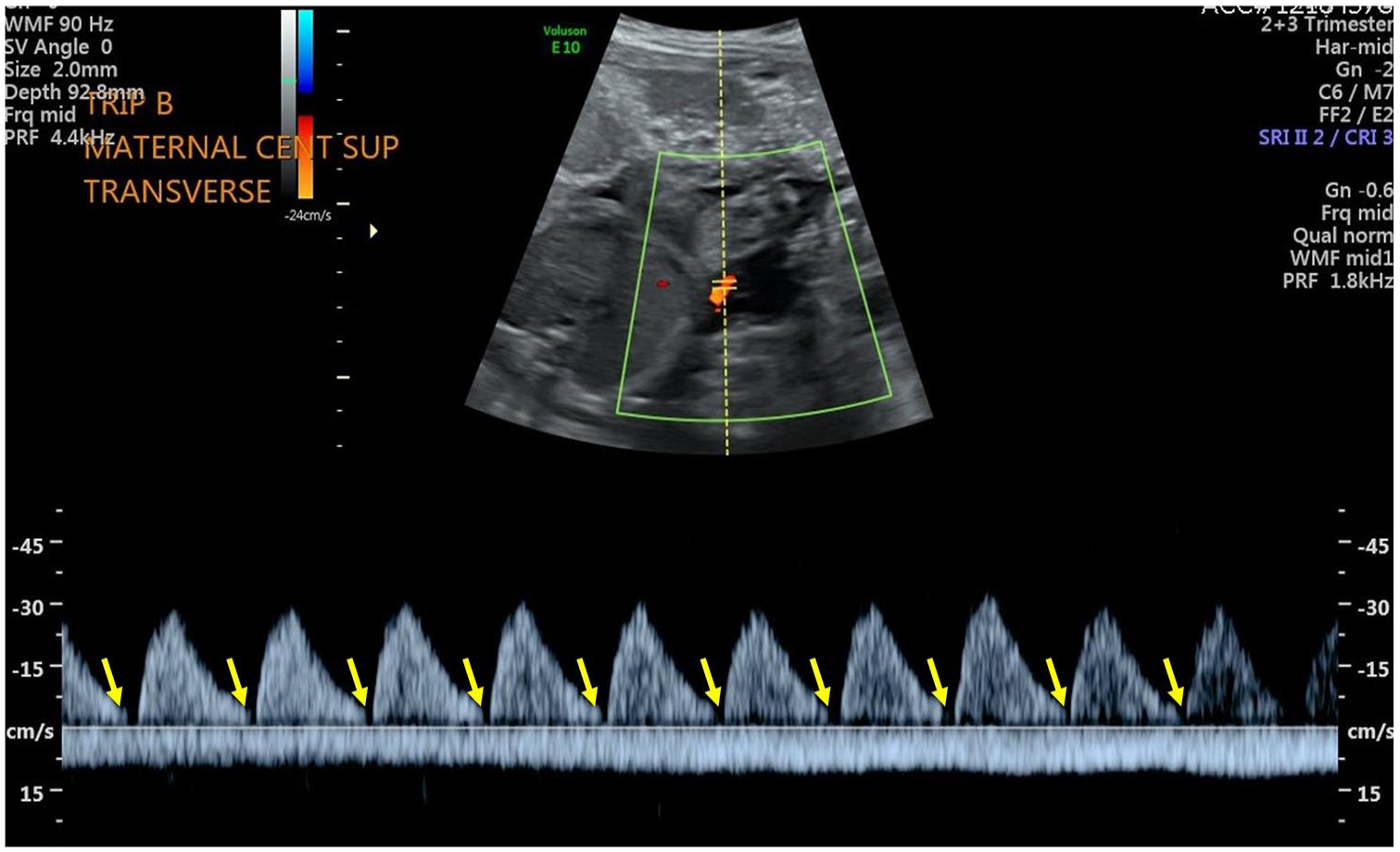
A triplex sonographic image that demonstrated an absent end diastolic flow in the fetus labeled as triplet B.
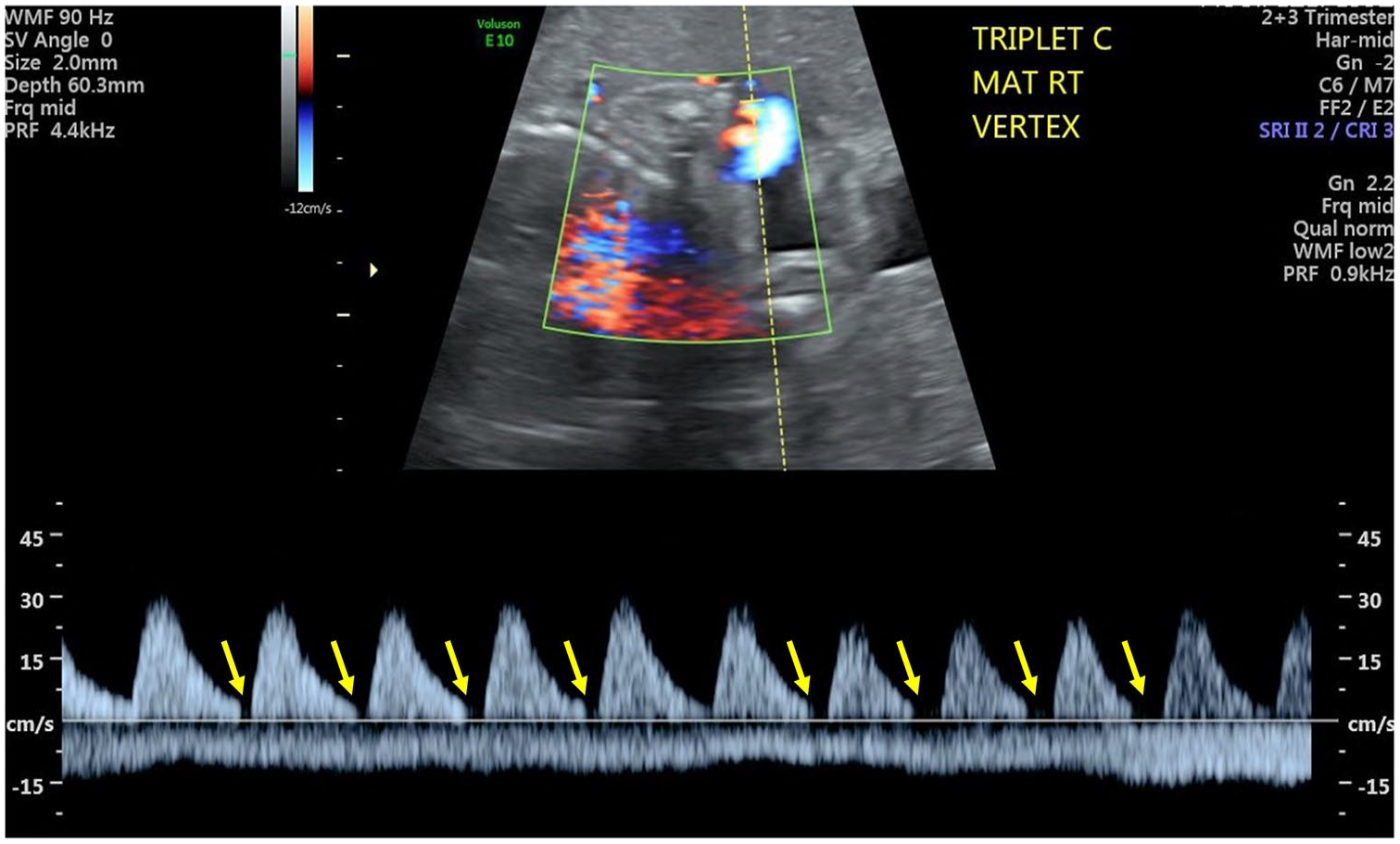
A triplex sonographic image that demonstrated absent end diastolic flow in the fetus labeled as triplet C.
The 3 females weighed 2300, 2200, and 2100 grams and had Apgar scores of 6/8, 6/8, and 6/7 at 1 and 5 minutes. All 3 were transported to the neonatal intensive care unit on room air. A single placenta was delivered demonstrating 3 cord insertions (see Figure 6). The triplet’s neonatal hospital course was uneventful, and all 3 were discharged home on their 21st day of life.

The placental specimen that demonstrated a single placenta and 3 umbilical cords (A, B, C).
Discussion
As mentioned, the incidence of triplet pregnancies in the United States is 1:5000 and the incidence of monozygotic (MZ) triplets is 1:10 000. 1 Most triplet pregnancies (68%) occur by assisted reproductive technologies. 3 Of the MZ triplets, 70% will be either dichorionic (DC) or trichorionic (TC). 3 MCTA triplet pregnancies are rare, with a reported incidence of 1:100 000 and spontaneous MCTA are even rarer accounting for only 4.25% of triplet pregnancies. 3 Complications related to monochorionicity may occur in up to half of MCTA pregnancies. 3 Multifetal pregnancies present unique diagnostic challenges for sonographers. In addition to the general increased risks of preterm birth, increased perinatal morbidity and mortality, preeclampsia, and postpartum hemorrhage associated with all multifetal pregnancies, monochorionic gestations are at risk for TTTS and TAPS. MCTA triplets have a 5-to-8-fold higher risk of perinatal death compared with trichorionic pregnancies.4 Growth discordance (> 35%) occurs in 26% of MCTA pregnancies. 4 Serial monitoring with sonography is essential in the management and decision-making process in the care of these pregnancies. Current recommendations include a sonogram at 18 to 22 weeks for evaluation of fetal anatomy, amniotic fluid, placentation and fetal growth. Monochorionic pregnancies should also be evaluated every 2 weeks for evidence of TTTS and TAPS. This would involve measuring amniotic fluid pockets, documenting the presence of fetal bladders, and Doppler evaluation of the middle cerebral artery. If fetal growth restriction is suspected, serial sonographic monitoring of estimated fetal weight, amniotic fluid volume, and umbilical artery Doppler waveforms should be initiated. 5
Conclusion
The use of sonography and the role of the sonographer are an important part of the care plan for patients with multifetal pregnancies. The sonographic evaluation of multifetal pregnancies can present significant challenges to the sonographer and a thorough understanding of the types of placentation, the unique components of the examination for multiples, and the potential abnormal findings, are essential to provide high quality obstetrical surveillance. This collaborative effort of the sonographer and the obstetrical team contributes to the goal of a positive outcome for the mother and infants.
Footnotes
Ethics Approval
Ethical approval was not sought for the present study because only anonymous information was used in this report.
Informed Consent
Informed consent was not sought for the present study because all case data was de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.