
Abstract
Monozygotic triplet pregnancies are very rare in assisted reproductive technology, and the relationship between monozygotic multiple pregnancies and several assisted reproductive techniques, including blastocyst transfer, remains unclear. Here, the case of a 28-year-old female patient with dichorionic quadruplet pregnancy following intracytoplasmic sperm injection and transfer of two day-3 fresh embryos, without assisted hatching, is reported. At 7 weeks following embryo transfer, the dichorionic quadruplet pregnancy, comprising monozygotic monochorionic triamniotic (MCTA) triplets plus a singleton, was detected by a transabdominal ultrasound scan. After counselling, the patient underwent selective reduction of the MCTA triplet pregnancy at 7 weeks after embryo transfer. The remaining singleton pregnancy was uneventful, resulting in a live birth at 38+ weeks. As the predictors of monozygotic multiple gestations remain poorly characterized, clinicians and patients should give great consideration to the risks associated with monozygotic multiple pregnancies, even if the patient has not undergone blastocyst transfer.
Keywords
Introduction
Multiple pregnancies following assisted reproductive technology (ART) have significantly increased over recent decades. According to statistics reports from the US Centres for Disease Control and Prevention National ART Surveillance System, 1 ART-conceived multiple-birth infants contributed to 14.75% of all multiple-birth infants (19 570 of 132 703) in 2017 and 14.67% of all twins (18 890 of 128 774), and 17.3% of all triplets and higher-order infants (680 of 3929) were accounted for by ART. 1 However, multiple pregnancies, particularly monozygotic multiple pregnancies, are often at higher maternal and fetal risks, such as twin to twin transfusion syndrome (TTTS) and selective intrauterine growth restriction. 2 Therefore, single embryo transfer is highly recommended and currently considered to be the main method for minimizing the risk of multiple pregnancies associated with in vitro fertilization (IVF). Although the rate of single embryo transfers was significantly higher in 2017 than in 2016,1,3 clinicians still need to pay attention to monozygotic multiple pregnancies, as a special type of multiple pregnancy with high risk and potentially poor outcome.
In order to achieve improvements in pregnancy rates while decreasing the rate of multiple pregnancies, prolonged culture and single blastocyst transfer has become more common. It is important to note, however, that single embryo transfer in ART cannot completely prevent the occurrence of multiple pregnancy. 2 ART itself increases the incidence of multiple births, and monozygotic multiple pregnancies occur more frequently in ART gestations than in spontaneous pregnancies. 4 The prevalence in Japan of multiple pregnancy with zygotic splitting was reported to be 1.36% of ART pregnancies between 2007 and 2014. 5 The mechanism of spontaneous zygotic splitting remains unknown, but many factors, including maternal age, culture media, ovulatory induction, cryopreservation, blastocyst transfer, prolonged culture and micro-manipulation of the zona pellucida, such as intracytoplasmic sperm injection (ICSI) and assisted hatching, are thought to be associated with monochorionic multiple pregnancy.6,7 Compared with monozygotic twinning pregnancies, the occurrence of monozygotic triplet pregnancies is very rare in ART, but the risks and complications of monozygotic triplet pregnancy are significantly increased compared with monozygotic twin pregnancies. 8 Monozygotic high-order pregnancies require increased attention in assisted reproduction. Herein, a case of dichorionic quadruplet pregnancy, comprising monozygotic triplets and a singleton, after intracytoplasmic sperm injection and transfer of two fresh embryos without assisted hatching, is presented, together with a specific review of possible risk factors for the occurrence of monozygotic high-order pregnancies in ART.
Case report
This case report was approved by the Ethics Committee of West China Second University Hospital, Chengdu, China and the patient provided written informed consent for publication of the case. The reporting of this study conforms to CARE guidelines. 9
In August 2016, a 28-year-old female patient (G2P1, with no obstetric-related comorbidities) and her husband received a second IVF cycle with ICSI at the Reproductive Centre, West China Second Hospital, Sichuan University, China, due to obstructive azoospermia. The female patient had a history of regular menstrual cycle; and physical examinations, body mass index, hormonal status and family history of multiple pregnancies were unremarkable for both participants. They had received their first ICSI cycle in 2011, while the female patient was aged 23 years, and obtained four embryos. Transfer of two frozen-thawed embryos in June 2011 resulted in a healthy male infant by vaginal delivery at 38 weeks’ gestation in April 2012. Transfer of the remaining two frozen-thawed embryos in 2016 failed to achieve successful pregnancy, so the couple underwent a second cycle of ICSI in 2016.
Controlled ovarian hyperstimulation was performed using a gonadotrophin-releasing hormone agonist long protocol, in mid-luteal phase. Pituitary down-regulation was initiated on day 21 of the previous cycle by administration of 0.1 mg triptorelin, subcutaneous injection, every other day. Ovarian stimulation was performed with daily intramuscular injections of 225 IU highly-purified urinary follicle stimulating hormone after pituitary down regulation. The total dose of gonadotropins was 2850 IU. After 10 days of gonadotrophin stimulation, human chorionic gonadotrophin (hCG) was triggered with 10 000 IU hCG when at least two follicles were >18 mm in diameter, followed by transvaginal ultrasound-guided aspiration 36 h later. A total of 13 oocytes were retrieved, 10 of which were in metaphase II and were microinjected with spermatozoa obtained by testicular sperm aspiration. On day 3 of incubation, two fresh embryos (compact and 8-cell stage) were transferred without performing assisted hatching, and the remaining three embryos were cryopreserved. The patient received progesterone supplementation with 90 mg progesterone gel, vaginally, daily. Her serum β-hCG level was found to be 144 mIU/ml at 10 days following embryo transfer, and transabdominal ultrasound, performed at 35 days, showed two intrauterine gestational sacs with detectable heart beats (Figure 1). Transabdominal ultrasound, repeated at 7 weeks after embryo transfer, revealed three embryonic buds in one of the gestational sacs. Subsequent transvaginal ultrasound confirmed an intrauterine quadruplet pregnancy, consisting of monozygotic monochorionic triamniotic (MCTA) triplets, and a monozygotic monochorionic monoamniotic (MCMA) singleton, with a detectable heartbeat in all four fetuses. The diameters of the triplet fetuses were 1.9 cm, 2.0 cm and 2.1 cm, respectively, and the diameter of the singleton was 2.3 cm (Figure 2).

Representative image from a transabdominal ultrasound scan performed at 35 days after embryo transfer showing two intrauterine gestational sacs.
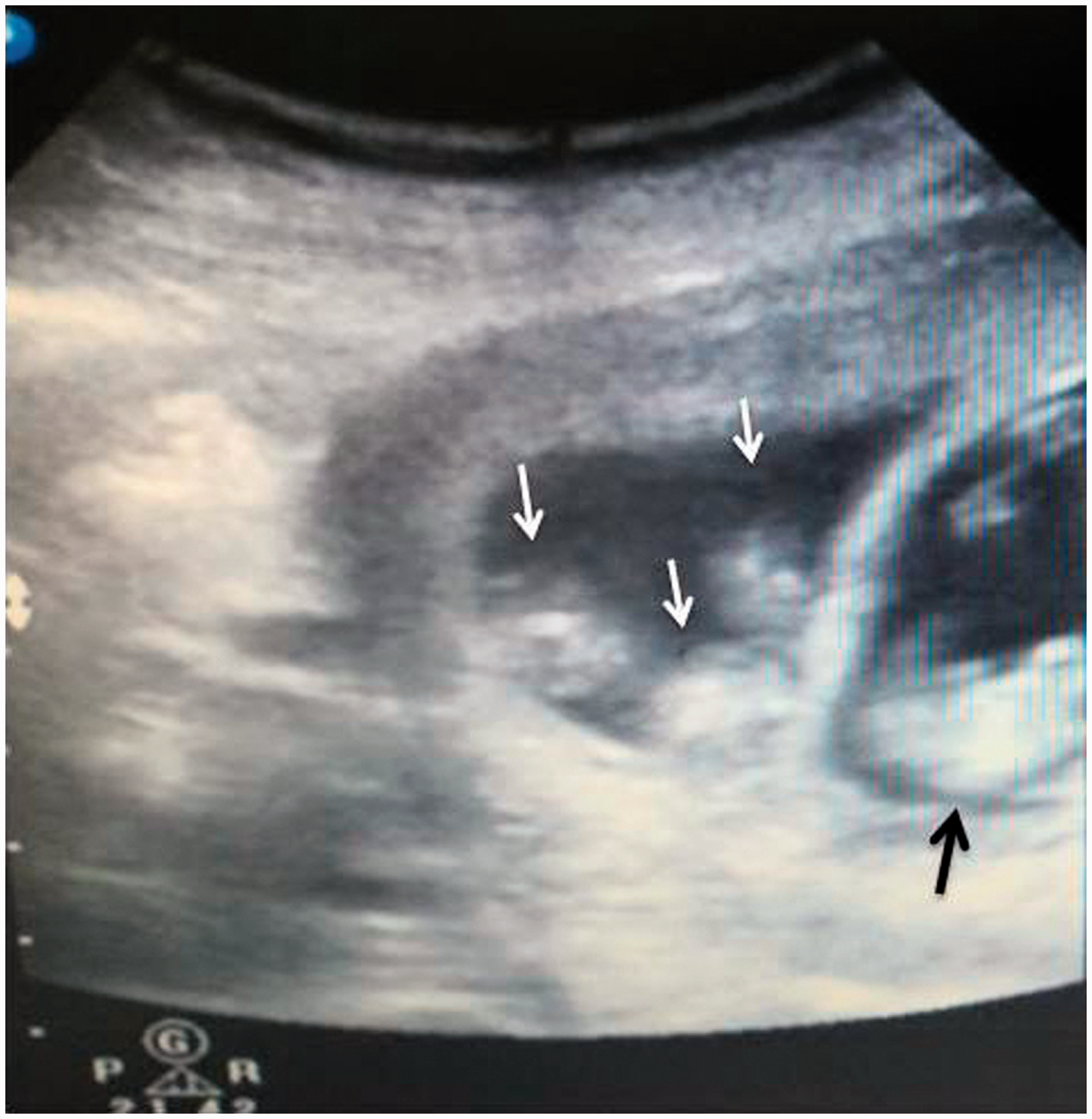
Representative image from a transvaginal ultrasound scan performed at 7 weeks after embryo transfer showing monochorionic triamniotic triplets (white arrows; three viable embryos were detected in one gestational sac); and a single embryo in another gestational sac (black arrow).
The couple was informed about the increased maternal and fetal risks of higher order monozygotic gestations and they were counselled regarding the possibility of a fetal reduction procedure. After extensive counselling, and considering that they had a healthy male child, they decided to undergo selective embryo reduction, and only proceed with the singleton pregnancy. Thus, at 7 weeks after embryo transfer, selective reduction was performed by ultrasound-guided transvaginal aspiration targeted at the MCTA triplets. This resulted in the cessation of cardiac activity in the monozygotic MCTA triplets, whereas normal cardiac activity was observed in the remaining monozygotic MCMA singleton. Subsequent ultrasound examinations after 24 h confirmed the presence of an ongoing singleton pregnancy. At week 10 of gestation after embryo transfer, the remaining singleton had normal nuchal translucency (1.5 mm), and continued to develop normally following selective reduction of the triplet sac. The remainder of the pregnancy was uneventful, and resulted in vaginal delivery of a healthy male infant, weighting 3 200 g, at 38 weeks and 6 days of gestation.
Discussion
This case report describes a quadruplet pregnancy comprising one implanted embryo that developed into a monozygotic monochorionic embryo and the other that split into monozygotic MCTA embryos after the transfer of two fresh embryos generated by ICSI. This case adds to the small number of monozygotic higher-order pregnancies in ART that currently exist in the literature.
The incidence of triplet births is very low, and was reported to be 0.01% of births in the Netherlands in 1980. 10 Monozygotic triplet pregnancies are even more rare, estimated to occur in only 0.004% of natural pregnancies, and found to account for 10% of all triplet pregnancies in a population-based study. 10 Following the introduction and development of ART, the rate of triplet births has increased significantly. The occurrence of triplets and higher-order multiples is estimated to be between 0.1% and 0.2% of pregnancies in the USA, with ART being more commonly associated with triplet pregnancies than twin or singleton pregnancies.1,3,11 In the USA, ART-conceived triplets and higher-order infants contributed to 33.0% of all triplets and higher-order infants in 2010, 11 however, with the increasing use of single embryo transfer, the rate decreased year on year to 17.3% in 2017. Similar to the USA, one-third of triplet pregnancies in the Netherlands are due to ART. 10 A population-based study in 2016 suggested a 60% increase in monozygotic twinning in ART gestations versus natural pregnancy. 12 A study published in 2018 reported a prevalence of 1.36% for multiple pregnancy resulting from zygotic splitting in Japan, and the prevalence of triplets in ART pregnancies was 0.04%. 5 Millions of IVF babies have been born since 1978, and in the largest study to date, Yamashita et al., 7 reported 122 triplet pregnancies and one quadruplet pregnancy after single embryo transfer in Japan between 2007 and 2014. Apart from the study by Yamashita et al., 7 only just over 30 cases of monozygotic triplet pregnancy in ART have been reported to date worldwide. Available published data are based on limited population-based sample studies, small sample studies or case reports.6,8,13–37
The occurrence of monozygotic triple and high-order pregnancies is thought to increase in ART due to similar split mechanisms associated with monozygotic twinning; several procedural factors in ART may be associated with the mechanisms, but the specific ART procedures that lead to splitting remain unknown.2,4,7,12,17,22,23,26,27,35,38–40 In the present study, the limited published reports regarding ART-conceived monozygotic triplet and higher-order pregnancies were reviewed to analyse possible factors.
Several factors relating to ART procedures are thought to be associated with the occurrence of monozygotic triple and higher-order pregnancies. Identifying which specific ART procedures have led to the occurrence of monozygotic triple pregnancies remains difficult due to limited relevant reports in the literature. Many studies have implied a correlation between blastocyst transfer and monozygotic twinning, and suggest that blastocyst transfer is a risk factor for monozygotic twinning.6,7,19,22,23,34,35,39,40 The incidence of monozygotic twinning in ART with blastocyst transfers has increased compared with day 2–3 transfers. 2 Due to the similar split mechanism with monozygotic twinning, the incidence of monozygotic triple and high-order pregnancies is thought to be increased in ART.10,40 From reports on monozygotic higher-order pregnancies published to date, it appears that 56.2% (18/32) have occurred after blastocyst transfer, 9.4% (3/32) after day 4 embryo transfer, and 34.4% (11/32) after day 3 embryo transfer (Table 1).6,8,13–17,19–37,41 Nearly one third of cases of monozygotic triple and higher-order pregnancies with ART involved transfer of day 3 cleavage stage embryos, while higher rates were associated with day 4 embryo and day 5 blastocyst transfers combined. With the increasing popularity of blastocyst transfer in many IVF centres, the monozygotic triple and higher-order pregnancies related to day 3 embryo transfer seems to have become relatively uncommon. The present study describes the third reported case in the last decade of monozygotic triple pregnancies and live birth after day 3 embryo-transfer. With current data and limited case reports, it remains difficult to draw definite conclusions, but the available data suggest that prolonged culture and blastocyst transfer may be one of the important factors in monozygotic higher-order pregnancies.
Summary of the present case and previously published reports of monozygotic triple/quadruplet pregnancies.

AH, assisted hatching; ICSI, intracytoplasmic sperm injection; IVF/ICSI, two selected blastocysts (one produced by in vitro fertilization [IVF] and the other by ICSI); NA, not available; D3, day 3 embryo; D4, day 4 embryo; D5, day 5 blastocyst; CS, caesarean section; MCTA, monochorionic triamniotic; MCQA, monochorionic quadramniotic; MCMA, monochorionic monoamniotic; MCDA, monochorionic diamniotic; DCDA, dichorionic diamniotic; PPROM, preterm premature rupture of membranes; TTTS, twin-to-twin transfusion syndrome; *patient underwent assisted reproductive technology with donor oocytes; #embryo biopsy.
Micro-manipulation of the zona pellucida, such as ICSI, assisted hatching and biopsy, is probably another risk factor for the occurrence of monozygotic multiple pregnancies. Since the first report of a correlation between zona pellucida structure following ART and monozygotic twinning, 42 many studies have analysed the association between micro-manipulation techniques and multiple monozygotic twinning, and have found that manipulation of the zona pellucida may cause disruption and splitting of the inner cell mass and increase the rate of monozygotic twinning.2,17,20,26,34,42 An increased rate of monozygotic twinning has been shown after ICSI and assisted hatching, and the largest study to analyse triplet or quadruplet pregnancies after single embryo transfer reported that blastocyst cultures and assisted hatching (P = 0.002 and P < 0.001, respectively) are risk factors for monozygotic twinning. 7 However, some studies do not support any association between a higher monozygotic twinning rate and micro-manipulation of the zona pellucida.2,4,12,40,43,44 Based on the published case reports summarised in Table 1, 65.6% (21/32) underwent ICSI, and 28.1% of cases (9/32) underwent assisted hatching or biopsy in ART. Of all cases, the zona pellucida was manipulated in 65.6% of cases (21/32), of which, 15 cases underwent blastocyst transfer. Thus, it appears that 47% of the published cases (15/32) received micro-manipulation of the zona pellucida and blastocyst transfer, so it is difficult to exclude the effect of blastocyst transfer as a confounding factor. Of all day 3 embryo transfers, 54.5% (6/11) were found to have occurred after ICSI, while 45.5% (5/11) occurred after IVF, so it appears that ICSI does not increase the risk of monozygotic multiple pregnancies in ART. In addition, a retrospective observational study in Japan, involving 937 848 single embryo transfer cycles, showed that embryo manipulations using blastocyst transfer, assisted hatching and frozen-warmed embryo transfer were potential risk factors for zygotic splitting, however, ICSI was not a potential risk factor. 5 However, in the present case, the transfer was performed with day 3 fresh embryos without assisted hatching, and it appears that ICSI may have been the possible risk factor for the monozygotic multiple pregnancies. Nonetheless, the relationship between ICSI and monozygotic multiple pregnancies remains controversial, and further studies are required to clarify this association.
The correlation between maternal age or oocyte age and monochorionic multiple pregnancy has been analysed in the studies summarised in Table 1. The mean age associated with monochorionic high-order pregnancy was found to be 31.2 ± 4.5 years after excluding four cases (three of which used donor oocytes and one that did not report the age). Twenty-nine of the cases used their own eggs, five patients were older than 35 years, and 24 patients were aged less than 35 years. A meta-analysis showed that younger maternal age may be associated with monozygotic twinning, 2 however, the largest study found no difference in age between singleton pregnancies and monozygotic triplet or quadruplet pregnancies. 7 Therefore, the potential association between age and monozygotic multiple pregnancies requires further investigation. In all cases, only seven out of 32 patients received frozen/thawed embryo transfer; thus, embryonic freezing does not appear to play an important role in the incidence of monozygotic multiple pregnancies, which is supported by a previously published study. 7
Because of the high risks and particular complications associated with monozygotic multiple pregnancies, selective fetal reduction to twins or singleton is an option to improve perinatal outcome. Nearly all of the couples described in the previously published cases were stated to have been informed of the increased maternal and fetal risks of monozygotic higher order gestations, and were counselled regarding the possibility of a fetal reduction procedure. From the results of limited reports summarised in Table 1, 43.7% of patients (14/32) underwent the fetal reduction procedure, and most cases resulted in a successive pregnancy or live birth. In cases of monozygotic triplet pregnancies combined with another singleton or twin pregnancy, the remaining pregnancy was often reported to have better outcomes after reduction of the MCTA.20,26,31,36,41 Reducing one or two fetuses in monozygotic triplet pregnancies may lead to subsequent MCTA fetal death, and some cases with no fetal reduction surgery resulted in live births.14,22,24,29,31,33,34 Although fetal reduction may significantly reduce the maternal and neonatal risk in other twin and multiple pregnancies, it remains unclear whether selective fetal reduction benefits monozygotic triplet pregnancies.
In conclusion, in addition to blastocyst transfer, the relationship between monozygotic multiple pregnancies and several assisted reproductive techniques, such as manipulation of the zona pellucida, remains unclear. As the predictors of monozygotic multiple gestations are poorly characterized, patients should be informed of the risks of monozygotic multiple pregnancies after assisted reproductive techniques. Both patients and infertility specialists need to pay great attention to the risks associated with monozygotic multiple pregnancies, even if the patient only receives general assisted reproductive technology, and does not undergo blastocyst transfer.
Footnotes
Acknowledgements
The authors would like to thank Professor Ling Liu for English language editing.
Availability of data and materials
All available data for this case are presented within this manuscript.
Author contributions
Ying Nie and Xiaoyong Qiao drafted the manuscript and analysed the reported cases. Sicong Li and Zhuo Pan assisted in collection and analyses of clinical materials and pictures. Jing Zhang assisted in collecting and organizing the materials, and Liangzhi Xu drafted and edited the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This case report was supported by the Clinical Discipline Development Fund of West China Second University Hospital (KL068) and the Key Research and Development Program of Sichuan Province (2021YFS0127).