
Abstract
Objective:
The aim of this systematic review and meta-analysis was to evaluate and compare the diagnostic accuracy of ultrasonography (US) and magnetic resonance imaging (MRI) in the diagnosis of placental invasion.
Method:
Two independent scientists carried out a series of searches to obtain relevant research, released from January 1, 2009, to December 31, 2018. National databases (Magiran and SID), KoreaMed, and LILACS were reviewed for literature, released in other languages. A series of MeSH keywords was employed as part of the searching strategy (e.g., pregnancy, pregnant, placental invasion, accreta). A forest plot was built with Meta-DiSc, version 1.4.
Results:
For placental invasion, the sensitivity and specificity of MRI were 89% (95% confidence interval [CI], 83%–93% with a 95% confidence interval) and 97% (95% CI, 93%–99%), respectively. The sensitivity and specificity of US were 73% (95% CI, 66%–79%) and 89% (95% CI, 84%–93%), respectively. In the detection of placenta accreta solely (as the first grade of placental invasion), the sensitivity and specificity of MRI were 89.3% (95% CI, 86%–92%) and 84% (95% CI, 77%–89.6%). The sensitivity and specificity of US detection were 95.4% (95% CI, 93.8%–96.6%) and 87.3% (95% CI, 81.4%–91.9%), respectively.
Conclusion:
Due to the increased cesarean sections, placental invasion may be increasing. The diagnosis of prenatal placental invasion is important to reduce maternal morbidity and mortality. Recent trends indicate an increased use of MRI to evaluate placental invasion as a complement to US. The most accurate imaging findings are using US for placental lacunae and MRI to detect the dark intraplacental band.
The placenta is an organ growing within the uterus during pregnancy. Placental anomalies are important to be diagnosed early, due to the possibility of maternal fetal morbidity and mortality. 1 The most common source of antepartum hemorrhage is abnormal placental implantation that may cause hysterectomy and an associated risk for maternal fetal morbidity and mortality.1–3 Once trophoblastic tissue near a defect in the decidua basalis moves through the decidual layer, it will attack deeper parts of the uterine wall. As placental adherence defects arise, this results in three subclasses of anomaly: placenta accreta, increta, and percreta. 4 The major risk factors for developing placental invasion are previous uterine surgery, cesarean section (CS), routine fetal delivery, and maternal age. 5 While the prevalence of placental adherence defects used to be rare (e.g., 1:30,000 in 1930 and 1:2500 in 1980), 6 the latest research estimates a prevalence of 1 in 250 defects. 6 An increased number of CSs may be the reason for this increasing rate of placental anomalies. No particular symptoms signal placental adherence defects. Primarily, the diagnosis is based on clinical suspicion, particularly in case of a history of CS or placenta previa. If placenta accreta is not diagnosed prenatally, the mother is at higher risk of a life-threatening hemorrhage and surgical complications, such as the ureter and urinary bladder injury.7,8 Due to the enhanced risk of antepartum hemorrhage during maternal labor, the timely diagnosis of an abnormal placentation is vital. This allows surgeons time for sufficient preoperative scheduling and patient counseling.9,10 At the delivery time, normal separation of the placenta is inhibited by abnormal placental adherence or invasion into the myometrium. This could lead to a life-threatening uterine hemorrhage or retained products of conception. The ability to accurately diagnose placenta accreta is critical, considering the major risk of morbidity. It also allows the patient and obstetrician to prepare for potential delivery complications. In addition, it allows for continued antenatal care, to minimize blood loss during and after delivery. 11 Since ultrasonography (US) is low cost and accessible, it remains the main diagnostic instrument for abnormal placentation, along with fetal screening examinations. Gray-scale and color Doppler sonographic findings of placenta accreta consist of blood vessels or placental tissue bridging the placenta-myometrium and myometrium-bladder interface or crossing the uterine serosa. It can also be noted as a loss of the normal placental myometrium interface, lacunae occurrence with turbulent flow, the echogenic line interruption at the myometrium-bladder interface, and retroplacental myometrium thickness of less than 1 mm.12–16 Regardless of using US, it may still be difficult to distinguish the myometrial invasion level. Magnetic resonance imaging (MRI) is a more expensive imaging method compared to US and requires added experience and expertise in assessing atypical placental invasion. MRI is regarded as an adjunctive imaging method and can slightly increase the diagnostic accuracy of US. 17 However, several studies have proposed equivalent diagnostic accuracy of both imaging modalities for placenta accreta. Presently, identified cases of placenta accreta lack adequate proof that MRI is an appropriate imaging alternative. Once accreta is alleged on US, frequently MRI is carried out by some hospitals and medical practices.18,19 MRI can define the degree of placental invasion and can change surgical management. 17 To explore this premise, a systematic review and meta-analysis was conducted to address the accurate antenatal diagnosis of placental invasion with MRI and US.
Method
A systematic review and meta-analysis were based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) principles. The PRISMA approach was used to search for qualified articles. The search for the eligible published articles was confined to the following dates: January 1, 2009, to December 31, 2018. Two independent scientists (H.D. and M.S,) carried out the literature search to obtain the relevant articles during the aforementioned timeframe. The databases searched were MEDLINE via PubMed, EMBASETM via Ovid, and the Cochrane Library to locate published literature in the English. National databases (Magiran and SID), KoreaMed, and LILACS were reviewed for literature released in other languages. References including published articles and corresponding reviews were located through additional searches. This was investigated to ensure that there was saturation of the literature (conducted by F.P.). The Health Sciences Librarian website, with a specialty in systematic review searches via the MeSH and open expressions according to the PRESS norms, was used to add unique search approaches. The outcomes were compared to determine if further databases were needed (M.S. and F.P.) once the MEDLINE search was finalized. PROSPERO was also used to discover the latest or current systematic reviews on this topic. The keywords employed in the search approach were pregnancy [MeSH], pregnant [MeSH], OR magnetic resonance imaging [MeSH], OR obstetric ultrasound [MeSH], OR ultrasound [MeSH], OR imaging, MRI [MeSH], OR placental invasion [MeSH], accreta [MeSH] increta [MeSH], percreta [MeSH] and placenta accrete [MeSH]. To identify the published articles (H.D. and M.S.), the complete list of sources and systematic search results was also checked. Moreover, the authors of research that fulfilled the inclusion criteria were contacted, and unpublished studies and abstracts were requested (F.P.).
Eligibility Criteria
The applied inclusion criteria to select published papers were as follows: (a) original retrospective and prospective blinded research on MRI and US performance for prenatal diagnosis of placenta invasion (accreta/increta percreta); (b) comprising a 2 × 2 table or the data, which allowed for a revised table; (c) describing the accurate diagnostic criteria for placenta invasion on MRI and US; and (d) meeting quality standards, as evaluated by the 14-item Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2). In addition, the thinning or loss of the retroplacental myometrial mantle, loss of bladder wall echogenicity, thrombosed placental lacunae, increased intraplacental vascularity, placental extension into the broad ligament, placental protrusions into the bladder, and abnormal cervical anatomy were criteria used to define the sonographic suspicion of placenta accreta in included studies. The bulging contour of the uterus, loss of bladder wall signal, homogeneous or heterogeneous placental appearance, thinning or loss of retroplacental myometrial mantle, dark intraplacental bands, intraplacental hemorrhage, placental extension into the broad ligament, placental protrusions into the bladder, and abnormal cervical anatomy were criteria used to define MRI suspicion of placental invasion.
Data Extraction and Risk of Bias Evaluation
To assess the participant characteristics, the related data were extracted from included studies. The index test consisted of features, such as special equipment and reference standard (organizer of the tests and the interval between them). Also, the data associated with precision diagnosis were extracted from included studies. The data were extracted by the first reader (M.S.). Then, the data were approved and completed by the second reader (H.D.).
The QUADAS-2 instrument was used to assess the probability of bias for each published article. There were four probable areas of bias areas assessed. The first area of bias was patient selection (picking up the participants accidentally or randomly). The research participants or patients must have been selected in this manner. Therefore, the risk of bias could be elevated for investigations that included only suspected patients for placental invasion. The second area was the index test (incorrect reading of the index test and correct clarification of detection threshold). A reference standard or “gold standard” (99% precision, the interpretation disregarding the index test results) was the third area. The flow and timing (the index test receiver’s description, the time interval between index tests, and reference standard) were the last domain of potential bias. The selected articles had to be assessed by two independent reviewers using the QUADAS-2 criteria (M.S., F.P.). The reviewers debated the article once the independent assessments were completed. To achieve inclusion in the study, each domain was discussed. A κ statistic was applied to measure the reliability of the reviewers for each area of bias.
Statistical Analysis
Pooled measures for sensitivity, specificity, diagnostic odds ratio (DOR), and area under the curve (AUC) with their 95% confidence intervals (CIs) were measured via DerSimonian and Laird. This was further guided by the results of the 2 × 2 tables. 20 Test summary receiver operating characteristic (ROC) curves were rebuilt via Moses-Shapiro-Littenberg on the basis of the pooled DOR for each index. 21 The DOR shows the test capability to distinguish placenta accreta in this case. A DOR of 1 specifies that the test has no discriminative power. The greater the DOR, the better the imaging mode’s diagnostic capacity. A Cochran Q statistic and the I2 index were applied to assess heterogeneity between studies. A significant I2 index specifies heterogeneity outside sampling variation. To detect predefined sources of heterogeneity, a meta-regression analysis was carried out. A forest plot was built with free software: Meta-DiSc, version 1.4 (http://www.hrc.es/investigacion/metadisc-en.htm; Ramon y Cajal Hospital, Madrid, Spain). 22 To offer a comprehensive analysis, the data associated with the diagnostic accuracy of US and MRI were collected. Certain studies then were meta-analyzed by each category. The results also were reviewed to determine a high or low risk of bias in participant selection (according to QUADAS-2 criteria). For each study, according to the true-positive, true-negative, false-positive, and false-negative rates, sensitivity, specificity, and positive and negative likelihood ratios (LRs) were calculated. LRs are autonomous from incidence rates, and there is an agreement that a positive LR >10 and a negative LR <0.1 offer substantial proof of reasonable diagnostic performance. 23 Based on the single global accuracy measure, the ratio of positive LR to negative LR was called, the diagnostic odds ratio. 24 Through a bivariate random-effect model, summary sensitivity and specificity, positive and negative LRs, and diagnostic odds ratios were calculated. The method presumes bivariate normal distributions for the logit transformations of sensitivity and specificity of particular investigations.25,26 Furthermore, the hierarchical summary ROC curve was built by specifying the point estimations for each research, the joint ROC curve, and the pooled characteristics with the 95% CI and the 95% prediction region. 27
Results
Based on the search strategy outlined, 1155 studies were selected. After examining the conformity of the studies with the required criteria, 17 studies were selected for final review (Figure 1).
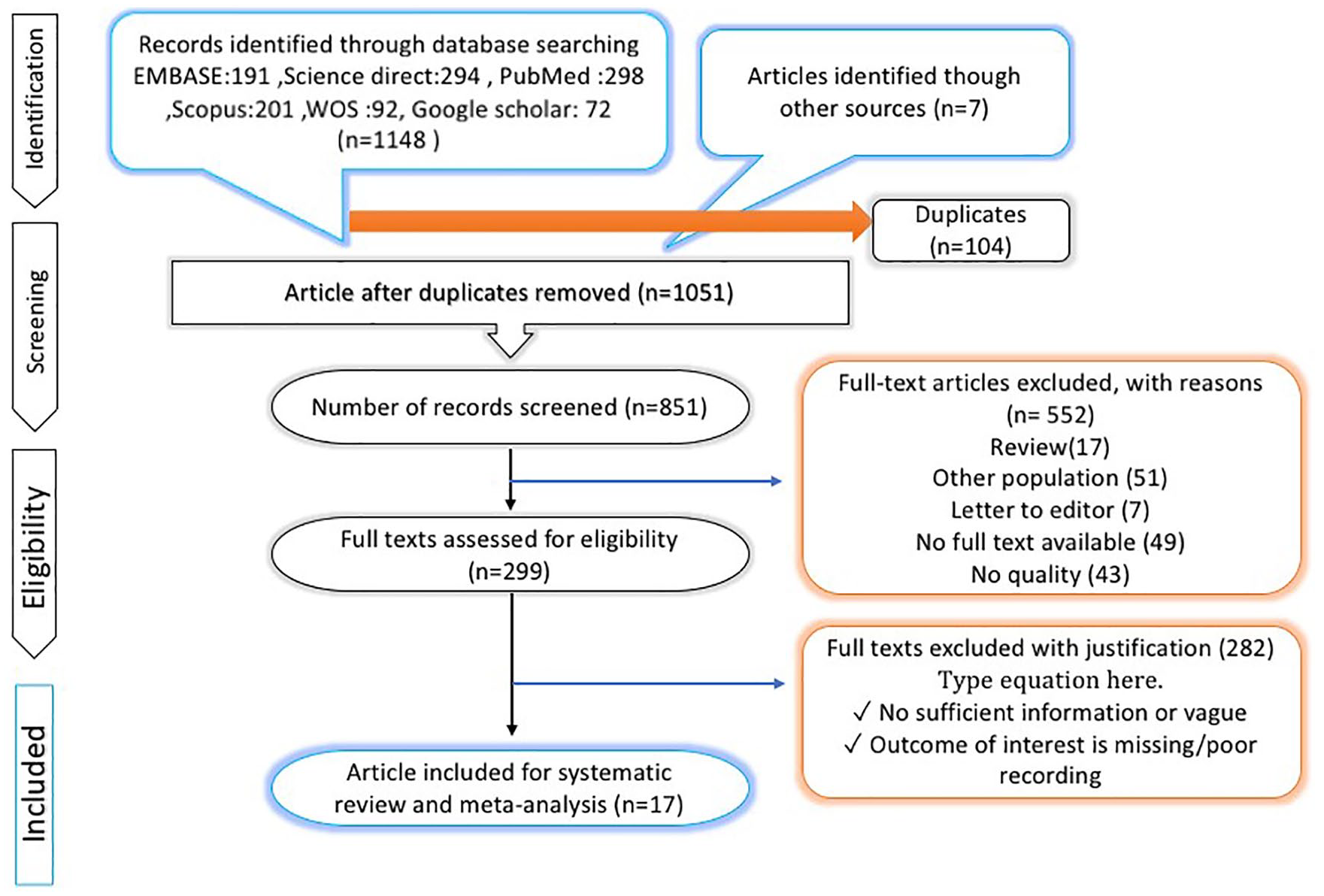
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.
Characteristics of the Selected Studies
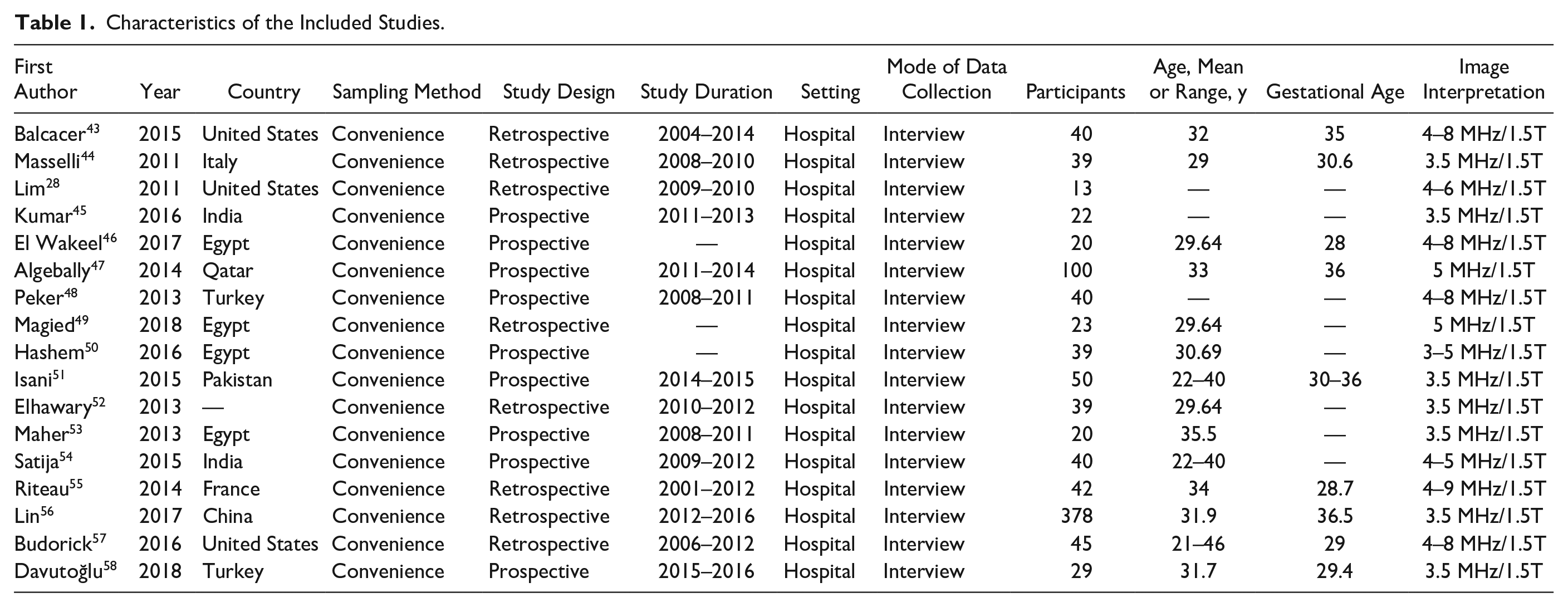
The characteristics of each selected study are shown in Table 1. Overall, 1506 patients (1506 pregnant women at risk of placental invasion) were studied in 17 studies. Of these 17 studies, 5 (29.4%) study were retrospective and 12 (70.6%) study were prospective. The study population included the pregnant women at risk of placental invasion. The patients ranged in age from 16 to 47 years. An experienced radiologist and, in most cases, an experienced radiology fellow evaluated the sonographic and MRI images that were provided with all the studies.
Characteristics of the Included Studies.
Risk of Bias
The evaluation findings of QUADAS-2 are shown in Figure 2. The findings indicate that there was a risk of bias of evaluation for one parameter (random sequence generation [selection bias]). These published studies had certain limitations to their findings (Figures 3 and 4).
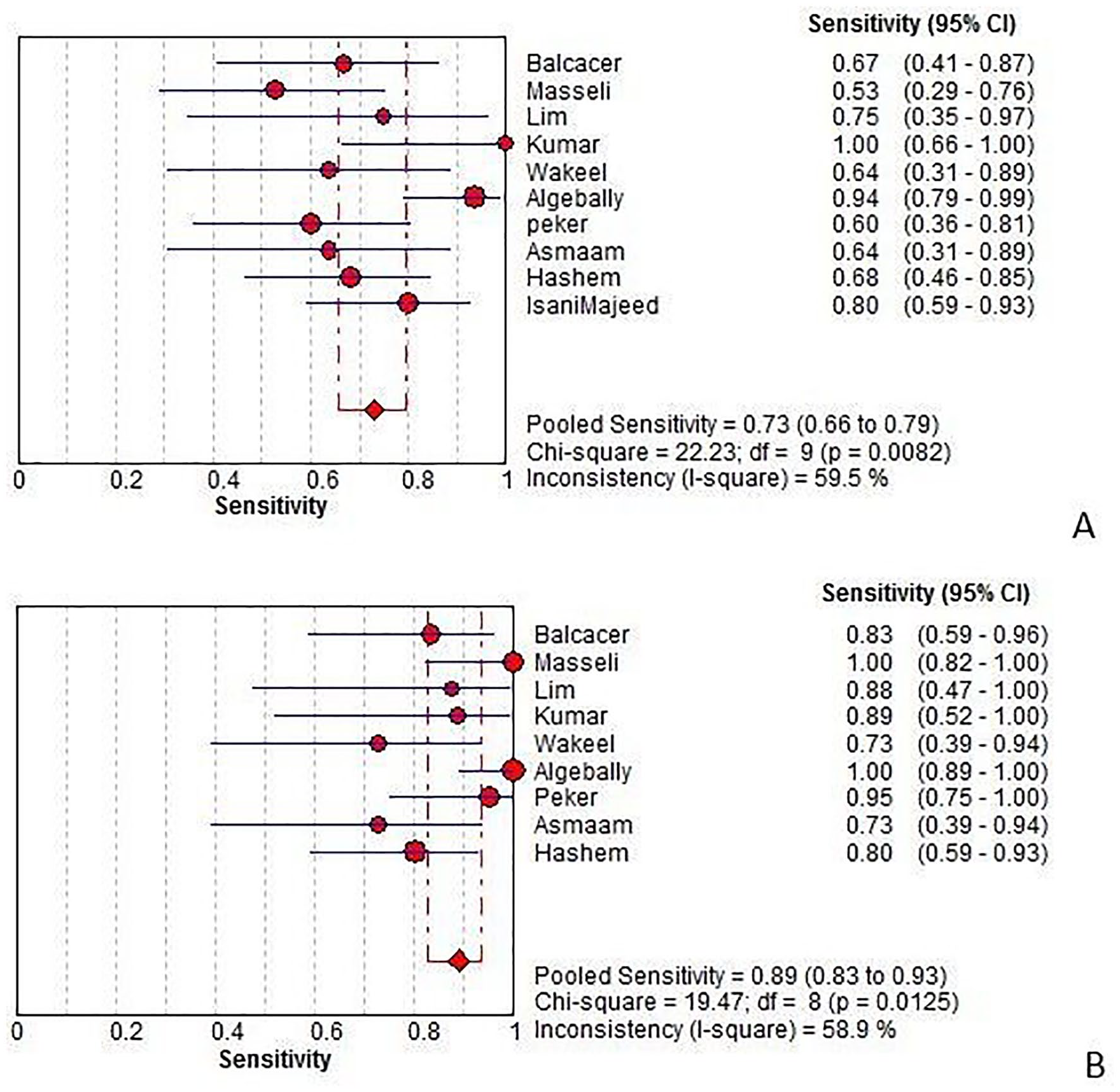
Sensitivity of ultrasonography (A) and magnetic resonance imaging (B) for diagnosing placental invasion. Forest plot of sensitivity reported in each study. Each study is identified by name of first author and year of publication, with circles representing individual study point estimates, size of each circle indicating relative contribution to data pooling (inverse variance weighting), horizontal lines indicating 95% confidence intervals (CIs), and dashed vertical lines representing 95% CIs for pooled sensitivity and specificity.
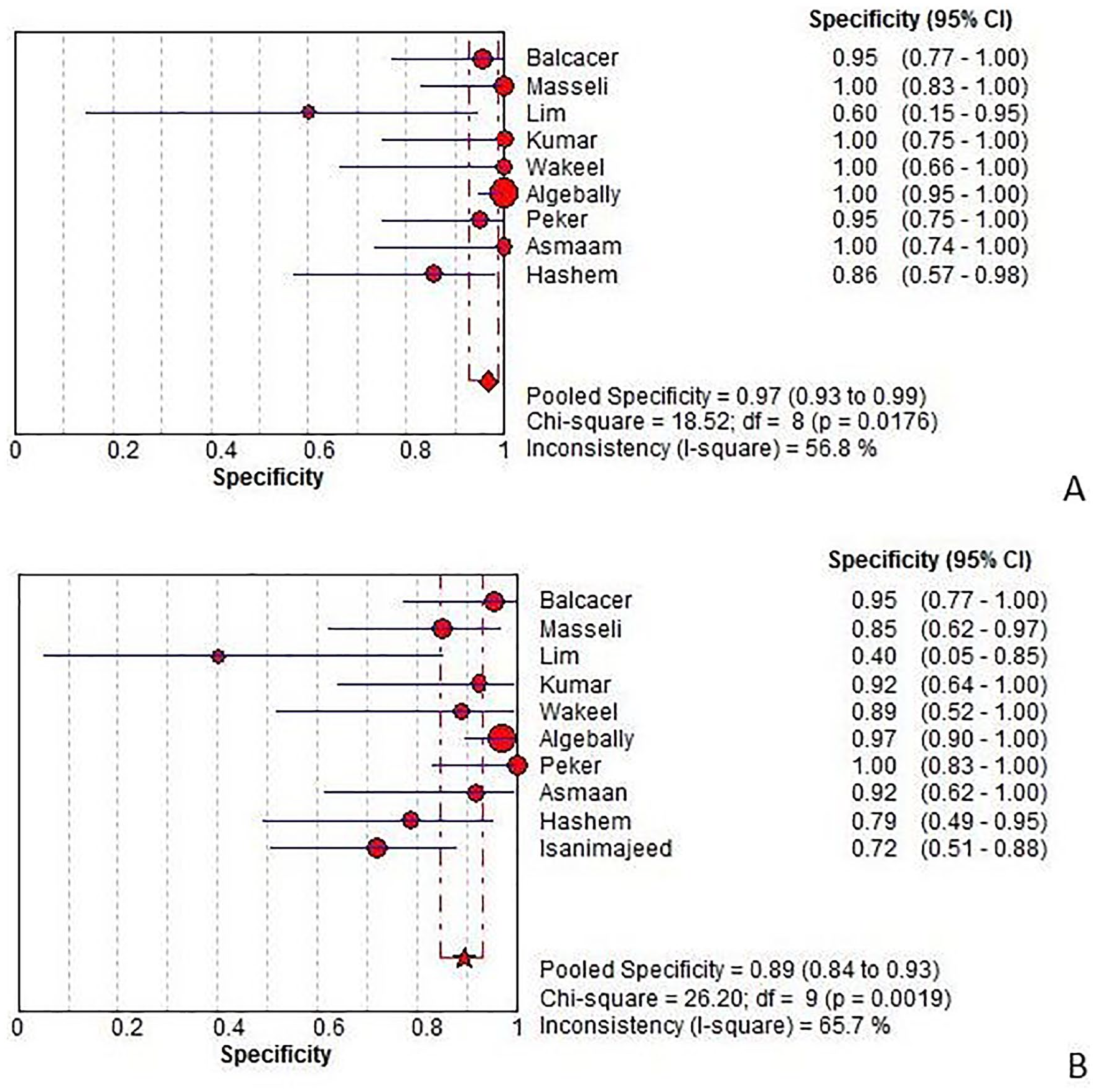
Specificity of magnetic resonance imaging (A) and ultrasonography (B) for diagnosing placental invasion. Forest plots of specificity reported in each study. Each study is identified by name of first author and year of publication, with circles representing individual study point estimates, size of each circle indicating relative contribution to data pooling (inverse variance weighting), horizontal lines indicating 95% confidence intervals (CIs), and dashed vertical lines representing 95% CIs for pooled specificity.
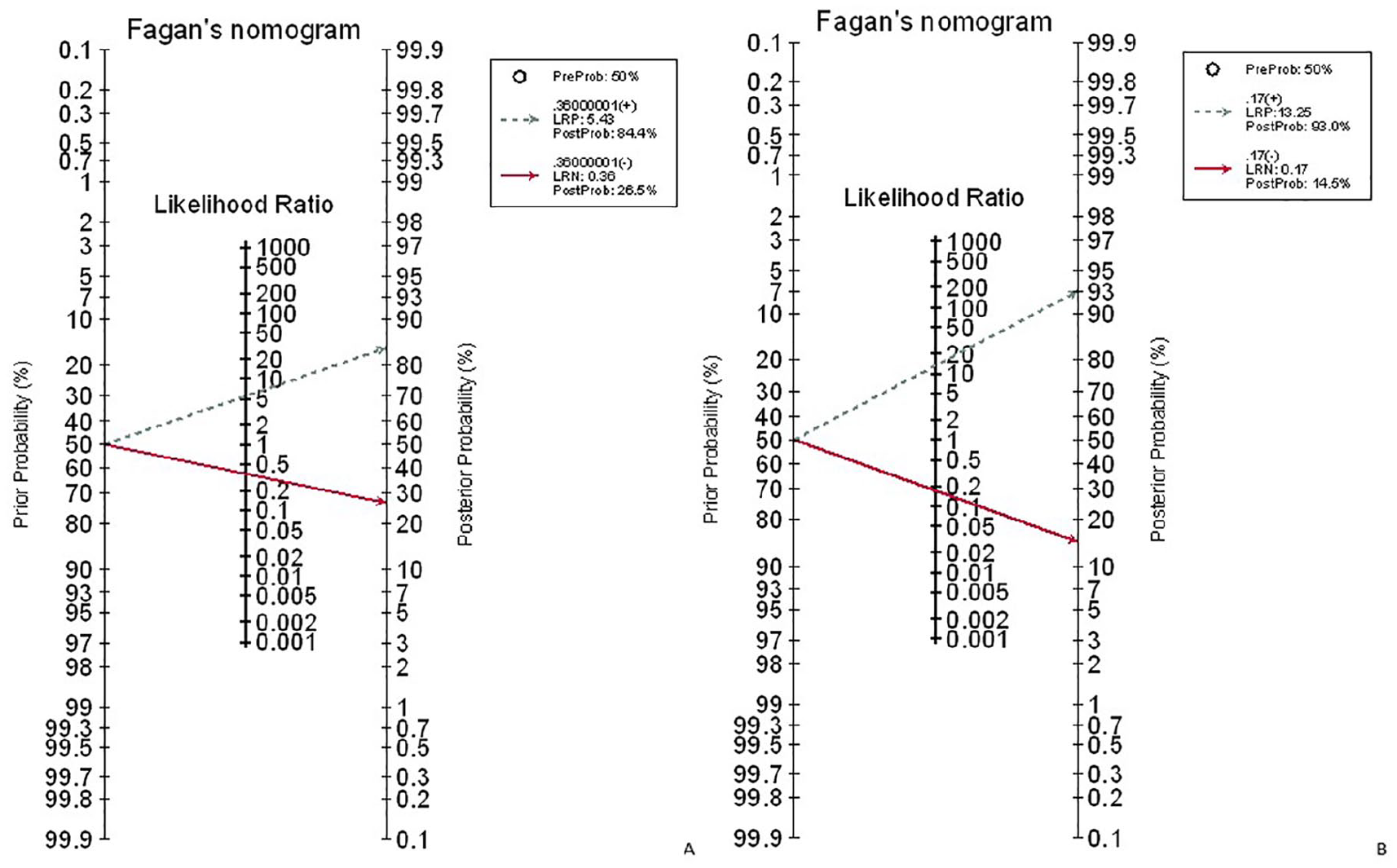
Fagan’s nomogram for the calculation of posttest probabilities. A pretest probability of 50% for placental invasion was fixed, which was estimated by the number of cases in selected studies. (A) ultrasound had a posttest probability of 84.4%. For MRI (B), posttest probability was 93%; that is, with an estimated prevalence of 50%, if this patient tests positive, the posttest probability that she truly has placental invasion would be 93% (solid line in red). On the other hand, if patient tests negative, the posttest probability that she truly has placental invasion would be 26.5% (A) or 14% (B) (blue dotted line). The results were obtained by the following calculations: pretest odds = prevalence/1 – prevalence; posttest odds = pretest odds × LR– (LR + ); posttest probability = posttest odds/1 + posttest odds. LR, likelihood ratio.
Meta-analysis: Diagnostic Accuracy of MRI and Ultrasound to Detect Placental Invasion
MRI for the detection of placental invasion
For placental invasion, the sensitivity and specificity of MRI were 89% (95% CI, 83%–93%) and 97% (95% CI, 93%–99%), respectively. The diagnostic odds ratio was 106.41 (95% CI, 31.31–361.6). The summary ROC (SROC) diagram demonstrated a summary of the estimated sensitivity and specificity. The area below the SROC curve for MRI demonstrated placental invasion in pregnant women with a high-risk pregnancy (Figures 3–6). The positive and negative LRs for MRI in detecting placental invasion in pregnant women with a high-risk pregnancy were 13.25 (4.85–36.2) and 0.17 (0.09–0.31), respectively (Figure 7). A significant heterogeneity was observed for the specificity (I2 = 48.2%; Cochrane Q = 17.38; P < 0.0431) and sensitivity (I2 = 59.8%; Cochrane Q = 22.39; P < 0.0077).
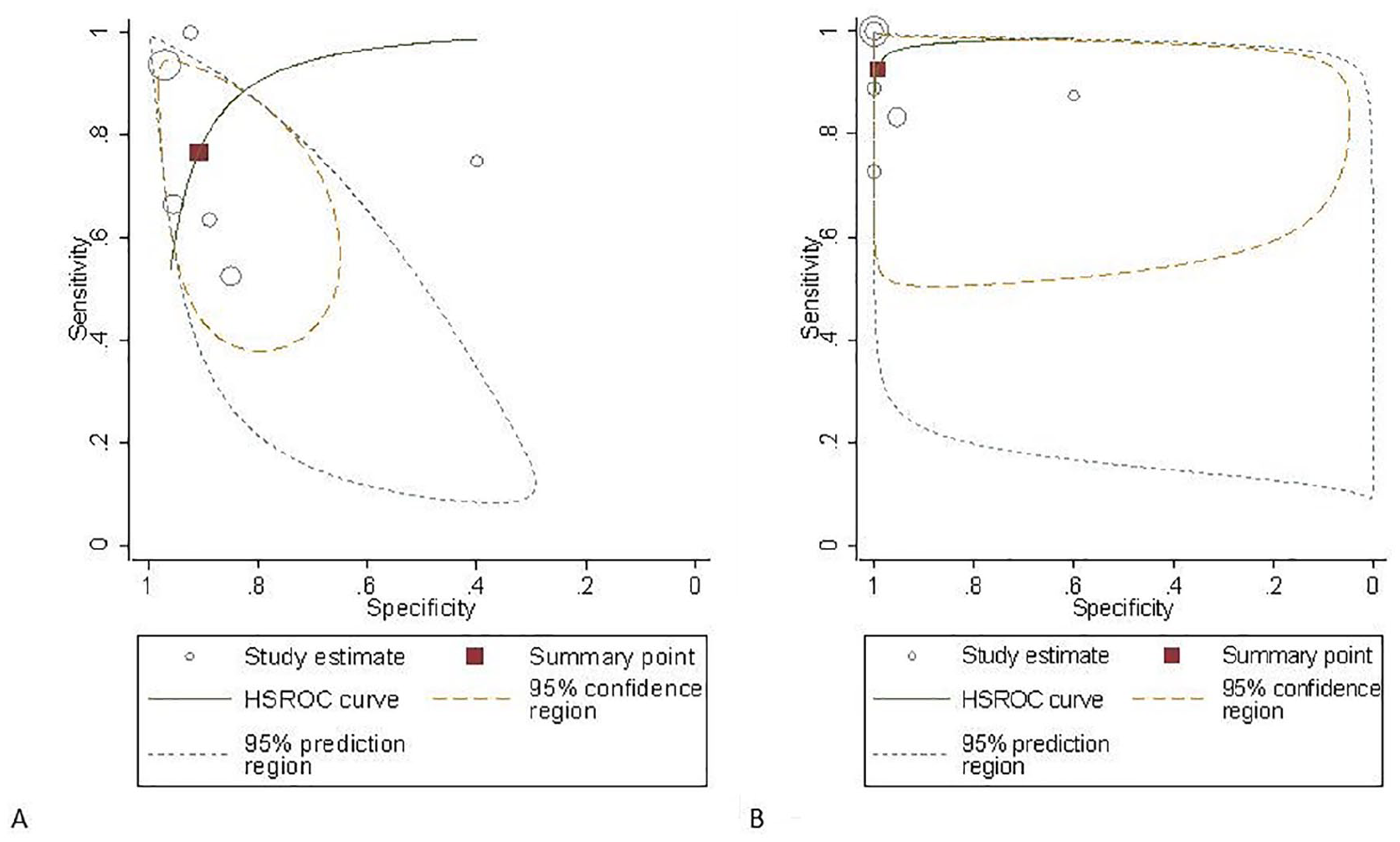
Hierarchical summary receiver operating characteristic (HSROC) curve of magnetic resonance imaging (A) and ultrasonography (B) for the diagnosis of placental invasion.
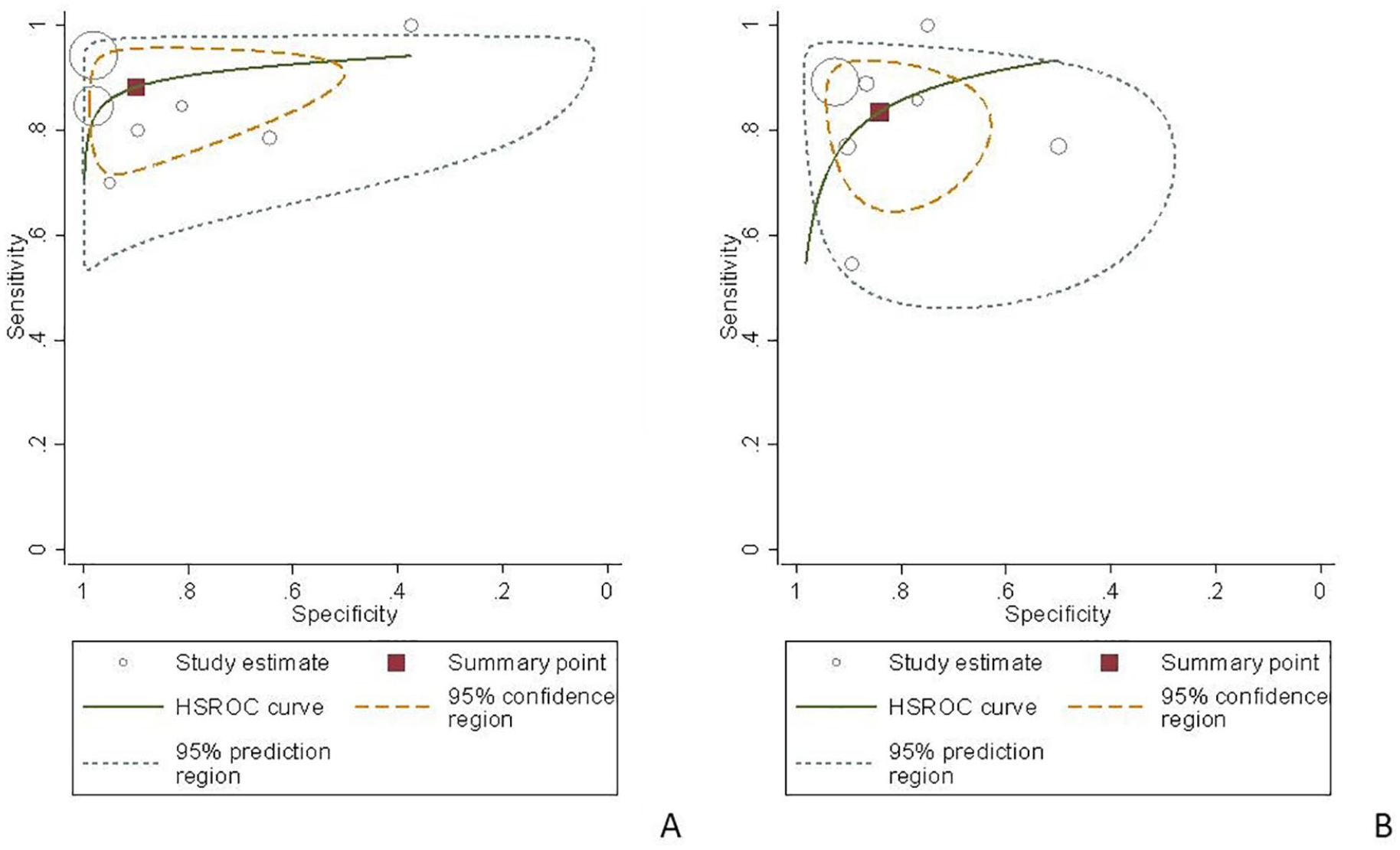
Hierarchical summary receiver operating characteristic (HSROC) curve of magnetic resonance imaging (A) and ultrasonography (B) for the diagnosis of placental accreta.
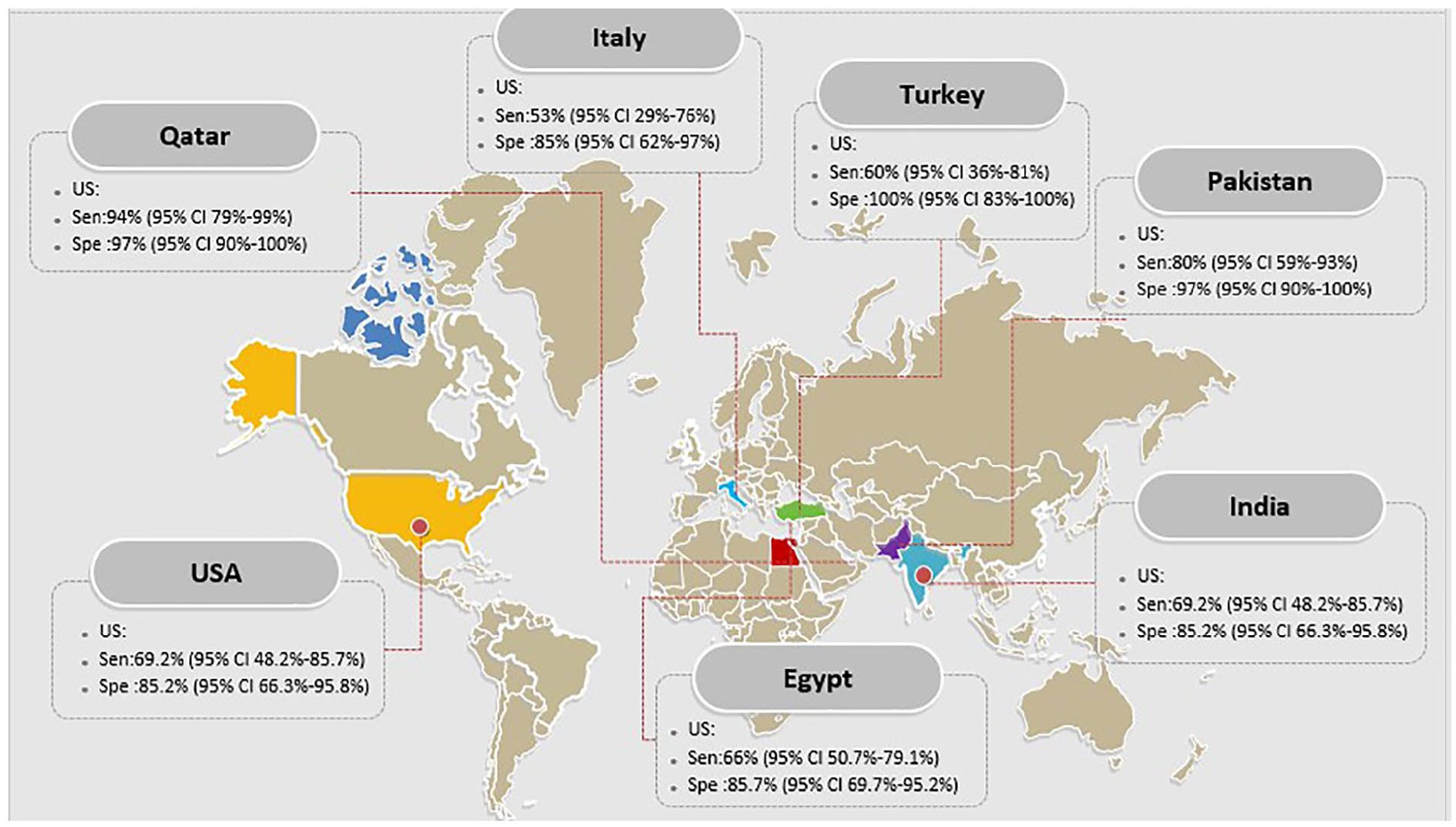
The sensitivity and specificity of ultrasound in diagnosis of placental invasion based on countries.
US for the detection of placental invasion
For placental invasion, the sensitivity and specificity of US were 73% (95% CI, 66%–79%) and 89% (95% CI, 84%–93%), respectively. The diagnostic odds ratio was 20.10 (95% CI, 7.55–53.53). The SROC diagram demonstrated a summary of the estimated sensitivity and specificity (Table 2). The area below the SROC curve, for US, detected placental invasion in pregnant women with a high-risk pregnancy (Figures 3–6). The positive and negative LRs for US in detecting placental invasion in pregnant women with a high-risk pregnancy were 2.86 (1.48–5.52) and 0.28 (0.12–0.63), respectively (Figure 7). A significant heterogeneity was observed for the specificity (I2 = 65.7%; Cochrane Q = 26.20; P < 0.0019) and sensitivity (I2 = 59.5%; Cochrane Q = 22.23; P < 0.001). The forest plot for the specificity and sensitivity are shown in Figures 3 and 4.
Summary Sensitivity, Specificity, and Receiver Operating Characteristic Plot of Ultrasonography in Detecting Placental Invasion.
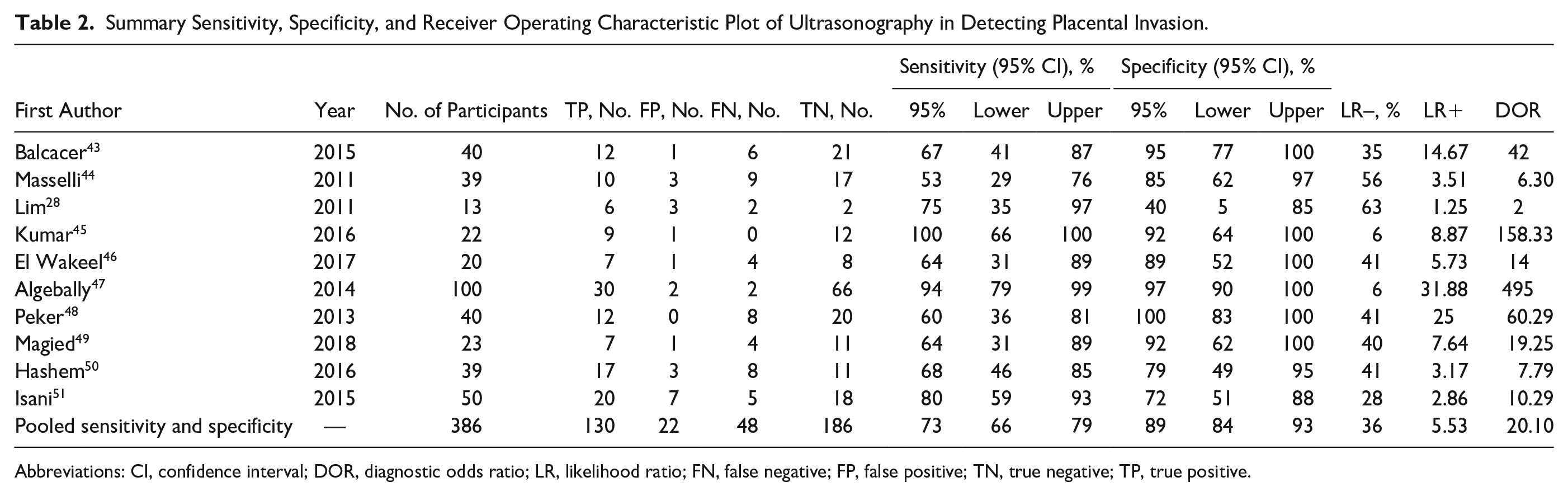
Abbreviations: CI, confidence interval; DOR, diagnostic odds ratio; LR, likelihood ratio; FN, false negative; FP, false positive; TN, true negative; TP, true positive.
The results of meta-regression showed that none of the evaluated variables (see above) explained the heterogeneity. The summary curve of the receiver system performance characteristic for the diagnostic performance of US and MRI in detecting placental invasion is shown in Figure 5. The Fagan nomogram shows that the US diagnosis of suspected of embryonic placental involvement increases the probability of predicting placental invasion. The probability moves from 50% to 84.4%, while the normal US finding decreases the pretest probability from 50% to 26.6% (Figure 7A). Also, an MRI diagnosis of suspected embryonic placental involvement increases the probability of predicting placental invasion from 50% to 93%. The normal MRI diagnostic finding decreases the pretest probability from 50% to 14.5% (Figure 7B).
Subgroup Analysis
US and MRI for the detection of placental accreta
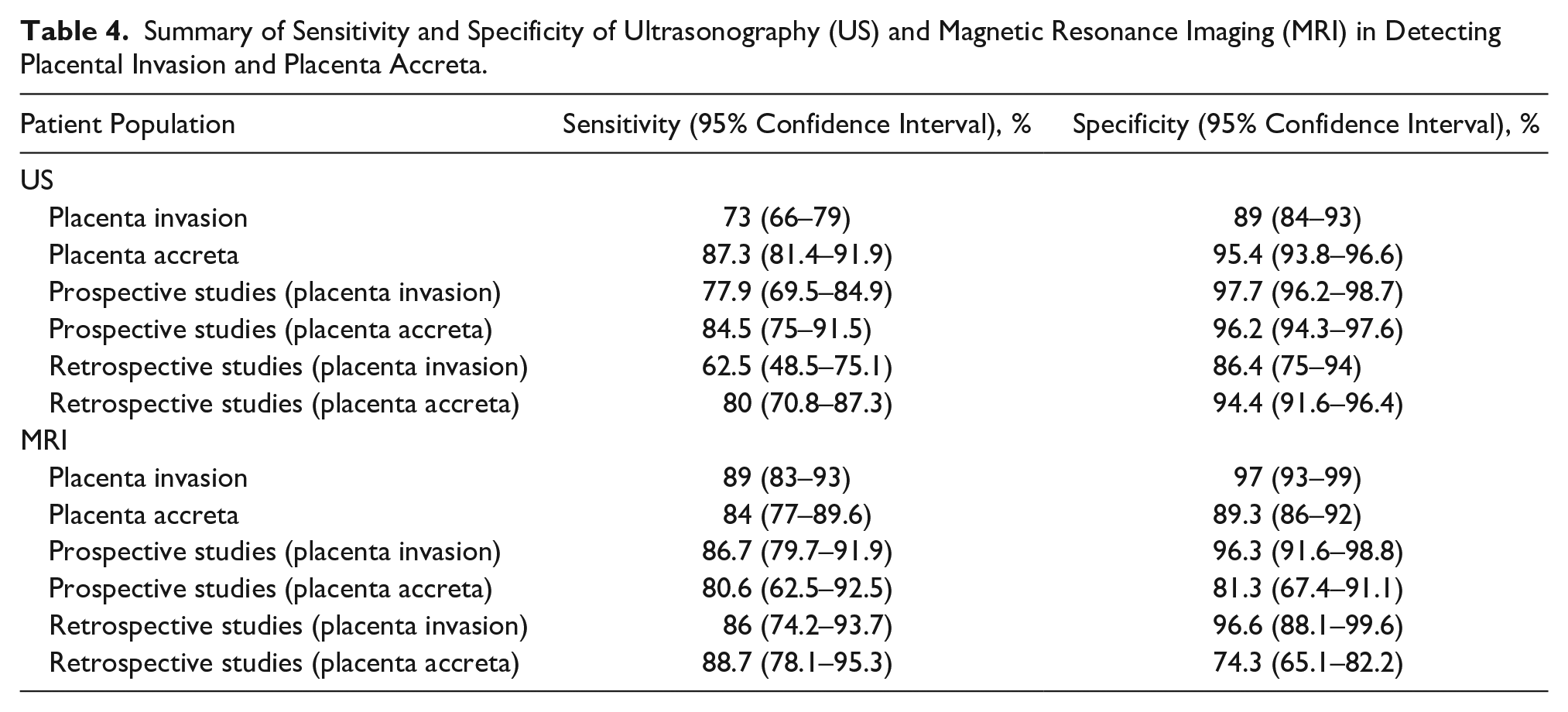
In the detection of placenta accreta solely (as the first grade of placental invasion), the sensitivity and specificity of MRI were 89.3% (95% CI, 86%–92%) and 84% (95% CI, 77%–89.6%). The sensitivity and specificity of US were 95.4% (95% CI, 93.8%–96.6%) and 87.3% (95% CI, 81.4%–91.9%), respectively. The diagnostic odds ratio was 61.261% (95% CI, 14.350%–261.52%). This would indicate a high accuracy of MRI and US in detecting placenta accreta in pregnant women with a high-risk pregnancy (see Table 3). The SROC diagram shows a summary of the estimated sensitivity and specificity and area below the SROC curve for US and MRI in detecting placenta accreta in pregnant women with a high-risk pregnancy (see Figure 6). The positive LRs for US and MRI in detecting placental accreta in pregnant women with a high-risk pregnancy were 8.502 (2.266–31.898) and 4.872 (2.311–10.268), respectively. The negative LRs for US and MRI in detecting placenta accreta in pregnant women with a high-risk pregnancy were 0.185 (0.117–0.294) and 0.234 (0.116–0.473), respectively (see Figure 7).
Summary Sensitivity, Specificity, and Receiver Operating Characteristic Plot of Magnetic Resonance Imaging in Detecting Placental Invasion.
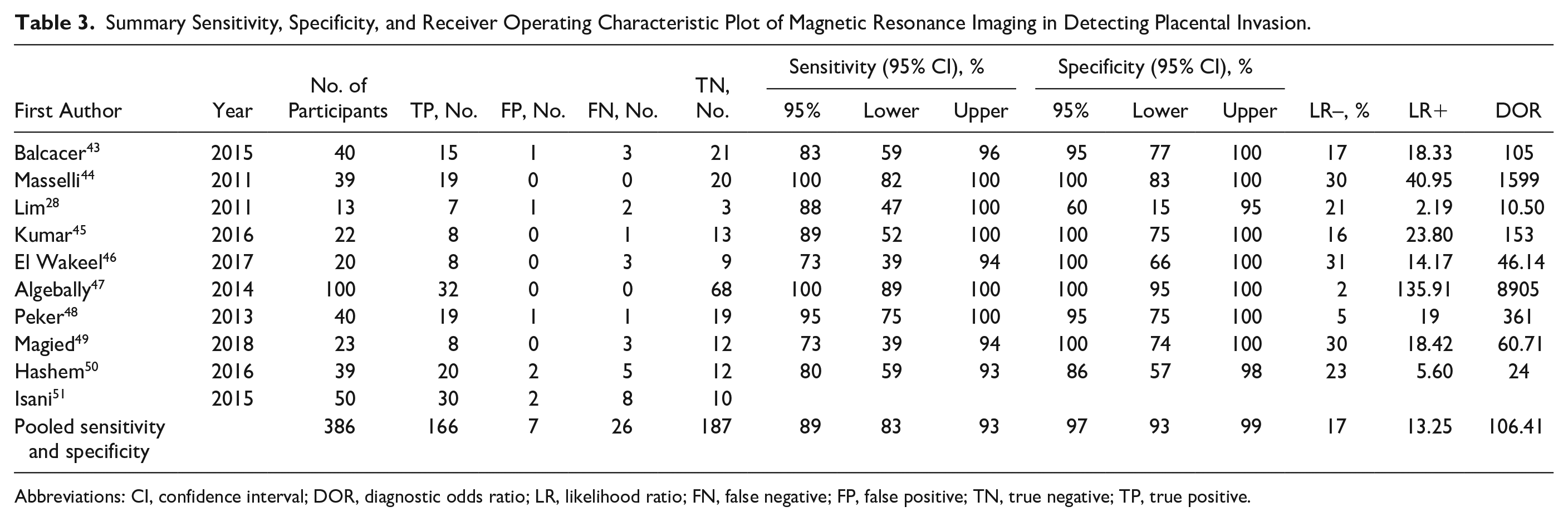
Abbreviations: CI, confidence interval; DOR, diagnostic odds ratio; LR, likelihood ratio; FN, false negative; FP, false positive; TN, true negative; TP, true positive.
Prospective and Retrospective Studies
In total, six studies were prospective and seven studies were retrospective. Among those studies reviewed, four prospective and six retrospective reports provided data on a US diagnosis.
For US, the combined sensitivity for the prospective studies was 0.92% (95% CI, 0.81%– 0.99%), and for the retrospective ones, it was 0.87% (95% CI, 0.75%–0.96%). There was no significant difference between the subgroups reviewed and was equal to P = .49. However, for MRI, the combined sensitivity for the prospective studies was 0.93% (95% CI, 0.78%–1.00%). The retrospective MRI studies were 0.90% (95% CI, 0.79%–0.98%) and the difference between the subgroups was equal to P = .76 (see Table 4).
Summary of Sensitivity and Specificity of Ultrasonography (US) and Magnetic Resonance Imaging (MRI) in Detecting Placental Invasion and Placenta Accreta.
Country of Research Origin
The combined sensitivity and specificity for three Egyptian studies and two US studies for MRI and US in detecting placental invasion during a high-risk pregnancy were 66% (95% CI, 50.7%–79.1%), 85.7% (95% CI, 69.7%–95.2%), and 69.2% (95% CI, 48.2%–85.7%), and 85.2% (95% CI, 66.3%–95.8%). The research that originated from Qatar, Italy, and Turkey had the most sensitivity and specificity in detecting placental invasion during a high-risk pregnancy, by comparison (see Figures 8 and 9).
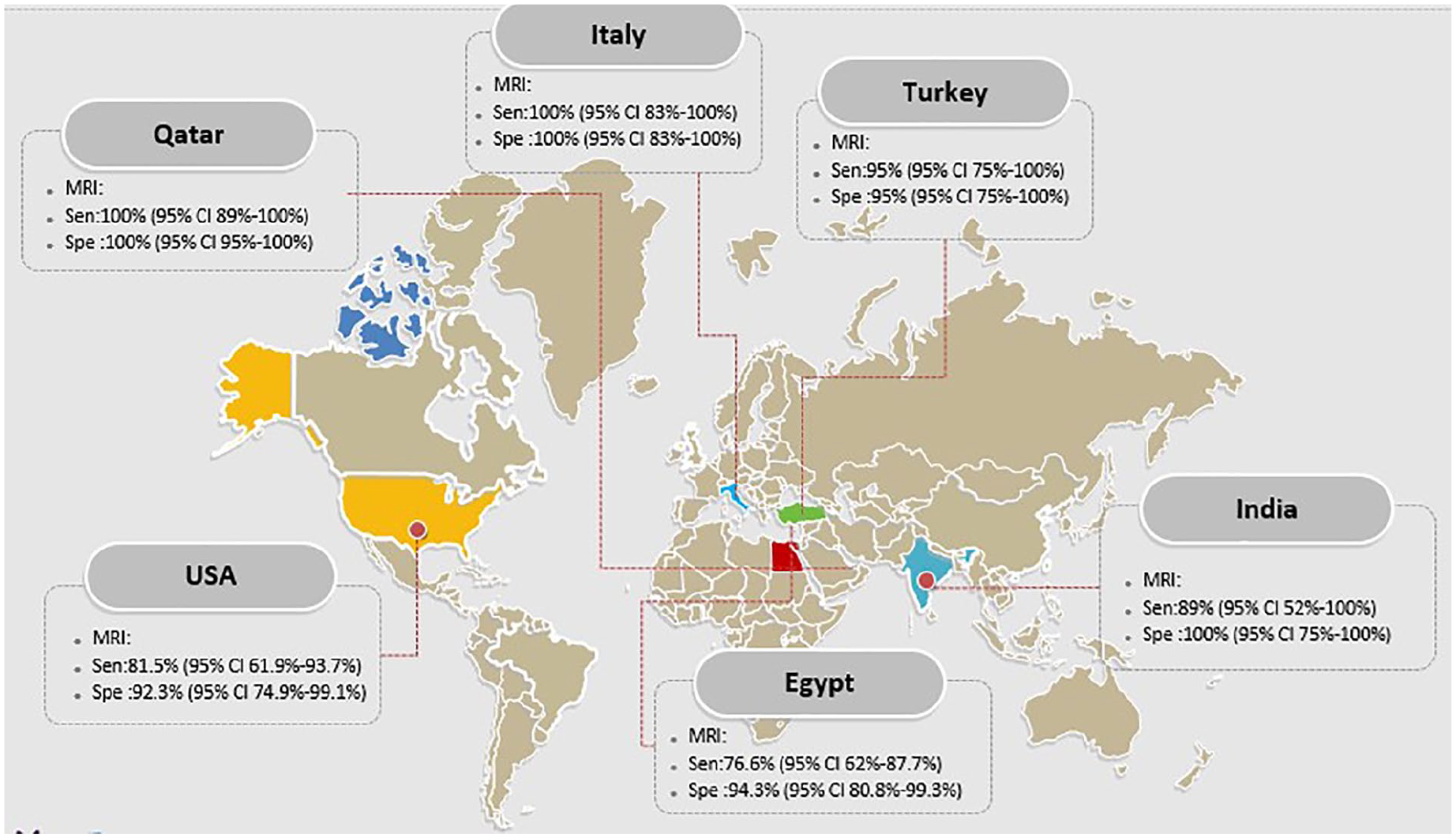
The sensitivity and specificity of MRI in diagnosis of placental invasion based on countries.
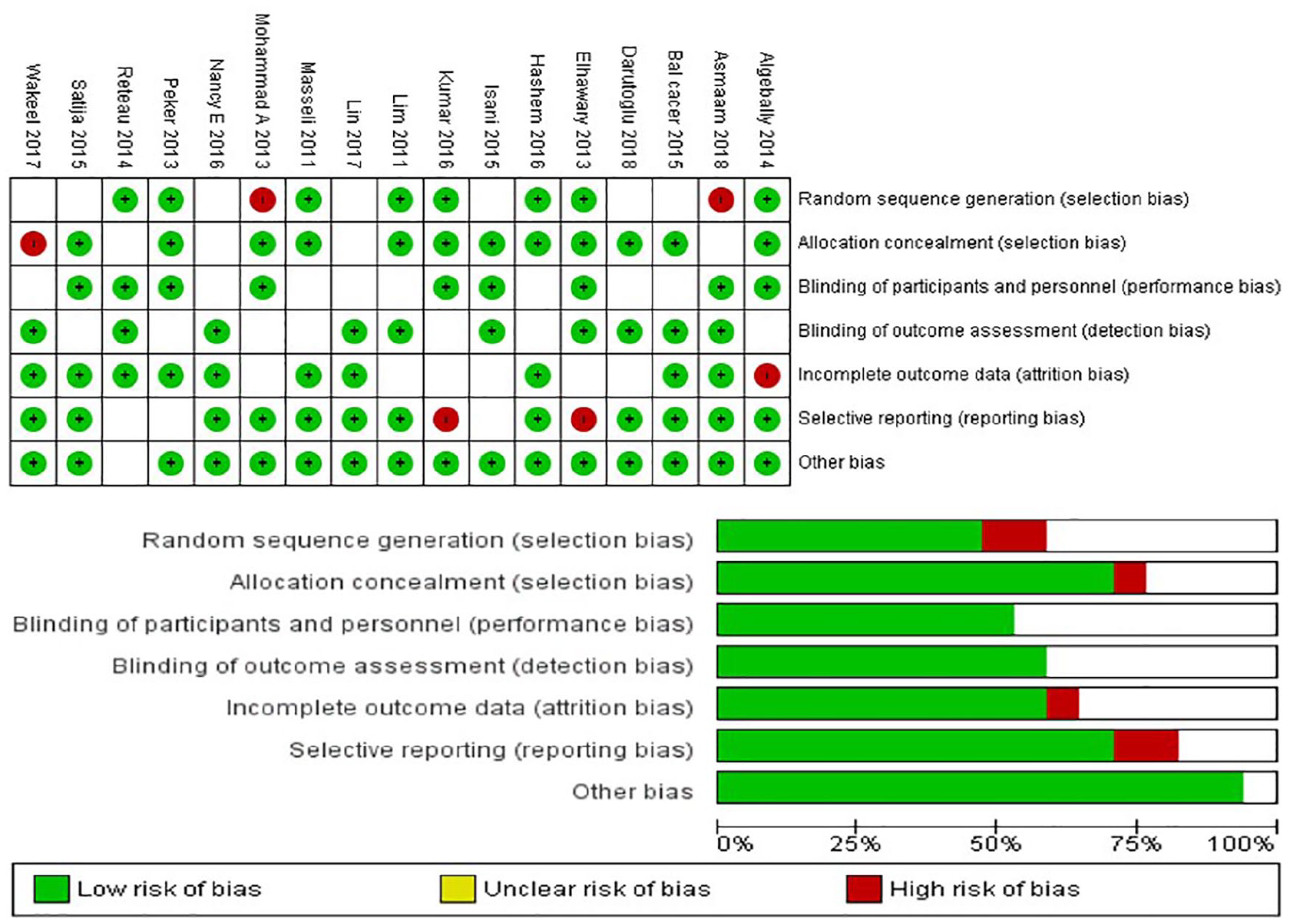
The risk of bias in the studies conducted was measured by using the Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) tool. The risk of bias shown in equation 2 of the above imaging model (magnetic resonance imaging) of each diagram indicates the number and percentage of studies with high (red), medium (yellow), and low (green) risk of bias in four groups of the QUADAS-2 tool.
Discussion
This systematic review and meta-analysis used the term placenta accreta to describe a single pathologic entity, as well as a generic term for the disease spectrum. Used singly, a placenta accreta (vera) occurs if the placenta attaches to but does not invade into the myometrium. If the placenta invades into the myometrium but not beyond, the placenta is described as a placenta increta. When the placenta invades through the serosal layer and potentially beyond, the term placenta percreta is used. Because unexpected placental accreta disorders can lead to severe blood loss, associated complications, and even maternal death, accurate prenatal diagnosis is essential. If these conditions are detected before delivery, a safer surgery can be done given the amount of blood loss. It would be important to secure the presence of anesthesiologists, gynecologic surgeons, and radiologists to work together to reduce bleeding by blocking the iliac arteries in cases of severe hemorrhage. As shown in the previous studies, there was a significant relationship between the number of previous cesarean sections and the rate of placental invasion, as well a higher prevalence of placental invasion with placenta previa.28,29
US has always been the first diagnostic tool for detecting the abnormal placental implantation, which is cost-effective and easily accessible.9,30 The sensitivity and specificity of US in detecting placental invasion, based on this systematic review and meta-analysis, were 73% (95% CI, 66%–79%) and 89% (95% CI, 84%–93%), respectively. Lu et al. 31 reported a sensitivity of 78% (95% CI, 74%–81%) and a specificity of 94% (95% CI, 93%–95%) for US in the detection of placental invasion. In the meta-analysis performed by Meng et al., 32 their sensitivity and specificity for US, in the detection of placental invasion, was 83% (95% CI, 77%–88%) and 95% (95% CI, 93%–96%), respectively.
However, US diagnostic findings have the following problems:
They may not be accurate in posterior placenta patient cases. 33
There is no evidence that US estimates the rate of placental invasion accurately through the myometrium. 34
There is an inability to report the topography of placental invasion accurately through the myometrium. 17
Some studies have also shown that MRI not only optimizes the diagnostic accuracy of US in cases of suspected placental invasion but can also be used as a surgical staging technique. This has the potential for planning a surgery under safer conditions and protects the uterus, with minimal complications.19,35 The sensitivity and specificity of MRI in detecting placental invasion were 89% (95% CI, 83%–93%) and 97% (95% CI, 93%–99%), respectively.
The analysis of SROC curves showed that, interestingly, the AUC for US and MRI was the same and equal to 0.9543 with an index (Q* = 0.8963). These results show that the sensitivity and specificity of US and MRI are exactly the same, and both have high specificity and sensitivity in detecting a placental invasion. In detecting placental accreta, as the first grade of invasion of the placenta, the sensitivity and specificity of MRI were 89.3% (95% CI, 86%–92%) and 84% (95% CI, 77%–89.6%), compared to the sensitivity and specificity of US, which was 95.4% (95% CI, 93.8%–96.6%) and 87.3% (95% CI, 81.4%–91.9%), respectively. This demonstrates the relatively better performance of US in the early stages of placental invasion. Early studies have shown that MRI is superior to US alone in evaluating posterior placenta.30,36 Other studies have shown that these methods are comparable and complementary, because while one imaging result may be ambiguous, the complementary imaging result yields accurate results. The use of MRI has increased for those patients suspected of having a placental anomaly. This may be due to some studies demonstrating that MRI results can alter the usual diagnostic and surgical methods in cases of placental percreta. This has the effect of reducing bleeding and disease.37,38 Given that the data were inadequate, the current analysis was unable to evaluate the sensitivity and specificity of MRI and US in placenta increta and percreta separately.
The most sensitive markers of placental invasion in US were the following:
The loss of the retroplacental clear space with a sensitivity of 85.2% and a specificity of 69.6%
The placental lacunae with a sensitivity of 82% and a specificity of 51.3%
The increased intraplacental vascularity with a sensitivity of 52%
The specificity of 85.2% and the loss of the bladder wall echogenicity with a sensitivity of 41.1% and a specificity of 91.8%
In their study, Mar et al. 39 reported that placental lacunae are the most sensitive marker with the highest positive predictive value (PPV) for placental accreta. Since the retroplacental clear space represents the capsular decidua, the uncertainty of the images is due to placental accreta.
However, the loss of the retroplacental clear space is not an accurate diagnostic marker. High false-positive rates of up to 50% have been reported.39,40 It would seem that the most accurate US diagnostic findings were related to placental lacunae.
The most sensitive markers for placental invasion in MRI were as follows:
The loss of retroplacental myometrial mantle with a sensitivity of 78.7% and a specificity of 29.3%
The heterogeneous placenta with a sensitivity of 75.6% and a specificity of 57.55%
The dark intraplacental band with a sensitivity of 75.2% and a specificity of 47.9%
Previous studies have reported that the most useful diagnostic MRI findings are the dark intraplacental band, heterogeneous placenta, and placental bulging, which are consistent with these study findings.10,41,42
Limitations
This study has some limitations with regard to the findings. Since this study is a meta-analysis, the validity of the results depends on the validity of the published studies. In addition, this analysis combined published studies that were clinically and methodologically diverse. As a result, this heterogeneity may cause a bias in the results, which were hard to avoid. An additional set of factors, such as the position of the placenta and the degree of bladder filling, were not investigated. It is also important to note that some factors such as the type and extent of the transducer, contrast agents, and the physician’s experience may have introduced bias in the published article results.
Conclusion
Due to the increased use of cesarean section, placental invasion may be increasing in frequency. The diagnosis of prenatal placental invasion is important to reduce maternal morbidity and mortality. Typically, the first diagnostic examination is done with US for patients suspected of having a placental anomaly. However, recent trends would indicate that MRI may be favored in evaluating placental invasion as a complementary imaging method. The diagnostic interpretation of MRI findings should be accompanied by a compatible US evaluation of the patient. Multiple published imaging results are based on the use of US and MRI for ultimate diagnosis. The most accurate diagnostic US findings are placental lacunae and the dark intraplacental band detected with MRI.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.