
Abstract
We present an unusual case of placental chorangioma in a 32-year-old female with poor antenatal care. Abdominopelvic ultrasound revealed polyhydramnios with no fetal cardiac activity and suspected placental cyst. An emergency caesarean was performed, and she had still birth of male baby. The cut specimen of the placenta revealed a well-circumscribed marginal mass of 4 cm. Our case emphasizes the importance of regular antenatal screening for early detection of placental abnormalities. While chorangiomas are rare, they should be considered in the differential diagnosis of placental masses. Prompt diagnosis and appropriate management are essential to reduce the maternal and fetal complications associated with chorangiomas. Histological examination of the placenta plays a vital role in differentiating chorangioma from other placental abnormalities with different clinical implications.
Introduction
Placental chorangioma, also called as placental haemangioma, is the rare non-trophoblastic benign tumour of the placenta which arises from the primitive chorionic mesenchyme. 1 It has an estimated incidence of 0.6–1%, which is usually diagnosed antenatal on ultrasound imaging. Most of these tumours are of size <5 cm, asymptomatic and most often in women over 30 years of age. They are usually associated with primipara and twin pregnancies. Chorangioma of size >5 cm are called large chorangioma’s and are associated with adverse maternal and fetal complications. 1
Case report
A 32-year-old female, primigravida patient with 36 weeks of gestation presented to gynecological emergency with the premature rupture of membranes (PROM). History revealed poor antenatal care. On general examination, all vitals were normal. Immediately, abdominopelvic ultrasound was performed which revealed polyhydramnios with no fetal cardiac activity and suspected placental cyst.
Routine laboratory investigations revealed haemoglobin – 10gm%, total leucocyte count – 33,000/cm, platelet count – 2.3 lacs/mm3, C-reactive protein – positive. An emergency caesarean was performed and delivered a still birth male baby. Post-operative period was uneventful, patient had normal recovery and discharged on the 7th day after surgery. The placenta along with umbilical cord was sent for histopathological examination. The cut specimen of the placenta revealed a well-circumscribed marginal mass of 4 cm (Figure 1).

Specimen of the placenta with a cut section shows the circumscribed grey-brown area.
Heamatoxylin and eosin stained section revealed the structure of placenta with circumscribed tumour tissue comprising of proliferating fetal capillaries of varying sizes, fibrosis, congestion and haemorrhage (Figure 2). Based on the clinical history, gross and microscopic features, a diagnosis of placental chorangioma was made.
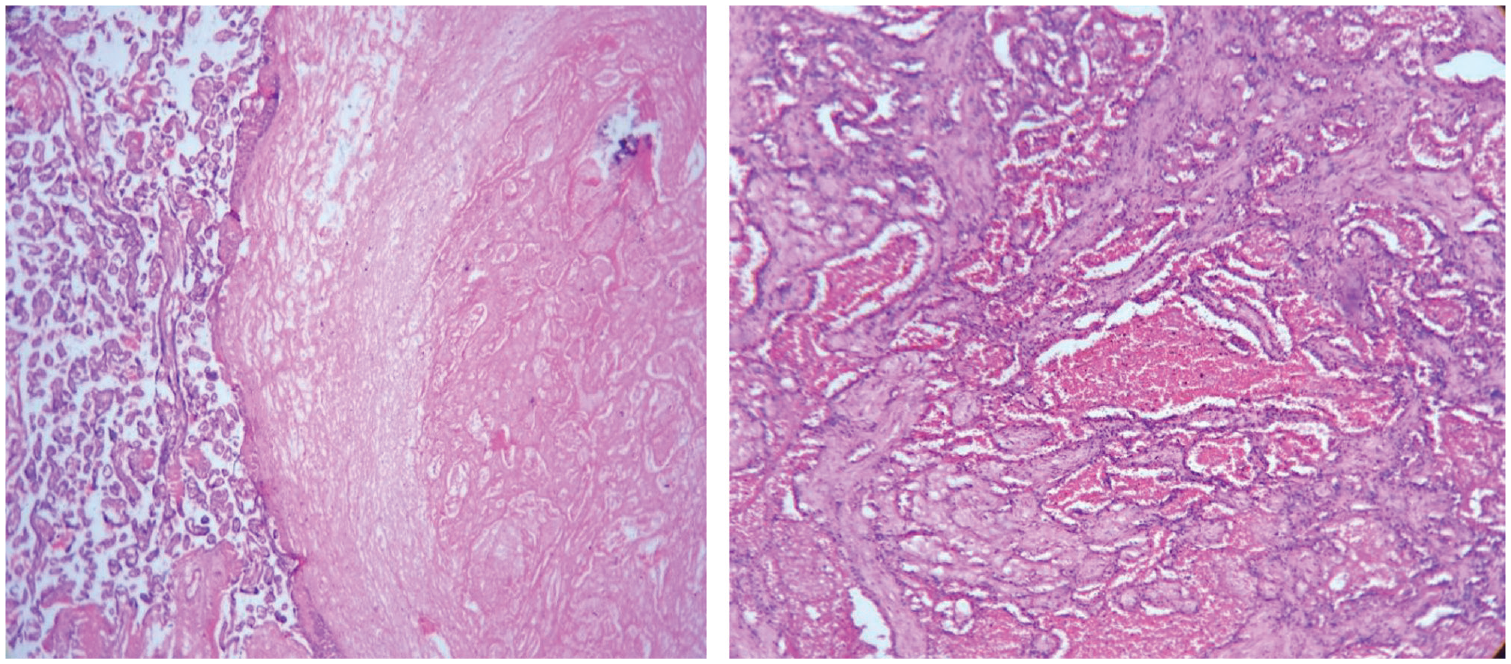
Structure of the placenta with circumscribed tumour tissue comprised of proliferating fetal capillaries of varying sizes, fibrosis, congestion and haemorrhage.
Discussion
Chorangioma, also called as placental haemangioma is a rare non-trophoblastic benign tumour of the placenta characterized by abnormal vascular development within the chorionic mesenchyma with an estimated incidence of 0.6–1% diagnosed antenatal on ultrasound imaging. 2 The differentials on ultrasonography include placental hematoma, degenerating fibroid, placental teratoma and deceased twin. Colour Doppler and magnetic resonance imaging are the other diagnostic tools but may not be always accessable. 3 Chorangiomas are most frequently observed in third trimester of pregnancy as a solitary nodule often in the vicinity of the umbilical cord insertion and incidental finding on antenatal ultrasonography. Grossly, they are single or multiple, well-circumscribed, spherical to oval masses of purplish red tumours with a fleshy appearance or firm as tan-brown if infracted microscopically. They are of three histological subtypes: angiomatus, cellular and degenerate, of which the angiomatous is the most common type and characterized by numerous proliferative blood vessels in various stages of differentiation, from capillary to cavernous types, surrounded by placental stroma. 4 Regarding prognosis, large chorangiomas associated with polyhydramnios lead to high perinatal morbidity and mortality. Treatment modalities include combined use of bipolar cautery with a diode laser. Emergency caesarean section was performed in this case of known intrauterine fetal death (IUFD) due to PROM and absence of fetal cardiac activity. The presence of polyhydramnios and a suspected placental cyst on ultrasound raised concerns about underlying placental pathology. Immediate delivery was crucial to minimize maternal risks and allow evaluation of the placenta. The LSCS facilitated the delivery of the stillborn baby and subsequent examination of the placenta for accurate diagnosis and identification of any contributing factors. Prompt intervention and thorough evaluation are essential in cases of IUFD to ensure appropriate management and prevent potential complications.
In this case, the placental examination revealed a well-circumscribed marginal mass, consistent with a chorangioma. Histological examination of the placenta plays a crucial role in differentiating chorangioma from other placental abnormalities, such as multiple chorangioma or chorangiomatosis, which may have different clinical implications.5,6 Multiple chorangiomas refer to the presence of two or more chorangiomas within the placenta. 5 Chorangiomatosis is a condition characterized by the presence of numerous, widely distributed chorangiomas throughout the placenta. 6 It is important to differentiate between these conditions, as multiple chorangiomas and chorangiomatosis have been associated with a higher risk of adverse fetal outcomes, including intrauterine growth restriction and fetal death. The evaluation of placental sections, careful assessment of the number, distribution and size of chorangiomas, and identification of any additional histopathological features are essential in making an accurate diagnosis.
A comprehensive analysis of the placental pathology, along with clinical history and other relevant investigations, is necessary to determine the underlying cause of IUFD. To improve the accuracy of diagnosis and understand the factors contributing to fetal death, advanced investigations such as immunohistochemistry, molecular studies or additional imaging modalities can be utilized. 7 These tools may help in identifying specific markers, genetic abnormalities or vascular characteristics associated with certain placental abnormalities, aiding in the differential diagnosis and better elucidating the pathogenesis of fetal demise.
Conclusion
In conclusion, we presented an unusual case of placental chorangioma in a patient with poor antenatal care, leading to IUFD. Our case emphasizes the importance of regular antenatal screening for early detection of placental abnormalities. While chorangiomas are rare, they should be considered in the differential diagnosis of placental masses. Prompt diagnosis and appropriate management are essential to reduce the maternal and fetal complications associated with large chorangiomas. Additionally, histological examination of the placenta plays a vital role in differentiating chorangioma from other placental abnormalities with different clinical implications.
Footnotes
Acknowledgements
Sincere thanks to Squad Medicine and Research for their support and guidance.
Author contributions
KKD and SKK involved in conception or design of the work. KKD, SKK, STC and TKS involved in first draft of the article. TKS and VT involved in critical revision of the article. KKD and VT involved in supervision of article. KKD, SKK, STC, TKS and VT involved in final approval of the version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.