
Abstract
Hemopneumothorax is a rare but serious complication that can occur in patients with central venous catheters, trauma, or underlying lung disease. It involves the accumulation of blood and air in the pleural cavity, which can cause hypovolemic shock if left untreated. Lung sonography is a noninvasive, nonionizing radiation imaging technique, and easily accessible diagnostic tool that can be performed at the bedside in critically ill patients, for the diagnosis of hemopneumothorax. A case is reported of a 60-year-old female with a medical history of leukemia who developed hypovolemic shock due to right hemothorax caused by a perforation of the superior vena cava by a central venous catheter. The patient underwent emergency surgery and her condition improved, but later presented with symptoms of hemopneumothorax, which was diagnosed using lung sonography. Emergency placement of a pleural drainage tube was performed, but unfortunately, the patient’s condition deteriorated, and she received end-of-life care. Prompt diagnosis and management of hemopneumothorax are essential to prevent life-threatening complications, and lung sonography is a valuable diagnostic tool, in the diagnosis of critically ill patients.
The occurrence of hemothorax, which can be accompanied by a pneumothorax, in critically ill patients, ranges from 1.0% to 3.4%. Within the intensive care unit (ICU) setting, hemothorax can arise from iatrogenic or spontaneous causes. Venous bleeding resulting from procedures such as thoracocentesis, pleural biopsy, chest tube placement, or central venous catheterization is the primary cause of hemothorax, in the medical ICU. 1 Conversely spontaneous hemothorax is infrequent. Several studies have reported additional complications associated with spontaneous hemothorax, including malignancy, anticoagulation therapy, and thrombocytopenia.1,2 Lung sonography is a noninvasive, nonionizing radiation imaging technique, and is an easily accessible diagnostic tool that can be performed at the bedside in critically ill patients. It has been shown to be highly sensitive and specific for the diagnosis of pleural effusion, pneumothorax, and hemothorax. 3 The case report describes a patient in which the use of lung sonography enabled the accurate diagnosis of a hemopneumothorax, based on the presence of characteristic diagnostic signs.
Case Report
A 60-year-old female patient with a history of leukemia who was undergoing prolonged hospitalization in the ICU, due to a COVID-19 pneumonia, malignant hypercalcemia, and persistent thrombocytopenia, which required mechanical ventilation. She presented with hypovolemic shock secondary to a right hemothorax. Emergency surgery with video-assisted thoracoscopy was performed, revealing perforation of the superior vena cava by a central venous catheter. Hematoma drainage, pleural decortication, and repair of the superior vena cava lesion were performed, and the patient showed good recovery, leading to the subsequent removal of the right pleural drainage. However, she presented with a decrease in hematocrit in the context of persistent thrombocytopenia.
A lung sonogram was performed using a Philips Healthcare’s (Andover, Mass.) Sparq ultrasound equipment system. A linear transducer was used with an operating frequency of 7 to 12 MHz, as well as a phased array transducer with an operating frequency of 2 to 4 MHz. During the sonographic examination, the standardized points specified in the BLUE-protocol, developed by Lichtenstein, were employed. 4 The positioning of the hands involved placing the little finger of the upper hand just below the clavicle, aligning the fingertips along the middle line, and situating the lower hand just below the upper hand. The midpoint of the upper hand was referred to as the upper BLUE-point, while the middle of the lower palm was identified as the lower BLUE-point. In addition, the determination of the posterolateral alveolar and/or pleural syndrome (PLAPS)-point involved extending a horizontal line from the lower BLUE-point and a vertical line from the posterior axillary line. 5
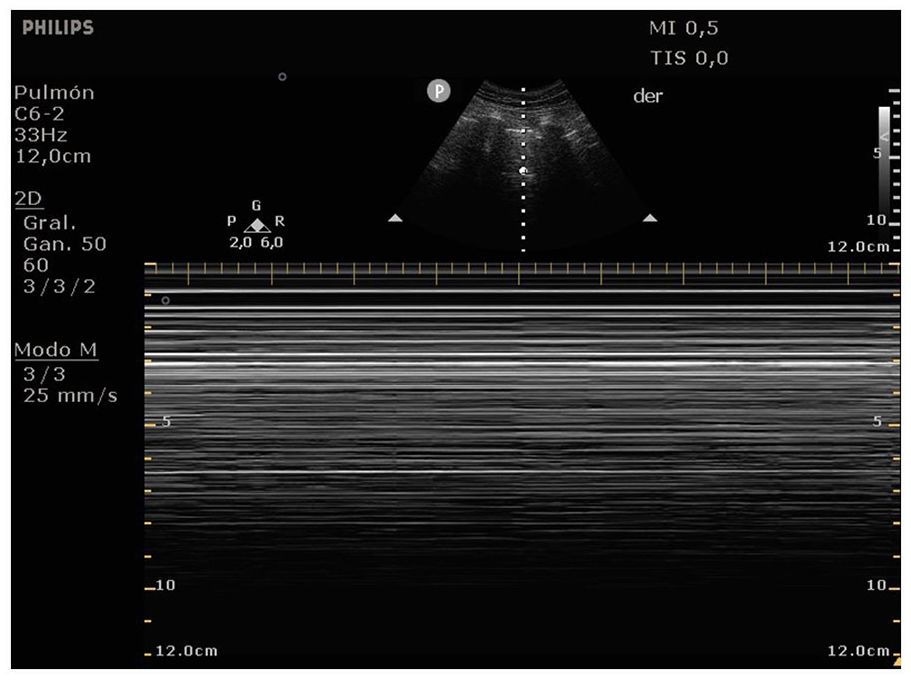
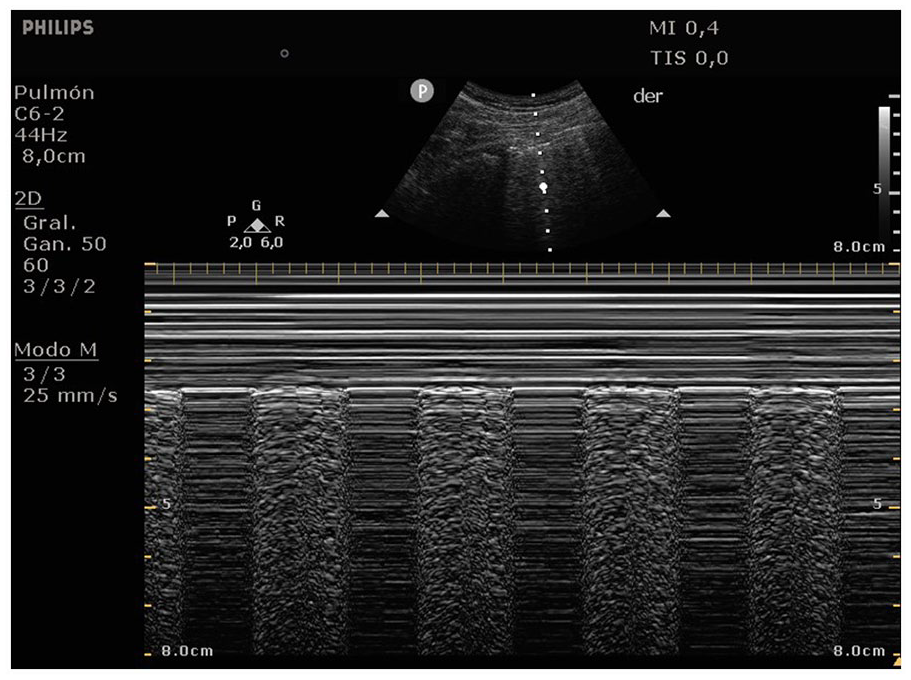
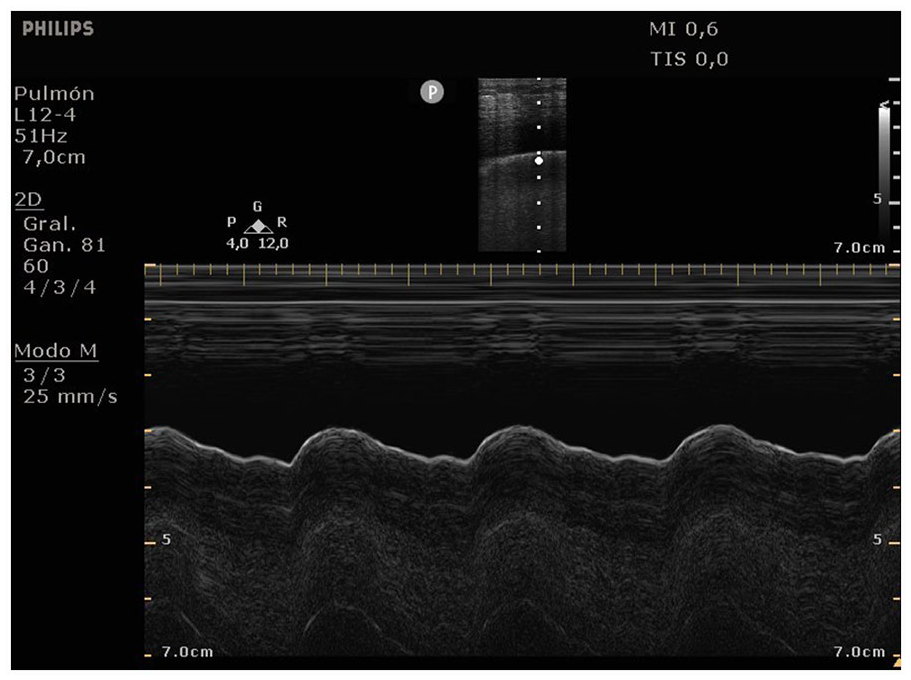
The examination of the right upper BLUE-point using the linear transducer revealed the absence of lung sliding, while the right lower BLUE-point exhibited a distinct pattern of absence of lung sliding, which abruptly transitioned to an anechoic image indicative of pleural effusion, in grayscale. This finding was consistent with the hydropoint sign (see Figure 1). Using the M-mode application, a characteristic pattern was noted as an intermittent barcode sign and an intermittent sinusoid sign (see Figure 2). Furthermore, utilizing a phased array transducer, a significant anechoic image was seen, which was compatible with moderate pleural effusion and detected at the right PLAPS point (see Figure 3). The presence of these diagnostic findings was confirmed with a chest computed tomographic (CT) examination.
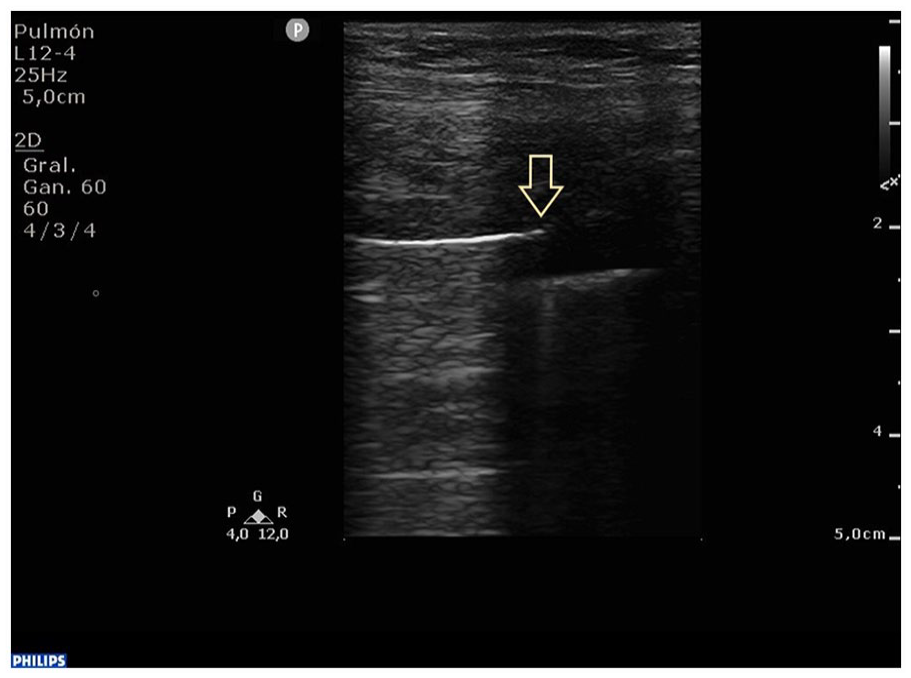
Grayscale lung sonogram obtained using a linear transducer, which highlights the hydropoint sign. This diagnostic sign is characterized by the alternating presence of and anechoic pleural effusion and the absence of lung sliding (see open yellow arrow).
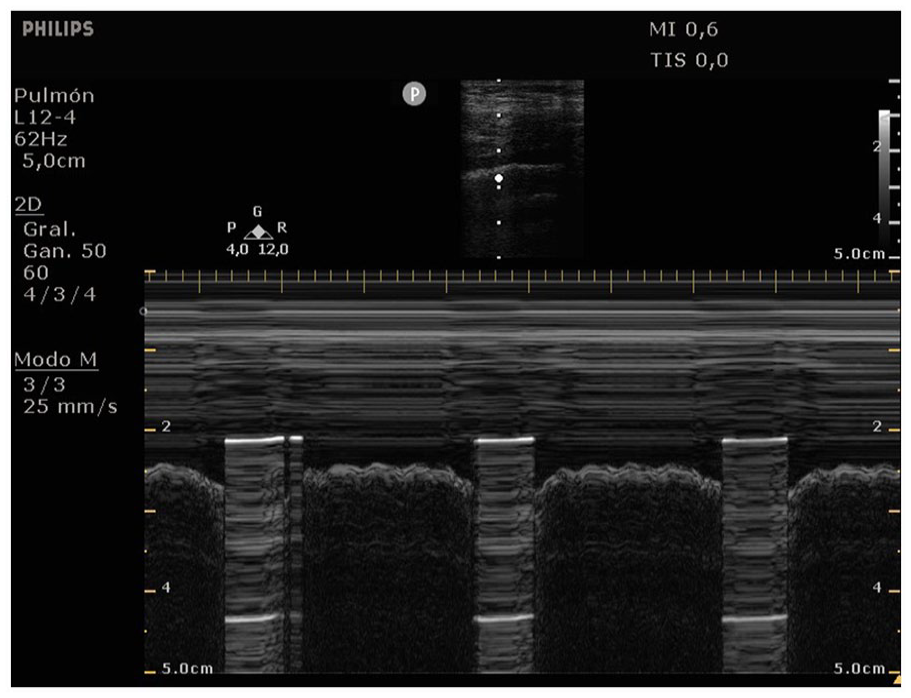
A M-mode tracing during a lung sonogram that was captured with a linear transducer, which revealed a characteristic pattern marked by an intermittent barcode sign and a sinusoid diagnostic sign.
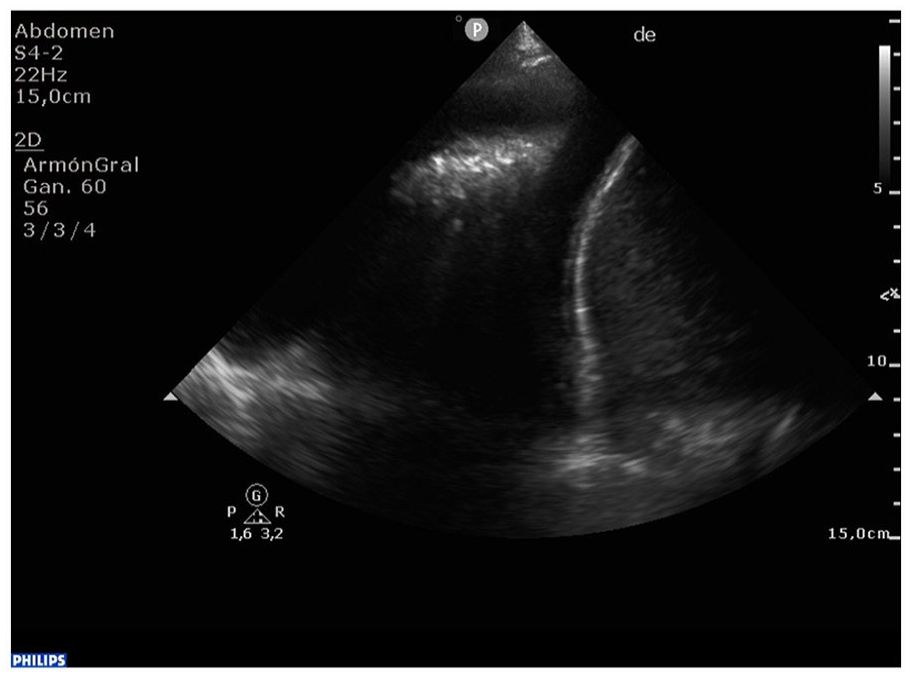
A grayscale lung sonogram acquired with a phased array transducer, which highlighted the presence of an anechoic pleural effusion located at the base of the right lung.
Emergency placement of a right pleural drainage tube was performed with the drainage of 600 mL of hematic content. As a result of poor clinical progress, the patient declined any further treatments or interventions but did receive end-of-life care. Unfortunately, the patient had a fatal outcome, a few days later.
Discussion
Lung sliding is a distinguishing diagnostic feature for normal lungs and is characterized by a visible to-and-fro movement of the pleural line, due to the inspiratory excursion of the lung. The M-mode application allows for the objective observation of lung sliding, which can be distinguished through the presence of a linear pattern above the pleural line and a gritty pattern below, called the seashore sign (see Figure 4).3,6
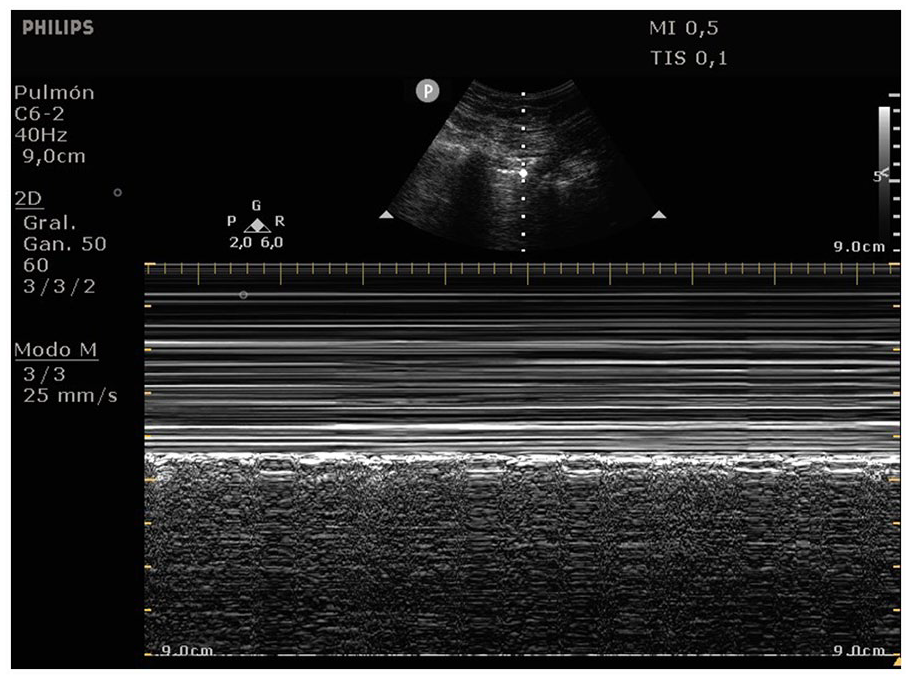
A M-mode tracing during a lung sonogram that was captured using a convex transducer, revealing a characteristic linear pattern above the pleural line and a gritty pattern below it. This diagnostic pattern is commonly known as the seashore sign.
If a pneumothorax occurs, the absence of lung sliding causes horizontal lines across the entire depth in the M-mode, which are known as the stratosphere or bar code sign (see Figure 5). Another distinctive indicator of pneumothorax is the lung point sign. This is a point where the transducer is stationary at the supposed junction between pneumothorax and lung, and sudden diagnostic lung signs appear, usually on inspiration. 7 The lung point sign is characterized by a synchronized change during the inspiration from a typical pattern with lung sliding to a pattern without lung sliding at a specific location. In M-mode, the lung point sign is seen as a sudden shift from the seashore sign to a bar code sign (see Figure 6).6,8
A M-mode tracing during a lung sonogram that was captured using a convex transducer, demonstrating a characteristic linear pattern across the entire depth. This diagnostic pattern is widely recognized as the stratosphere or bar code sign.
A M-mode tracing taken during a lung sonogram which was captured using a convex transducer, displaying a characteristic pattern with intermittent barcode sign and seashore sign. This diagnostic pattern is commonly referred to as the lung point sign.
With a hemopneumothorax, there are additional sonographic signs corresponding to pneumothorax, as well as the presence of a hypoechoic or anechoic image consistent with the presence of pleural effusion, commonly located in gravity-dependent areas. 3 During the M-mode tracing, the sinusoid sign can be identified, indicating the inspiratory excursion of the lung beyond the anechoic effusion, toward the pleural line (see Figure 7). 7
A M-mode tracing taken during a lung sonogram which was captured using a linear transducer and displayed the sinusoid sign, indicating the inspiratory excursion of the lung surface beyond the anechoic effusion toward the pleural line.
There is also a very characteristic sign called the hydropoint sign, which can be considered a variant of the lung point sign. It consists of a sudden alternation between an anechoic image corresponding to pleural effusion and the absence of lung sliding (see Figure 1). 9 When M-mode is applied at this point, it reveals a highly distinctive pattern called the defective barcode sign by Mahalingam et al. This pattern is characterized by an intermittent barcode sign that correspond to pneumothorax, as well as an intermittent sinusoid sign, which corresponds to pleural effusion (see Figure 2). This occurs due to a respirophasic motion and it demonstrates the coexistence of air and fluid in the pleural space. 10
Prompt diagnosis and management of hemopneumothorax is essential to prevent life-threatening complications. In this case, the patient underwent emergency surgery with emergency placement of a right pleural drainage tube.
Conclusion
In summary, lung sonography is a valuable diagnostic tool for the detection of hemopneumothorax, in critically ill patients. The use of lung sonography has the potential to provide a prompt diagnosis, expedite clinical management, and potentially improving patient outcomes.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Approval for this study was waived in accordance with the local regulations because this study is a case report of a single patient and did not include protected health information, data analysis, or testing of a hypothesis, and was de-identified.
Informed Consent
Written consent was obtained from the patient before the publication of this case report.