
Abstract
Objective:
To determine if lung sonography is accurate in assessing and confirming pulmonary compromise and thereby reduce the risk of x-ray exposure, for pediatric patients.
Materials and Methods:
This study was a systematic review of individual published studies. PubMed was the only database used for the article search. A review by a committee of contributors determined whether studies met the specific inclusion criteria. Studies reviewed had participants between the ages 0 and 18 years, with lung compromise of varying pathophysiological diagnoses. Each intervention was coded by levels of evidence; grading of recommendations, assessment, development, and evaluation (GRADE); the evidence alert traffic light grading system; and risk of bias in nonrandomized studies of interventions. Each article was evaluated using the Cochrane assessment of bias and GRADE evidence tables.
Results:
Thirty-seven articles were retrieved. Of those, 21 articles were removed following title and abstract screening. With 16 articles remaining, only one duplicate was removed. Based on the 15 articles extracted, in full-text versions, only two articles were noted to be irrelevant, and one article was not provided in English. Only 12 articles met the eligibility criteria, but two articles had to be removed because they were systematic reviews and not individual studies. The final analysis was based on 10 articles that met the inclusion criteria.
Conclusion:
Once reviewed, all 10 articles indicated that lung sonography had high accuracy and confirmation of lung compromise, which spanned multiple pulmonary diagnoses, in pediatric patients. When used by a trained clinician, lung sonography was as highly effective in comparison to other diagnostic tools, such as a chest radiograph and computed tomography.
Pediatric patients have unique medical needs, backed by anatomical and physiological differences from adults. Due to their developing bodies, rapid cellular division, and longer life expectancy than adults, it is important to minimize radiation exposure, when possible. Ionizing radiation can have an increased risk of carcinogenic effects, due to repeated exposures with radiographic imaging.1,2 Although radiographic imaging is the gold standard for diagnosis, reduction of exposure is paramount. Sonography is a proven method of imaging without the risk of radiation exposure to the patient. 3 Specifically, lung sonography has been increasingly used in adult populations. Current literature on adults, not examined in this review, with pneumonia have shown positive results in using lung sonography for analysis and diagnosis. 4 Pediatric lung health compromise is typically the result of a viral or bacterial infection. Commonly a pediatric patient will present with respiratory distress, cough, dyspnea, retractions, poor saturations, and fever. Progression to a lung consolidation is typically noted by auscultation, or percussion, leading to daily radiation exposure, with a chest radiograph for diagnostic confirmation. This systematic review examined the efficiency of lung sonography compared to a chest radiograph, in pediatric patients, for the detection of pneumonia, consolidation, pneumothorax, masses, and pleural effusions.
Materials and Methods
This study was a systematic review completed according to the preferred reporting items for systematic reviews (PRISMA) guidelines. The patient/population, intervention, comparison, and outcomes (PICO) question was, In pediatric patients with lung compromise (such as viral lung consolidation), does a bedside lung sonogram, following an initial chest radiographic confirmation, provide sufficient ongoing assessment/confirmation and reduce their overall radiation exposure risk, during their hospital admission?
Search Strategy
A search of the literature was conducted between November 17, 2020, and November 19, 2020, using the PubMed database, hosted by the university’s library. The search criteria were narrowed to include articles published between 2000 and 2020. Following a PICO questioning search strategy, articles were narrowed down to specifics, based on the titles that matched this review. A combination of chest or lung ultrasound, while including child or pediatric, was used as a narrowing search term factor. Finally, adding the terms radiation and reduction (or) decrease helped to eliminate articles out of the context of the review. The PRISMA search strategy was used to determine whether articles should be retained or removed. The primary author screened articles for inclusion, and two others screened the chosen titles for agreement.
Inclusion/Exclusion Criteria
The articles that were retained for this systematic review had to meet several inclusion and exclusion criteria. The following is a list of the inclusion criteria:
Participants had to be 0–18 years of age.
A comparison of lung sonography was made with other radiographic imaging techniques (chest radiography, computed tomography [CT], or transillumination in the neonate).
Patients had to have lung compromise (normal findings were removed).
Neonatal patients were included especially when radiographic or transillumination comparison was used.
In a similar manner, articles were removed if they met the preassigned exclusion criteria. The following is a list of the exclusion criteria:
The results were based on an adult population.
The article was a systematic review.
The article pulled was irrelevant to the topic of this systematic review.
The publication was deemed to have not been peer-reviewed.
If the article was a duplicate publication to others already retained.
The selection was not accessible in English language format.
The studies that were chosen for this systematic review were initially selected by the article title, abstract with results, and methods reviewed. The final study selection was determined after a thorough full-text review.
Data Extraction and Management
As a part of the process of procuring the data from the articles retained, some key components were uniformly extracted and recorded. The following is a list of the elements extracted from those articles that were retained:
Reviewer name
Answered the PICO question, or part of the PICO question
Study design
Patient population
Criteria of the individual study design
Interventions within the study
Comparison intervention
Outcome measurements
These critical elements led to the formative development of a data table that needed further appraisal. For an example of the worksheet used during data extraction, see Figure 1.
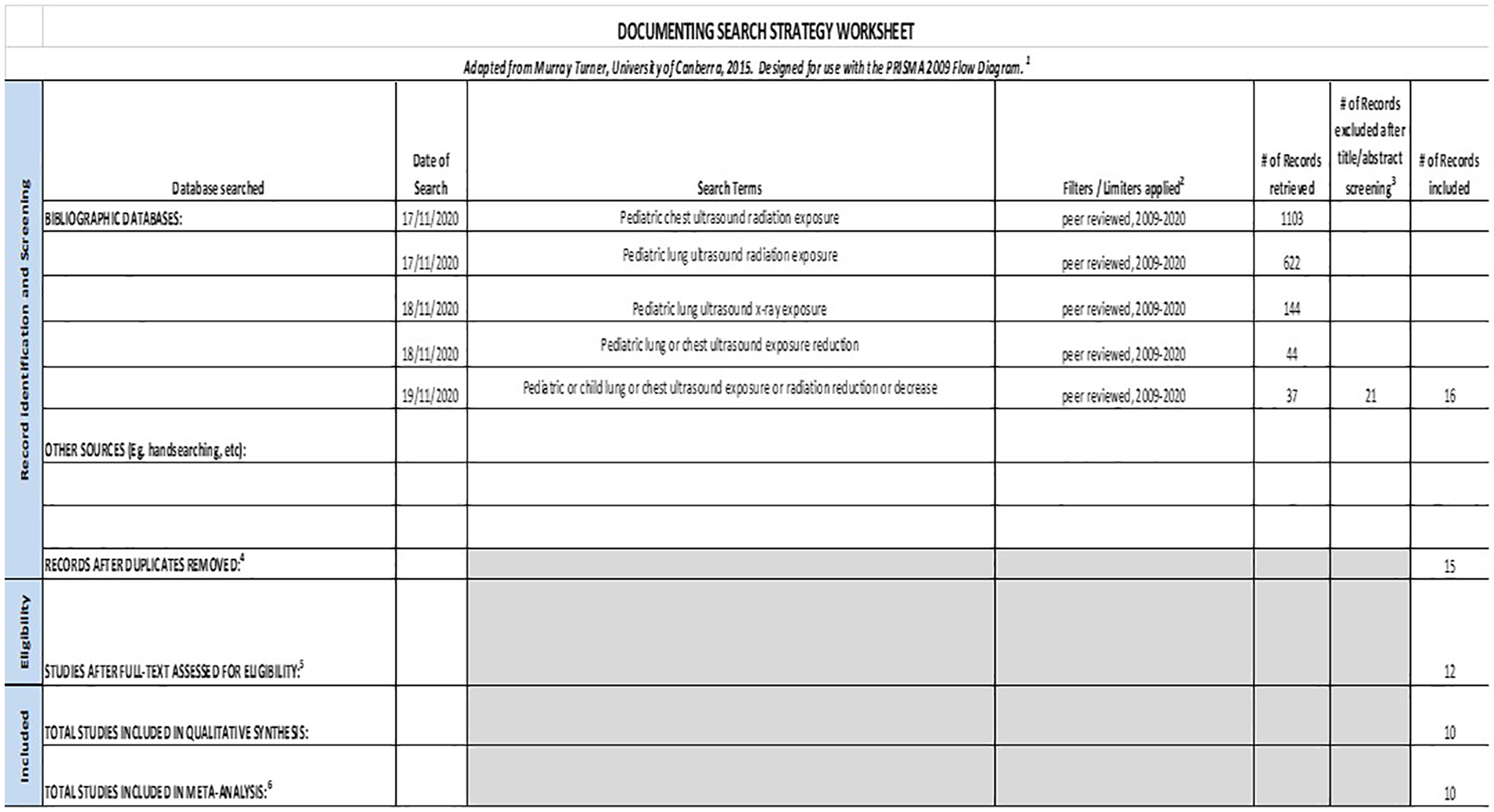
An example worksheet that was used to record the data extracted during this systematic review. PRISMA, preferred reporting items for systematic reviews.
Quality of Studies and Risk of Bias
The next step was to assess the methodological quality of the article retained. This was assessed using a step-by-step approach for each article, during the review process. During full-text review, each study was recorded into data-extraction sheets and assessed using the evidence alert traffic light grading system 5 and risk of bias in nonrandomized studies of interventions (ROBINS-I-version for cohort-type studies). 6 This phase of the assessment was conducted to determine the validity and bias of the information. In addition, it was important to gauge the strength of evidence and evaluate the recommendations, using the levels of evidence, grading of recommendations, assessment, development, and evaluation (GRADE). 7 Internal validity and bias were assessed specifically using the ROBINS-I assessment tool, which was applied to the article as well as the confounding elements, study participants, interventions, and outcomes. The main domains are preintervention, at intervention, and postintervention. The bias assessments of all studies were then compiled to form a Cochrane review table for comparison and analysis. The quality of evidence and strength of recommendation were evaluated using the GRADE process to score each body of evidence. Step one outlines the quality of the evidence, scoring the body of evidence, rated high to very low. Randomized controlled trials are rated high quality 4/4, compared to observational studies rated 2/4 initially. Points are reduced by risks of sample bias, inconsistency of study, indirectness of study, imprecision of study meaning lack of confidence, and publication bias. Each study was then tabled for quick reference, in the GRADE table. The process was finalized with the evidence alert traffic light system.
Results
After the database search criteria narrowed results to the desired inclusion criteria, 37 articles were retrieved. Twenty-one articles were removed based on the title and abstract screening. Of the 16 articles that remained, only one duplicate was removed. Next, 15 articles were extracted in full-text versions to make it convenient for reviewing. On closer inspection, two articles were found to be irrelevant to this review, and one article was not available in the English language. Finally with only 12 articles meeting the eligibility criteria, two articles had to be removed because they were systematic reviews and not individual studies. The remaining 10 studies were included within this systematic review. The PRISMA outline of the study results is provided in Figure 2.
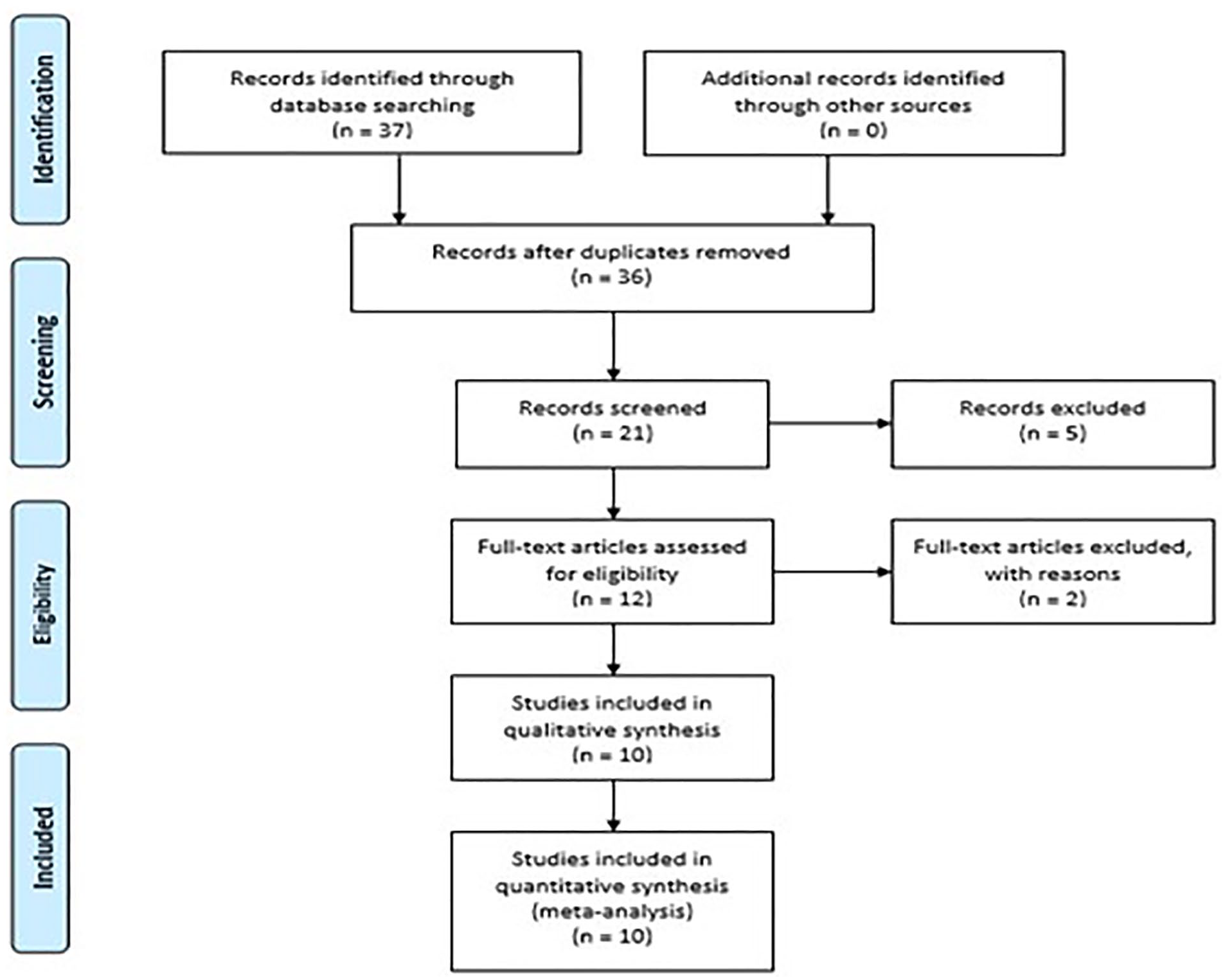
The PRISMA outline of the systematic review of articles selected from PubMed based on the use of lung sonography. PRISMA, preferred reporting items for systematic reviews.
This systematic review considered multiple pulmonary complications such as pneumonia, pneumonia specific with bronchiolitis, chest radiographic opacities, pulmonary tuberculosis, neonatal pneumonia, and pneumothorax. The effectiveness of lung sonography in comparison with other imaging techniques was the intended purpose. All the studies procured indicated a positive result, demonstrating the versatility of sonography as a possible intervention instead of radiography.
All the articles retained were graded based on their levels of evidence. Eight of the articles rated moderate with either weak positive or strong positive strength of recommendation. Only one out of the 10 studies were given a high level of evidence, with a strong positive strength of recommendation. However, this article was based solely on neonates. One article was rated low for levels of evidence, with a positive strength of recommendation. The measured outcomes and results of each article are compiled together with extracted data (see Figure 3a-e: Evidence Summary).
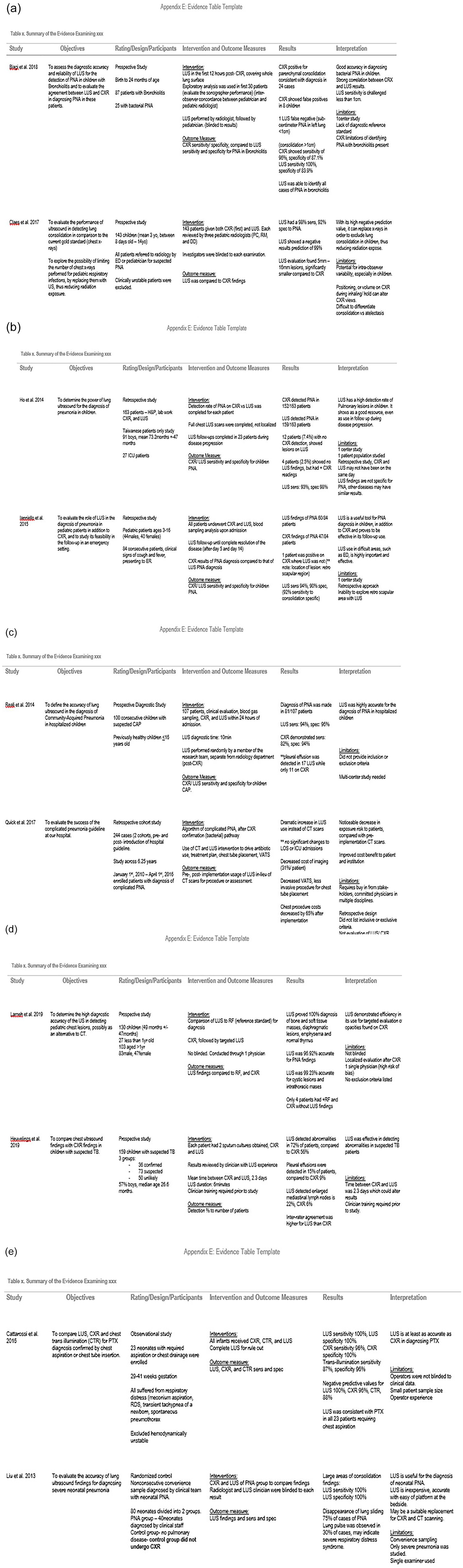
The summary of evidence procured from the systematic assessment of the published articles retained. (a-e) Summary of the evidence examining Lung Ultrasound use in pediatric patients. CAP, community acquired pneumonia; CT, computed tomography; CXR, chest x-ray; ED, emergency department; ER, emergency room; LOS - Length of stay; LUS, lung ultrasound; PNA, pneumonia; RF, reference standard; TB, tuberculosis; VATS, video-assisted thoracoscopic surgery.
Each article was assessed for publication bias using the ROBINS-I format. Individual bias assessments were completed for all 10 articles. The most commonly identified biases were anonymizing of participants, anonymizing of outcome assessments, and allocation concealment. This is partially due to the type of studies available for review. The studies are mainly prospective and retrospective studies. Some studies were able to have some anonymizing, in regard to the sonographer or radiologist knowing other outcomes. However, the majority of them did not have anonymizing or allocation because of the sample size or type of study performed. Individual studies’ risk of bias was reported (see Figure 4. Cochrane bias assessment).
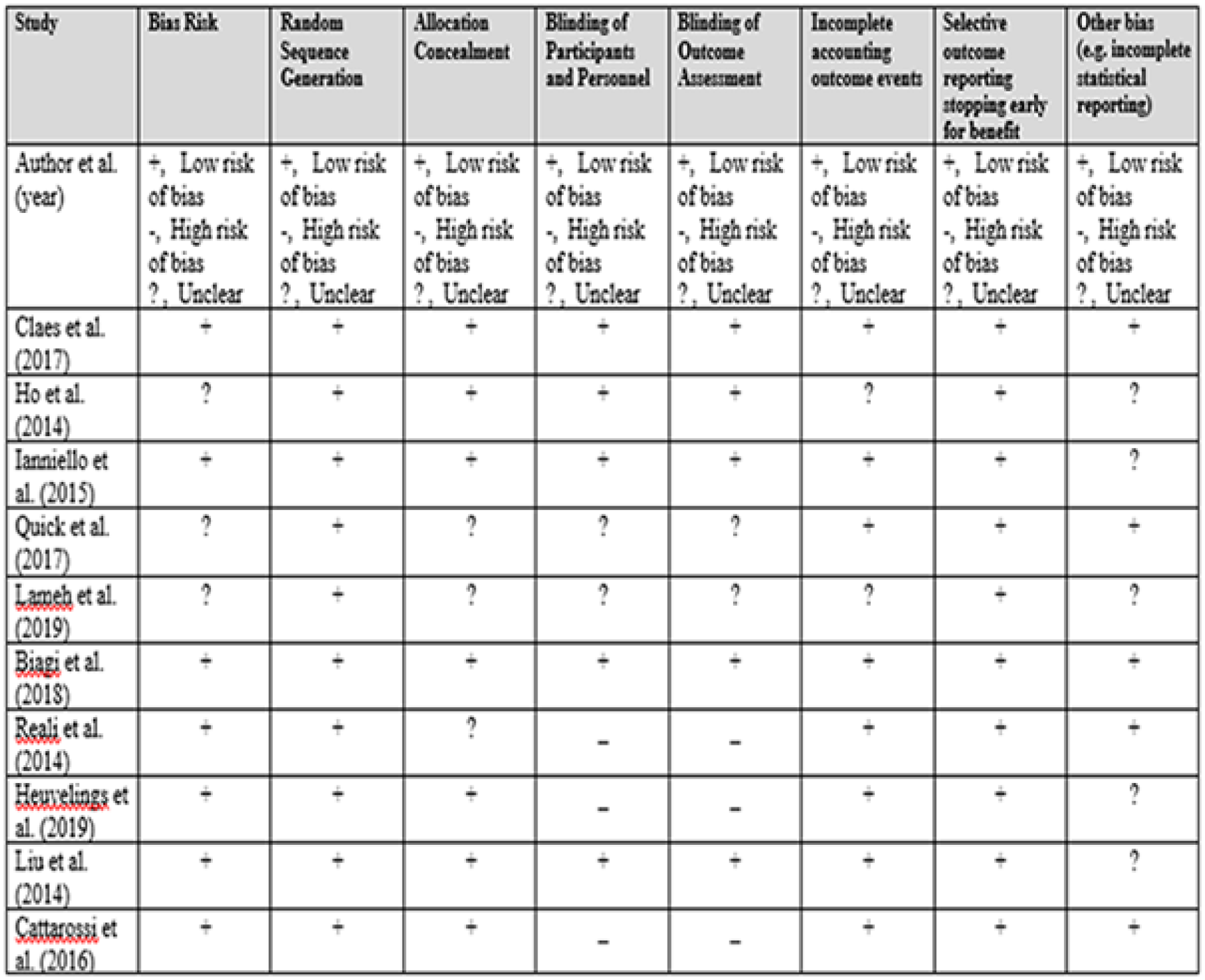
Article review based on the Cochrane bias assessment.
The articles were scored systematically using the GRADE quality of evidence with the evidence alert traffic light system. The most common quality rating seen among the articles, in regard to scoring the body of evidence, was related to the type of studies conducted. Point reduction was seen because studies were prospective or retrospective. All studies maintained some risk of bias. Yet, none had a risk based on publication, inconsistency, indirectness, imprecision, and so forth. Each study was given a “green light,” go ahead, for traffic light recommendations. This was based on a risk versus risk of imaging in pediatric patients described by the researchers. Lung sonography does not expose the patient to ionizing radiation, compared to alternative radiographic imaging.1–3,8,9 Overall, each author noted that sonography was a safer alternative, and each study set out to examine its effectiveness and performance in diagnosing. All quality of evidence and strength of recommendations were recorded in Figure 5 (GRADE quality).
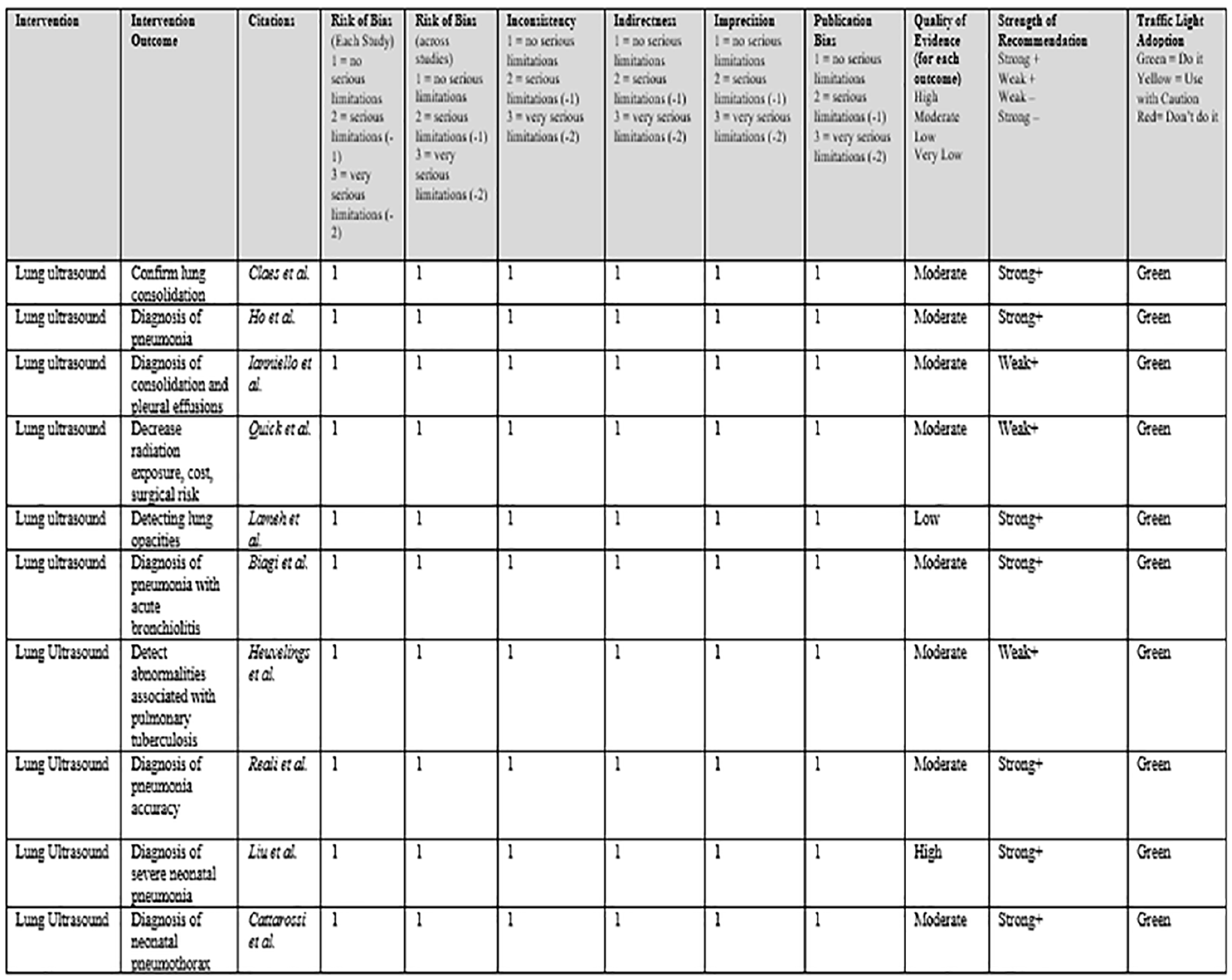
Examples of the quality of evidence and strength of recommendations.
Discussion
The research question for this systematic review was, In pediatric patients with lung compromise (such as viral lung consolidation), does a bedside chest sonogram, following an initial chest radiographic confirmation, provide sufficient ongoing assessment/confirmation and reduce their overall radiation exposure risk, during their hospital admission? The results of this review were based on neonates, infants, or pediatric patients (0–18 years) with lung compromise, by consolidation, atelectasis, pneumothorax, or infection leading to pneumonia or effusion. Although the evidence was limited, these published works support the use of lung sonography, for the assessment and diagnosis of lung tissue. Lung sonography has been tested broadly in these pulmonary conditions. Although further, multicenter studies will certainly add to the knowledge base, the articles procured received a GRADE recommendation rating of strong+ and an evidence alert traffic rating of green. Lung sonography appears to be surfacing as a strong diagnostic tool for pediatric patients with lung compromise. 10
The main success of lung sonography, in neonates or pediatric patients, is the recent effort to reduce ionizing radiation and pediatric dose. Lung sonography may be able to offer relatively the same, or better, assessment and diagnosing ability, without any risk to the patient. While sonographic imaging may take from 6 to 10 minutes, it can be done at bedside, eliminating the need of transporting to a radiology department, which may avert other viral transmission issues as well. This discussion is organized into the key elements, pulled from the review, that highlighted what sonography provides for each lung condition.
Lung Sonography Used to Detect Pneumonia
Five of the articles reviewed the use of sonography in pediatric patients, with pneumonia. Bacterial or viral lung consolidations are difficult to differentiate from atelectasis in imaging. Patients’ symptoms and physical assessment guide a provider to order chest imaging for diagnostic confirmation. Chest radiographs and a chest CT are considered the gold standard in detecting pneumonia. This is of course coupled with the increasing importance of reducing the ionizing radiation exposure to pediatric patients. Sonography is a nonionizing diagnostic source of radiation exposure but does ensure quality diagnostic imaging. When considering pneumonia, lung sonography has been shown to have a high negative prediction value and diagnosis efficiency. 11 The negative prediction value refers to the ability of a lung sonogram to rule out a diagnosis, especially when compared with other diagnostic tools. Negative predictive value is a probability that patients with negative screening, using lung sonography, truly do not have pneumonia. Pneumonia that has not fully consolidated within the lung tissue may not be present during early assessment with tools such as chest radiographs. Patients with a negative chest radiograph may still be positive for pneumonia. 8 In one study, lung sonography found 17 areas of consolidation in 8 patients with pneumonia. 8 Three studies demonstrated that lung sonography has high sensitivity and specificity. Across the studies reviewed, lung sonography had either a sensitivity of 98% and a specificity of 92% 8 or a sensitivity of 98% and a specificity of 93.4%, 1 as well as a reported sensitivity of 94%. 12 Based on these statistics, it would appear that lung sonography is a reliable tool for diagnosing pneumonia in pediatric patients.
Lung Sonography Used to Detect Pneumonia With Bronchiolitis
One article specified the use of lung sonography to document pneumonia in pediatric patients, with bronchiolitis. Pneumonia, specifically in infants or toddlers with bronchiolitis, typically develops as a bacterial pneumonia, secondary to viral illness. Based on the review, lung sonography showed good accuracy in diagnosing bacterial pneumonia in infants. It is important to note that the diagnosis is more clearly made when lobar consolidation exists along the pleural wall or lining. Consolidation of less than 1 cm may be missed during a lung sonogram. 10 It is also unlikely that a consolidation of less than 1 cm would be diagnosed with a chest radiograph. 10 Using lung sonography had a high specificity, 98.4%, compared to a chest radiography and an 87.1% specificity, for consolidations of less than 1 cm, in pediatric patients with bronchiolitis (see Figures 6 and 7).
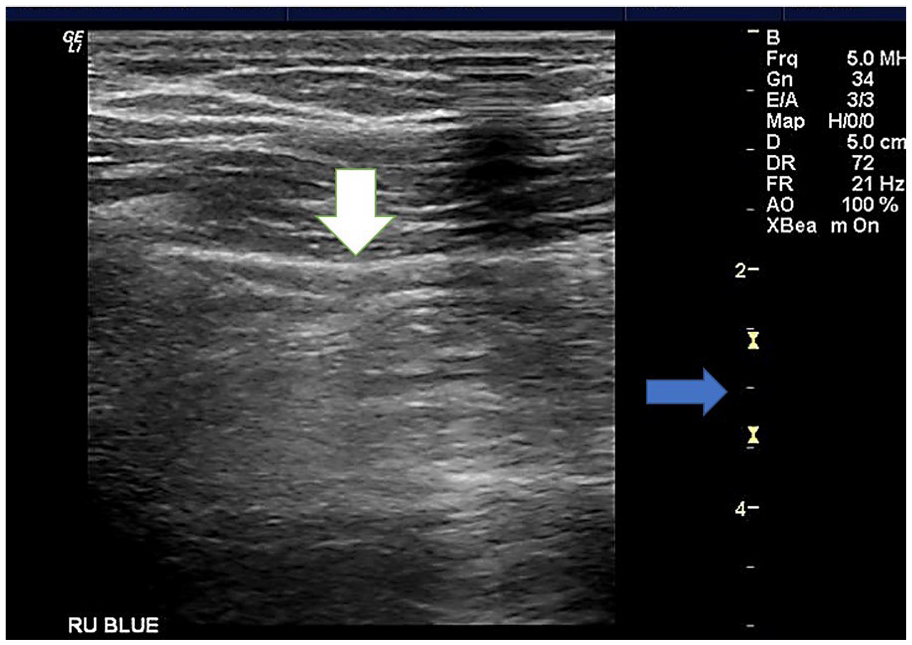
A BLUE-point right upper anterior sonographic image of a pediatric participant who complained of shortness of breath. The pleural line is seen (white arrow), but the penetration of the lung tissue is limited to less than 1 cm (blue arrow at 2-3 cm).
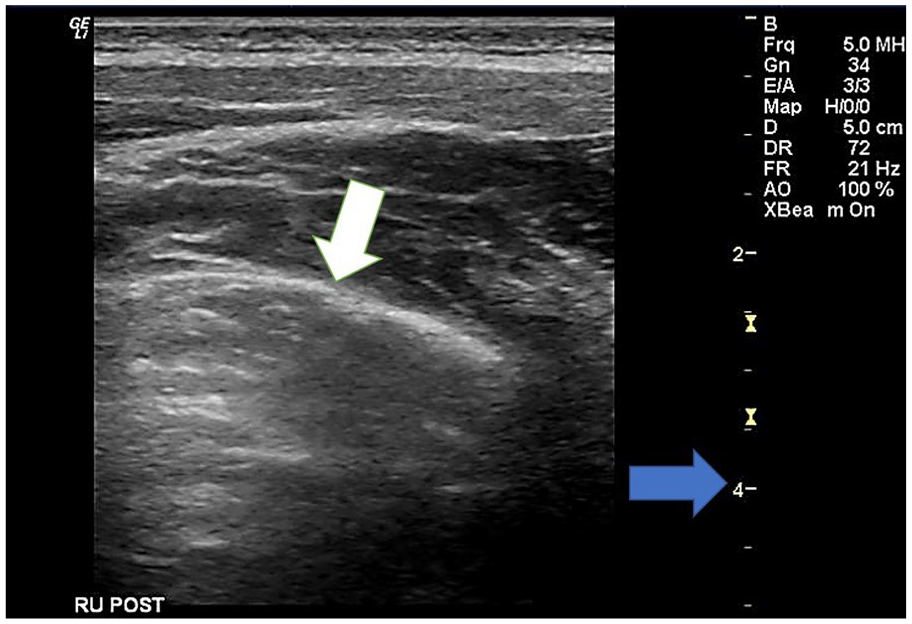
A BLUE-point right upper posterior sonographic image of a pediatric participant who complained of shortness of breath. The pleural line is seen (white arrow), but again the penetration in this area of the lung is limited due to absorption of the beam (blue arrow at the 3-4 cm).
This published evidence would indicate that lung sonography is a strong alternative to a chest radiograph for this specific pathology. 10
Lung Sonography Used to Identify Chest Radiographic Opacities
One of the articles, in the review, described using lung sonography to follow radiographic chest opacities, not specific to pneumonia. These radiographic opacities would be entities such as diaphragmatic lesions, cystic lesions, bone and soft tissue masses, intrathoracic masses, localized empyema’s, thymus, and pneumonia. These opacities are causes of pediatric cough, chest pain, and shortness of breath, which resulted in the need for diagnostic imaging. The opacity identified on a chest radiograph is a result of diagnostic testing that follows from the initial patient complaint. Many of these cases require a follow-up chest CT or magnetic resonance imaging. 13 Lung sonographic accuracy was compared to the opacity identification on a chest radiograph. Lameh et al 13 found that lung sonography was 100% accurate in the diagnosis of bone and soft-tissue mass, diaphragmatic lesions, empyema, and normal thymus, and the accuracy was 96.92% for pneumonia and 99.23% for cystic lesions and intrathoracic masses. The high accuracy is due to the localized process and the ability to position the ultrasound transducer following an initial chest radiograph. However, a systematic approach to lung sonography and the overall chest assessment should be used to also identify these opacities. Based on this limited evidence, lung sonography appears to be an appropriate diagnostic tool for the diagnosis of pediatric radiographic opacities and lesions. 13
Lung Sonography Used to Detect Pulmonary Tuberculosis
One article was included that compared chest radiography to lung sonography in pediatric patients with pulmonary tuberculosis. Pulmonary tuberculosis often demonstrates pulmonary consolidation and effusions in symptomatic patients. Patients may also have enlarged mediastinal lymph nodes. When compared to the chest radiographic identification of these findings, lung sonography more frequently identified the abnormality. 14 Heuvelings et al 14 found that lung sonography detected abnormalities in 72% of the patients studied, compared to 56% with chest radiography. Lung sonography detected enlarged mediastinal lymph nodes more frequently (22%) than chest radiography (6%). 14 Large masses, consolidations, or effusions are much easier to identify when conducting chest imaging. Heuvelings et al 14 noted that lung sonography may have limitations given that diagnostic findings, at the pleural line, are more likely to be detected, but those abnormalities that are beyond the pleural line may be missed when using sonography. This is a very important point made by the authors when considering this particular clinical application. Training the clinician to use a systematic scanning approach when using lung sonography may be a way to raise effectiveness. This becomes even more paramount when large consolidations, masses, or effusions may not be present.
Lung Sonography Used to Detect Neonatal Pneumonia
One article outlined the use of lung sonography in neonatal pneumonia, specifically. Neonatal lung sonography demonstrated a high sensitivity (100%) and specificity (100%) for large areas of consolidation in severe neonatal pneumonia cases. 9 Due to the size of the patient, compared to the size of the ultrasound transducer and equipment system, as well as the depth of acoustic pressure, lung pulse may be observed in severe respiratory distress. 15 Lung pulse in unventilated patients is associated with severity of atelectasis. 9 This demonstrates the effectiveness and safety of lung sonography use with neonatal patient populations.
Lung Sonography Used to Detect Neonatal Pneumothorax
One article reported on the use of lung sonography in detecting neonatal pneumothorax compared with chest radiography and chest transillumination. Historically, a pneumothorax in a neonatal patient is examined by chest radiography or transillumination. Transillumination has been used as a quick assessment of the chest without imaging or exposing the neonate to radiation. Lung sonography showed a 100% sensitivity and specificity for the diagnosis of a neonatal pneumothorax. 16 This was in comparison to the chest radiography’s sensitivity of 96% and specificity of 100% and assessed against transillumination’s sensitivity of 87% and specificity of 96%. 16 In this case, lung sonography demonstrated that it was more sensitive than the historically used diagnostic tools for neonatal pneumothorax. Cattarossi et al 16 stated that lung sonography is at least as accurate as using chest radiography in obtaining the diagnosis of neonatal pneumothorax. Cattarossi et al 16 also noted that the lung point seen with sonography may be used to differentiate between a large and a small neonatal pneumothorax.
Limitations
This systematic review has some limitations. First, it is clear from the initial database search that few articles existed around pediatric and lung sonography. This systematic review analyzed articles from a singular database and may not be an exhaustive review of all literature available. Additionally, lung sonography is still not a universally used diagnostic technique and is just recently being evaluated for adult coronavirus disease 2019 (COVID-19) patients. Adult patient populations are more commonly studied before pediatrics, and it is apparent within the search results. Second, there is an overall scarcity of studies on each of the lung conditions. This systematic review had to analyze multiple lung conditions due to the lack of studies surrounding one pulmonary compromising condition. Third, many studies suggest the need for multicenter studies with larger populations to confirm their results. The literature just is not robust enough, with no large patient sample sizes to provide a definitive answer one way or the other. However, the results are promising. Lastly, each article concluded with a need for further studies and use of multicenter patient recruitment and studies. This review also demonstrates the need for more studies with the multicenter approach for guideline creation in using chest ultrasound with specific lung conditions. Future published studies, even current COVID-19 pandemic studies, should include pediatric data where possible.
Conclusion
This systematic review of lung sonography used with pediatric patients for the assessment and confirmation of lung complications yielded high effectiveness in pneumonia, pneumothorax, opacities, masses, and tuberculosis diagnoses. Lung sonography applied to pediatric patients demonstrated similar or better results than traditional ionizing radiation diagnostic tools in each lung condition where the consolidation or lesion was bigger than 1 cm. Although this was a limited review, hospital clinicians should be encouraged to include lung sonography as a tool for evaluating patients with lung compromise. A full systematic approach adopted by the clinician using lung sonography should only take 6–10 minutes to complete. Using lung sonography at the bedside provides an added diagnostic benefit and could reduce the risks and complications associated with transporting patients to radiology. Ultrasound equipment systems offer a lower cost to the institution, also providing more imaging opportunities due to its availability and ease of use at the patient’s bedside. Lung sonography has been shown to possibly be effective even for small lung lesions. Lung lesions that are less than 1 cm may be successfully detected with sonography. Lung sonography has been shown as a safe and effective tool for diagnostic imaging, while also providing a quality assessment and reducing radiation exposure risk. Future research that highlights the use of sonography to detect pediatric lung diseases or compromise, across a multi-institutional framework, is still needed.
Footnotes
Image Consent
Images were provided from an institutional review board–approved study of pediatric sonography for lung disease. OSU#2021H0448.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.