
Abstract
Objective:
The primary goal of this article is to show that an abbreviated ultrasonography (US) examination protocols can decrease imaging time and staff exposure.
Materials and Methods:
This is a single-center institutional review board (IRB)-approved retrospective cohort study in which 39 patients, positive for 2019 coronavirus disease (COVID-19), underwent an abbreviated US examination protocol from April to May 2020. Radiologists, specializing in body imaging, created these protocols. Descriptive statistics were performed, including the mean duration of the abbreviated US protocols and the mean duration of the standard US protocols, as a control group.
Results:
The abbreviated US protocols resulted in a significant time reduction (P < .05) compared with the regular protocol duration.
Conclusion:
As radiology services face this unprecedented pandemic, implementing reduced US protocols can result in safer practices decreasing staff exposure.
The 2019 coronavirus disease (COVID-19) has been labeled a pandemic by the World Health Organization (WHO) and has contributed to thousands of deaths and hospitalizations, worldwide. The pandemic began in December 2019 in Wuhan, China. At the time of writing, approximately 197 682 958 cases have been confirmed, according to the coronavirus resource center, at the Johns Hopkins University School of Medicine.1,2 Many COVID-19 cases have been identified as having mild symptoms. However, more extreme cases have led to respiratory failure, septic shock, and multiple organ dysfunction, causing enormous human fatalities and severe economic loss. Therefore, the development of strategies to contain the viral spread continues to be urgently needed.3,4
Because of high transmissibility, there is considerable risk to health care workers who may become infected and unintentionally become a source of continued transmission.5,6 Standardized personal protection protocols can reduce the risk of cross-infection. Containing disease spread involves protecting health care workers. 7
Imaging equipment, especially for conducting ultrasonography (US), is at high risk for surface transmission because of frequent direct contact with patients. US is frequently required to diagnose comorbid conditions, such as pleural effusion, renal obstruction, cholecystitis, and deep venous thrombosis (DVT).8,9 Easy availability, accurate and rapid results apart from performing a longitudinal assessment, at frequent intervals without ionizing radiation, makes US a valuable diagnostic tool for patient management. 10
COVID-19 has essentially changed the way health care workers provide care for patients. The use of portable US can limit the staff exposure to a confirmed or suspected case, compared with performing imaging, in the department. Most recently, point-of-care ultrasound (POCUS) provides numerous benefits, including minimizing interaction with patients, decreasing resource utilization, and guiding management of the critically ill patient, with COVID-19.11-14
Safety Guidelines When Performing Abbreviated US Examination Protocols
The decision to image patients, who are positive for COVID-19, is based on how the imaging will impact patient care. An important and necessary consideration for radiology departments is to ensure the safety of technologists and physicians by providing personal protective equipment (PPE) and promoting the use of institutional guidelines and recommendations.15,16
Although not the primary goal, it is essential to outline other precautions when planning an US, in the context of COVID-19. Several national and international recommendations for infection prevention in US have been published, as well as procedures to perform a safe routine or targeted sonogram. 17
Designating one ultrasound equipment system for scanning patients with a positive COVID diagnosis is one approach. When the US procedure involves contact with a patient’s intact skin, no probe cover is used. However, when conducting an evaluation of a contaminated patient’s open wound, a single-use cover is utilized. Most recently, according to Centers for Disease Control and Prevention (CDC) guidelines, low-level disinfection is effective for external procedures. Therefore, ammonium chloride-containing wipes are used to disinfect the ancillary equipment after every examination.17,18
It is crucial to examine the radiology departments’ current infection control and prevention practices to reduce cross-contamination and protect health care professionals. 19 These factors are considered when creating abbreviated US examination protocols to diminish exposure by reducing images and improving workflow with COVID-19 patients, while maintaining minimum diagnostic standards.
Materials and Methods
This was an institutional review board (IRB)-approved retrospective cohort study with 39 patients who underwent an abbreviated US examination protocol, from April to May 2020. The abbreviated US examination protocols and safety guidelines were developed specifically for the COVID-19 pandemic and also drew from the expertise of other institutions. This also included a multidisciplinary consensus with colleagues specializing in infectious diseases, emergency medicine, pulmonary and critical care.
Abbreviated US Examination Protocol
Registered diagnostic medical technologists performed the examinations, and board-certified radiologists interpreted the studies. The abbreviated US examination protocols included a lower extremity DVT sonogram (see Appendix A), an upper extremity DVT sonogram (see Appendix B), a lower extremity arterial Doppler examination (see Appendix C), an upper extremity arterial Doppler examination (see Appendix D), a liver sonogram (see Appendix E), a liver Doppler examination (see Appendix F), and a renal sonogram (see Appendix G). The abbreviated US examination protocols utilized were retrospectively reviewed through the picture archiving and communication system (PACS). All appendices are available online as Supplemental Material.
Data Retrieval
Data from patients were retrospectively retrieved from the institutional search engine using the keywords “COVID-19 protocol” and subsequently selected for the appropriate use of the abbreviated US examination protocols. Therefore, exclusion criteria included an incomplete examination protocol as well as patients with a negative COVID-19 test. Repeated search results, for the same patient, were also considered an exclusion criterion.
The collected variables included the time duration of the abbreviated US examination protocol and demographics, such as age and gender.
Statistical Analysis
Descriptive statistics were performed, including the mean duration of the abbreviated US examination protocols and the mean duration of the standard US examination protocols were used as a control group. Subsequently, a correlation of both values using t student analysis was performed. The statistical significance was set as P = .05, a priori.
Results
Demographic data of patients include age ranging from 14 to 85 years with a mean of 55 years, and gender, for which 22 were males and 17 females. All the abbreviated US examination protocols resulted in reduced time compared with standard evaluation (see Figure 1).
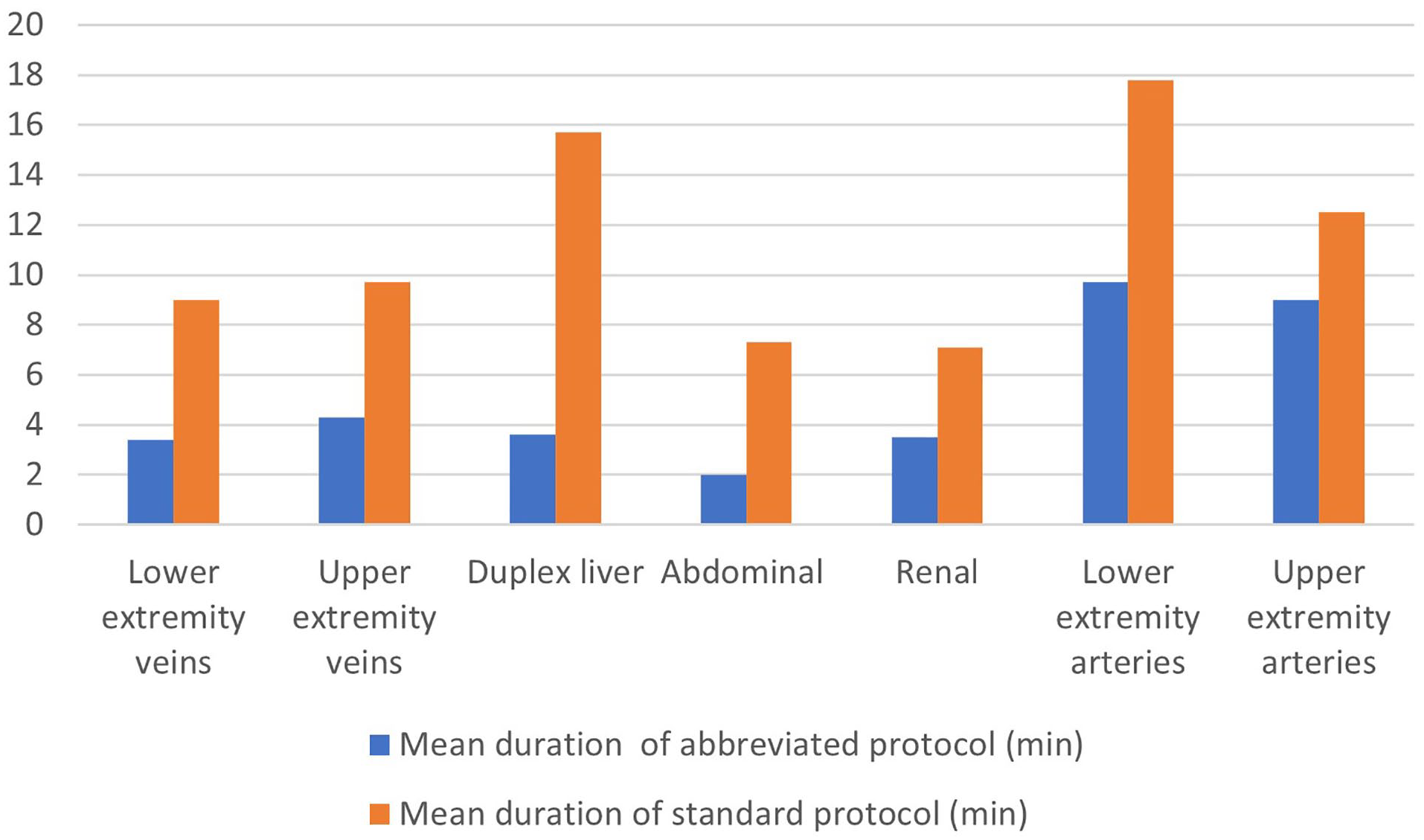
The graphic compares the mean duration of abbreviated ultrasonography examination protocols versus the standard examination protocols, demonstrating that the abbreviated examination protocols resulted in a significant time reduction.
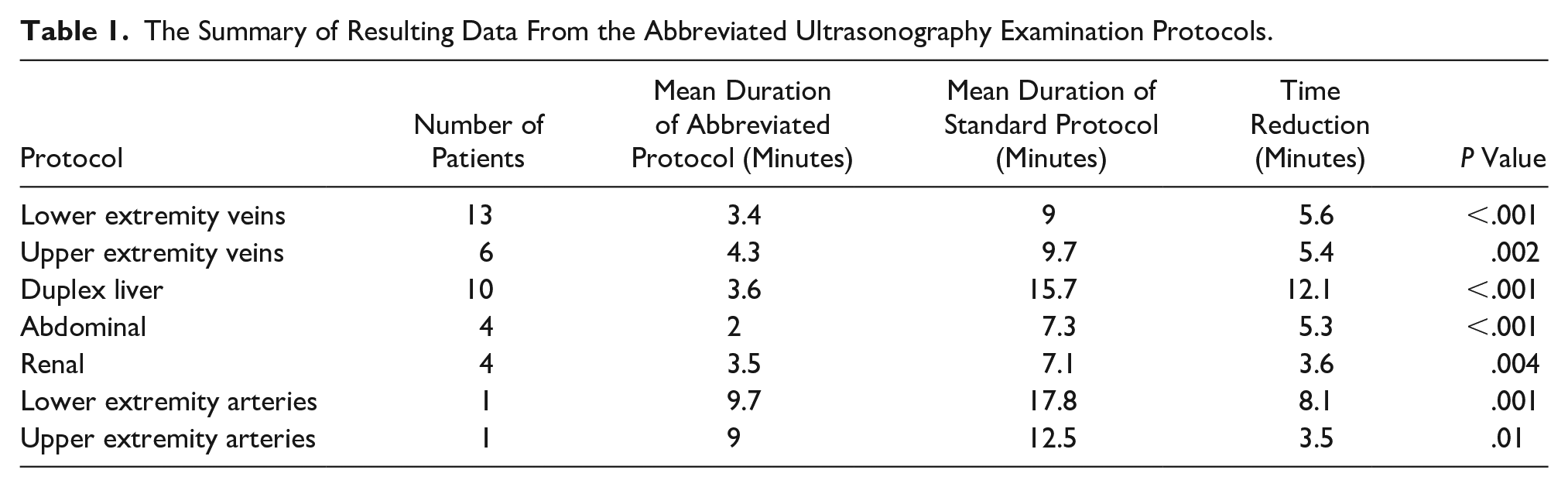
The following breakdown of abbreviated US examination protocols is listed in Table 1. A total of 13 patients had a lower extremity venous sonogram with a mean duration of 3.4 minutes in the abbreviated protocol, with 5.6-minute reduction compared with the regular protocol (P < .001). The abbreviated upper extremity venous sonogram had a mean duration of 4.3 minutes, which represented a reduction of 5.4 minutes (P = .002). Regarding the liver duplex ultrasound, the mean duration of 3.6 minutes for the abbreviated protocol signified a total decrease of 12.1 minutes (P < .001). Four patients were evaluated with the abbreviated abdominal sonogram protocol, which had a mean duration of 2 minutes. This represented a decrease of 5.3 minutes (P < .001). The abbreviated renal sonogram protocol resulted in a reduction of 3.6 minutes (P = .004). Regarding the lower extremity and upper extremity arterial Doppler, a time reduction of 8.1 minutes (P = .001) and 3.5 minutes (P = .01) was obtained.
The Summary of Resulting Data From the Abbreviated Ultrasonography Examination Protocols.
Discussion
US is used more frequently for medical diagnosis and treatment; however, according to Westerway et al, it may be overlooked as a potential vector in transmitting a health care-associated infection. 20 Specifically, there have been calls for the protection of health care workers, and various tools for risk stratification have been developed worldwide. 21
Although certain health care workers may be considered high risk due to exposure to oronasal secretions, the risk to other workers must not be underestimated. Bandyopadhyay et al did a systematic review highlighting the need for universal guidelines for testing and reporting infections in health care workers. 22 Gholami et al described the clinical outcomes and risk factors for COVID-19 infection, in health care workers. They showed a significant number of infected health care workers during the first 6 months of the pandemic, with a prevalence of hospitalization of 15.1% and mortality of 1.5%, hence the importance of this study and considering this factor among radiology departments and specifically during US. 23
This study showed that an abbreviated US examination protocol resulted in a significant time reduction compared with the regular US examination protocol, which could diminish the exposure of health care workers. The time reduction is achieved by reducing the number of images while maintaining diagnostic imaging standards. Gepner et al investigated the ability to identify increased carotid intima–media thickness with abbreviated examination protocols compared with comprehensive US examination protocols. They showed that abbreviated examination protocols were 100% sensitive, therefore, validating the diagnostic value of this particular abbreviated US examination protocol. 24
The American Society of Echocardiography (ASE) provided a “Statement on Protection of Patients and Echocardiography Service Providers during the 2019 Novel Coronavirus Outbreak.” They also focused on determining the examination’s urgency, selecting equipment and rooms, cleaning, disinfecting, and addressing scanning techniques. 25 Similar to this study, their strategy for limiting exposure is shortening the examination time. An abbreviated US examination protocol might yield the desired information while decreasing the time needed for the technologist to be exposed to the patient. They also highlight additional ways to limit exposure, keep the equipment clean and disinfected, and appropriate use of PPE according to the patient status.
In addition, the World Federation for Ultrasound in Medicine and Biology (WFUMB) Safety Committee provided official guidance to ensure a consistent approach to safe US practices, during the COVID-19 pandemic. 15 Wessner et al focused on preventing the transmission of COVID-19 from ultrasound equipment systems and created an US examination protocol for these patients. 26 Their experience concurs with this study, highlighting that shorter protocols and target images can answer the clinical question. Similarly, they also replaced the number of static images with video clips, to reduce staff’s exposure time.
Limitations
This study has strengths and weaknesses. It was a relatively small study and during a short time at the beginning of the COVID-19 outbreak. It demonstrates specific abbreviated US examination protocols and evaluates the decreased examination time to minimize patient contact and ensure staff protection. In addition, given the study’s retrospective nature, this is subject to convenience sampling and selection bias. Therefore, it is not possible to generalize the results to the entire population. Despite the limitations, this work allows radiologists to undertake leadership roles in executing new imaging protocols and monitoring quality and safety compliance, especially in the current pandemic times. Ideally, these abbreviated US examination protocols should be performed on a large scale and followed longitudinally, to evaluate the impact on health care safety guidelines.
Conclusion
The current pandemic situation is evolving, and health care dynamics change as more information is obtained. As radiology services face this unprecedented time, implementing new examination protocols can potentially ensure safer practices maintaining good patient outcomes. Ideally, the changes US examination protocols should be done as an adjunct to safety guidelines. Ultimately, the implementation of an abbreviated US examination protocol could offer the possibility of providing quality care to patients while taking into consideration staff protection.
Supplemental Material
sj-docx-1-jdm-10.1177_87564793221079805 – Supplemental material for Abbreviated Ultrasonography Examination Protocols for COVID-19 Patients: A Streamlined Process to Reduce Staff Exposure
Supplemental material, sj-docx-1-jdm-10.1177_87564793221079805 for Abbreviated Ultrasonography Examination Protocols for COVID-19 Patients: A Streamlined Process to Reduce Staff Exposure by Cibele Luna, Indira Estanga and Rosa Patricia Castillo in Journal of Diagnostic Medical Sonography
Footnotes
Acknowledgements
Thank you to Rubyvette Jencic and Surizaday Collazo, Jackson Memorial Hospital Ultrasound Technologists, for their valuable contribution and feedback on the implementation of the protocols.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.