
Abstract
Objective:
Lung involvement due to COVID-19 infection relates to patient clinical outcomes. However, little evidence exists on whether an abnormal lung sonogram, during an initial outpatient infection, may signal an abnormal immunologic response and lasting abnormalities. The aim of this study was to observe whether high-risk outpatients, previously infected with SARS CoV-2 and found to have an initial abnormal lung sonogram, had persistent diagnostic findings at a 1-year re-examination.
Materials and Methods:
A prospective longitudinal cohort study was performed, based on a prior study completed in January 2022 wherein 55/201 (27%) of consecutive outpatients infected with SARS-CoV-2 received therapy at an outpatient monoclonal antibody clinic and had presented with an abnormal lung ultrasound containing at least 3 apical lung B-line artifacts (LUS+). One year later, the original 55 LUS+ patients were contacted for re-examination; as a result, 14 LUS+ patients consented to a repeat LUS tospecifically recheck the apical area of the lungs for persistent B-line artifacts. The same ultrasound equipment system and imaging methodology were used for this cohort of patients. Additional data was collected regarding COVID-19 test-positive re-infection, persistent pulmonary symptoms during the past year, and COVID-19 vaccination status.
Results:
Of the 14 LUS+ patients, the mean cohort age was 63 ± 9 years, of which 71% were men. Over the ensuing year, 43% had persistent symptoms, 71% had updated vaccination, and 36% had a self-reported re-infection. The re-infection was reported to have occurred a median of 7 months after the initial infection. The cohort was sub-divided into those with persistent LUS+ compared to those that reverted to a normal scan. The mean age was 69 ± 10 years among those LUS+ compared to 56 ± 8 years in the normalized group. The body mass index (BMI) was 32 kg/m2 in those LUS+ compared to 27 kg/m2 in the normalized group. The cohort has 6 men and 2 women in the LUS+ group compared to 4 men and 2 women in the normalized group. One LUS+ patient out of eight reportedly had been reinfected compared to four normalized patients out of six stated being reinfected. Three LUS+ patients out of eight reported having persistent symptoms compared to three normalized patients out of six complaining of continued COVID-19 symptoms.
Conclusion:
Based on the 1-year repeated LUS, for this cohort, there was a high prevalence of persistent symptoms and lung abnormalities, in those who had mild-moderate outpatient COVID-19 and received monoclonal antibody therapy. The longitudinal data collection on this cohort of COVID-19 positive outpatients may suggest that individual immune responses or viral virulence factors may play a role in B-line persistence. Certainly, future LUS results may be confounded by a previous COVID-19 infection.
Although lung involvement as a result of COVID-19 relates to mortality, 1 most studies that implicate lung involvement with disease severity and/or mortality have been conducted among hospitalized patients. 2 However, pulmonary radiographic abnormalities persist in 21% of mild-moderate outpatient COVID-19 infections, 3 and pulmonary symptoms can persist in over 50% of non-hospitalized COVID-19 patients. 4 Few studies have examined the clinical significance of abnormal lung ultrasonography (LUS+) during an initial outpatient infection. Sonography of the lung apex can be used to detect B-line artifacts associated with a COVID-19 infection. B-line artifacts are defined as hyperechoic reverberation artifacts that appear to emanate from the pleural line and extend to the bottom of the sonographic image, which are highly sensitive for interstitial edema, inflammation, or fibrosis. 5 Although such fibrosis is largely asymptomatic, the persistence of chronic B-line artifacts can confound diagnoses of decompensated congestive heart failure or pneumonia in these patients, as well as provide insights into their immune response. Although over 750 million people have recovered from COVID-19, concerns persist regarding long-term symptomatology and organ injury, especially in providing outpatient healthcare.6,7 Several groups have investigated the persistence of pulmonary sequelae on imaging and determined a relationship between persistent interstitial lung abnormalities and long-term respiratory symptoms. 8 The aim of this study was to observe the prevalence of persistent LUS+ findings, 1 year after a mild-moderate COVID-19 infection, in a cohort of high-risk outpatients that were treated with monoclonal antibodies.
Materials and Methods
A prospective longitudinal data collection, based on a previously treated group of patients, was approved by the institutional review board (IRB #22-7761). This study was a continuation of a prior data collection that was published in 2022. 9 The original study took place between October 2021 and January 2022, of which patients were likely exposed to the delta and omicron COVID-19 variants. At that time, 201 consecutive outpatients, with mild-moderate COVID-19 disease and at least one risk factor, presented within ten days of symptom onset, to receive monoclonal antibody treatment. In this group of patients, they had their lung apices evaluated for the presence or absence of sonographic B-line artifacts. Briefly, enrolled patients had qualified for monoclonal antibody treatment with one or more of the following risk factors, reported as prevalence (%) in the original study: age ≥65 years (27%), body mass index (BMI) >25kg/m2 (78%), chronic kidney disease (6%), diabetes (16%), immunosuppression (11%), cardiovascular disease/hypertension (40%), and chronic lung disease (10%). Mild-moderate COVID-19 was defined based on the Centers for Disease Control classification of COVID-19 severity. The grading consisted of outpatient individuals with saturation of oxygen >94% on room air at sea level with mild symptoms, such as cough, fever, or sore throat.9,10
Lung ultrasonography had been performed by one of four experienced physicians using the Lumify (Philips Healthcare, Andover, MA), connected to a smartphone and equipped with an S4-1 MHz transducer. LUS+ was defined as the presence of three or more B-line artifacts, in the third intercostal space, at the mid-clavicular line, of the lung apical zone. This scoring was based on prior studies of the prognostic value of this finding on a point-of-care ultrasound examination. 11 Of 201 patients, 55 (27%) of consecutive COVID-19 positive outpatients were found to have a LUS+, as part of the original study. LUS+ was found in the absence of pulmonary symptoms and later found to have prognostic value.9,12
For this phase of data collection, attempts were made to contact all the original 55 LUS+ patients and none were excluded. Patients were contacted by phone and invited to return to the outpatient clinic for a repeat LUS. They were told that they would be examined with the same ultrasound device and default settings, and this would be conducted by one of the original expert imaging physicians (BJK). Patients who agreed to return to the study were re-consented. The patient data and symptoms were anonymized from the physician examiner. Lung ultrasonography images were recorded and interpreted by the one expert during the return appointment and patients were categorized as being persistently LUS+ if either the right or left lung demonstrated three B-line artifacts, as was originally defined. At the time of their appointment, the 14 returning patients were also asked about subsequent COVID-19 reinfections, persistent pulmonary symptoms of dyspnea and cough since their initial bout, as well as COVID-19 vaccination and booster status in the intervening year.
Results
Of the original 55 LUS+ patients, 19 (35%) could not be contacted, 16 (29%) refused, six (11%) did not show (despite attempts to re-schedule), and 14 (25%) patients agreed to participate to have their apical lungs re-imaged. Patients cited the most common reason against participation as lack of time to participate. Of the 14 LUS+ patients, none had a subsequent hospitalization related to their COVID-19 infection, and all had received monoclonal antibody therapy. The mean age of the continuing cohort was 63 years (± 9 SD) and 71% were men. The 1-year repeat LUS examination demonstrated that eight out of the 14 (57%) patients had persistent LUS+ diagnostic findings. For those patients over 65 years of age compared to those younger, seven out of seven had persistent LUS+ findings compared to one out of seven younger patients. Figure 1 provides a set of LUS images and exemplifies this association by showing one younger patient (age 49) and one older patient (age 75) with resolution and persistence of B-line artifacts, respectively. Data was collected regarding gender, BMI, prior lung disease, re-infection, and residual symptoms (See Table 1). Of note, the presence of known pulmonary disease (e.g., asthma, chronic obstructive pulmonary disease, interstitial lung disease, or thoracic malignancy) was only observed in 37.5% of participants with persistent B-line artifacts, while 62.5% of those patients who had persistent B-line artifacts had no known history of prior lung disease. Despite the mild-moderate nature of outpatient COVID-19 infection, six out of 14 participants (43%) had persistent pulmonary symptoms over the subsequent year. Over the ensuing year, 71% had updated vaccination, and 36% had a self-reported re-infection. The re-infection was reported to have occurred a median of 7 months after their initial infection.
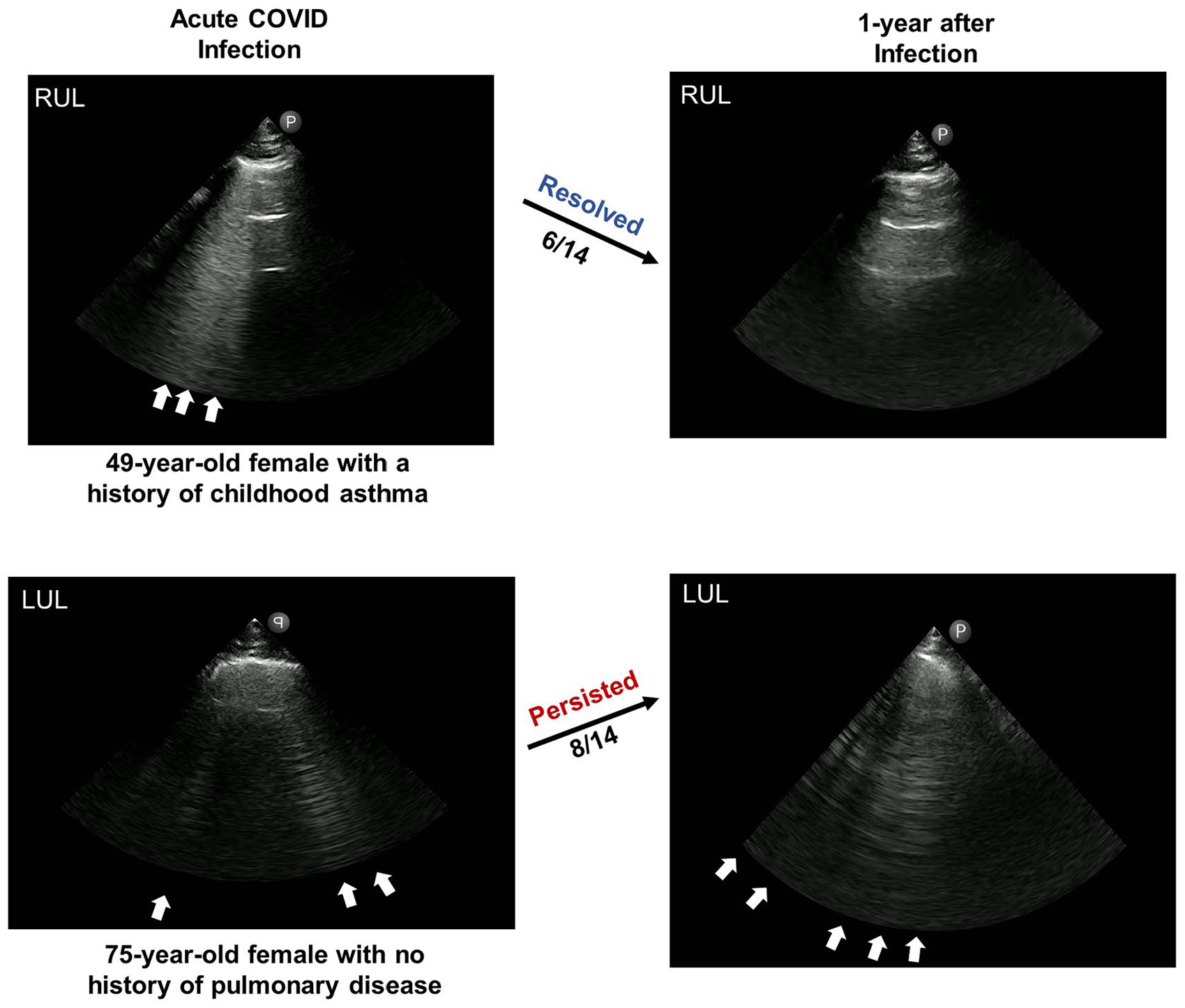
Comparing the resolution and persistence of lung sonography B-line artifacts, based on an older and younger returning patient, post-COVID-19. The top set of LUS images is recorded on a 49-year-old female with a history of asthma. Her acute LUS images are provided and compared to an image provided 1 year after a mild-moderate COVID-19 infection. The lower set of LUS images are recorded on a 75-year-old female with no prior pulmonary history, other than a mild-moderate COVID-19 infection. For comparison purposes her acute and 1 year LUS images are provided as well as a comparison with a younger counterpart. The cohort’s overall persistence of LUS+ was seen in 8/14 patients. The sonographic images were recorded at 16 cm using a 3MHz phased array transducer. RUL: right upper lobe; LUL: left upper lobe.
Demographics and Study Variables Measured Within the Longitudinal Patient Cohort, Having Been 1 Year From Their Initial Abnormal Lung Ultrasonogram (LUS+) for COVID-19.
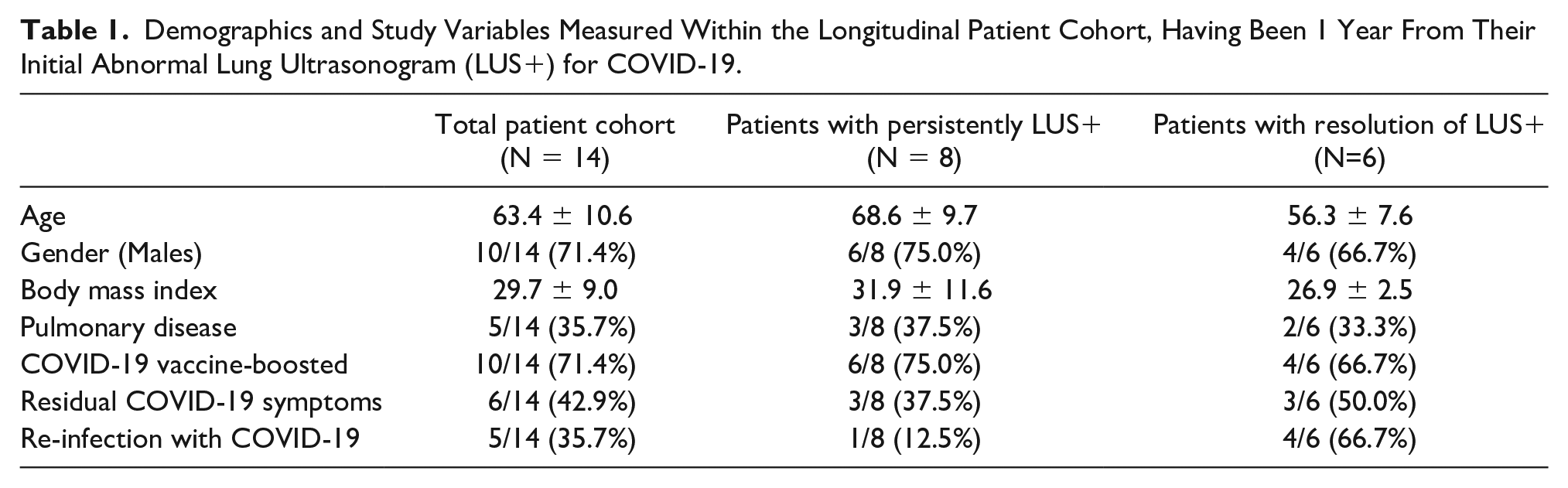
The cohort was sub-divided into those with persistent LUS+ compared to those that reverted-to-normal. The mean age was 69 ± 10 years among those LUS+ compared to 56 ± 8 years in the normalized group. The BMI was 32 kg/m2 in those LUS+ compared to 27 kg/m2 in the normalized group. The cohort has six men and two women in the LUS+ group compared to four men and two women in the normalized group. One LUS+ patient out of eight reportedly had been reinfected compared to four normalized patients out of six stated being reinfected. Three LUS+ patients out of eight reported having persistent symptoms compared to three normalized patients out of six complaining of continued COVID-19 symptoms. There were six of eight patients in the LUS+ group who were up-to-date on vaccinations, compared to 4 of 6 normalized patients.
Discussion
In this cohort of patients reporting for longitudinal data collection, all 14 received monoclonal antibody therapy for COVID-19 infection 1 year prior. In this same cohort, a persistent LUS+, was focused on the apical lung, and noted in 57%. These preliminary observations suggest that even mild-moderate outpatient COVID-19 infection may be associated with subsequent lung abnormalities, perhaps more so in those ≥65 years of age. Although the prevalence of a LUS+ in an asymptomatic patient population is unknown, one reported outpatient patient group, with 46% of patients, age ≥65 years, had a LUS+ prevalence of less than 10%. 13 The current study is unique in that it provided a repeated assessment for B-line artifacts in the same apical intercostal space 1 year later in patients enrolled in the original study. As about one-fourth of patients in the original outpatient cohort had B-line artifacts upon mild-moderate COVID-19 infection, and over half of those patients were found to be persistently abnormal in the renewed data collection, these observations may portend a high prevalence of abnormal LUS findings in those who have been infected with COVID-19.
B-line artifacts, or comet-tail artifacts, represent a “ringdown” phenomenon, due to reverberation of the ultrasound signal within thickened or edematous lung interstitium. 5 B-line artifacts are highly sensitive to an abnormal interstitium and have been observed in acute COVID-19 infection, where they likely represent edema or inflammation. Few data exist on the persistence or resolution of these diagnostic findings at long-term surveillance, 9 particularly after an exceedingly common, non-severe outpatient COVID-19 infection. This study reports the persistence of multiple B-line artifacts 1 year after resolution of acute disease, potentially representing chronic interstitial sequelae, consistent with radiologic evidence of ground glass opacities and fibrotic changes reported in hospitalized COVID-19 groups. 14 This cohort’s data introduces the concept that long-term pulmonary sequelae after COVID-19 infection may be related to the individual immune response to the virus, as well as the severity of the acute process. 15 This may suggest the importance of individual COVID-19 risk factors such as age, male gender, and elevated BMI, which were borne out of the early epidemiologic studies and became requirements to receive monoclonal antibody infusion and current antiviral therapy.
Limitations
As a small longitudinal cohort study from a single center, these observations have multiple limitations. The major limitation is the threats to internal and external validity, due to the research design. In addition, the longitudinal data collection on a cohort of patients was composed by sampling during a compressed time. This cohort was exposed primarily to the delta variant and were part of prolonged and changing pandemic that makes this a specific limitation to generalizability.
Another limitation to consider is that although the B-line artifacts in the current cohort are likely a result of a fibrotic response to the SARS-CoV-2 virus, a persistent smoldering inflammatory response cannot be excluded. The recognition of pre-existing B-line artifacts generated by chronic lung disease (i.e., false positives) do not explain these results, as previous lung disease was not reported in most patients. A bias may exist for this cohort due to opting to return to the study with chronic lung disease that can be arguably discounted by the lack of difference in rates between those with and without lung disease.
Recently, much interest has developed in sequelae of SARS-CoV-2 infection, the so-called “long COVID” syndrome. While the risk of “long COVID” increases with the severity of the acute infection, more than 90% of “long COVID” patient cases occur in those with a mild-moderate response to the SARS-CoV-2 virus. 16 The classic form of “long COVID-19” is characterized by extrapulmonary manifestations of brain fog and fatigue, 17 while the “pulmonary long COVID-19” subtype is characterized by prolonged dyspnea and cough. 18 This small longitudinal cohort data did not uncover an overwhelming relationship between persistent symptoms and LUS+, which may be due to a lack of statistical power or the possibility that the B-line artifacts represent inert fibrosis.
Next, this cohort’s data lacked radiographic correlation; however, similar imaging studies using computed tomography (CT) of patients suggested the persistence of pulmonary radiographic changes at 3 months after discharge, in more than half of COVID-19 patients, for those who were hospitalized. 19 A recent prospective study at 12 months after hospitalization for COVID-19 demonstrated CT evidence of persistent fibrosis in 29% of subjects. 20 While these studies provide valuable evidence of chronic lung pathology following COVID-19 infection, the majority of these studies have been conducted in post-acute COVID-19 patients or those with more severe disease, rather than outpatients experiencing sequelae from mild-moderate illness, as addressed by the current cohort.
Conclusion
These diagnostic findings document a persistent LUS+ in over half of this cohort of patients with mild-moderate COVID-19 treated with monoclonal antibody infusion, 1 year after initial infection. Persistent B-line artifacts on LUS, could confound the diagnosis of decompensated congestive heart failure or pneumonitis in the future for what could be a sizable number of patients who were previously infected with only mild-moderate COVID-19. More research is needed to determine patient and disease characteristics that may result in persistent interstitial abnormalities on LUS.
Footnotes
Ethics Approval
Ethical approval for this study was obtained from the institutional review board (IRB #22-7761).
Informed Consent
Written informed consent was obtained from all subjects before the study.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used during the study.
Trial Registration
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NIH NCATS Grant #UL1TR002550 for statistical analysis.