
Abstract
Objective:
When measuring the liver sonographically, liver volume measurement (LVM) is not routinely performed, though considered the gold standard on CT. The objective of this study is to encourage the sonography community to obtain an LVM instead of a single linear measurement on ultrasound, so as not to subject patients to the potentially harmful radiation exposure of a CT scan when assessing liver size. This study compared the consistency and accuracy between expert and novice sonographers in obtaining an LVM on sonography.
Materials and Methods:
Both groups obtained linear and LVM on 30 participants and calculated LVM using the formula Liver Volume (cc) = 343.71 + (0.84 × ABC).
Results:
Both groups took longer to obtain LVM than linear, P < .0001. Novices and experts obtained an LVM in a similar amount of time. More consistency was observed among experts when scanning participants in the lower BMI ranges. Novice sonographers’ LVMs were consistent with experts’ only in the lowest BMI range of this study.
Conclusion:
Groups acquired LVM in similar amounts of time, showing LVM is easy to teach and learn, and has good inter-rater reliability. Difference for both groups to obtain LVM over linear was only 38 seconds. Consequently, it is prudent to incorporate LVM into abdominal ultrasound protocols.
Key Takeaways
The Childs’ sonographic liver volume formula can be confidently employed to measure the liver volume equally accurately and consistently to the accepted gold standard of CT, but without harmful ionization radiation exposure.
LVM can be acquired in a timely manner and will not impact the overall time taken to perform an abdominal sonogram.
Sonography labs should incorporate the LVM into all abdominal ultrasound examinations.
The liver is the largest internal organ in the human body. It is responsible for many important physiologic functions, including detoxifying chemicals, and metabolism of proteins, fats, vitamins, and carbohydrates.1,2 It is important to accurately, consistently, and reliably measure the liver, as any changes in size can indicate an underlying pathology or disease process.3,4 Many imaging modalities are used to assess liver size. Computed tomography (CT) is considered the gold standard in accurately measuring the liver, primarily because it employs a volume measurement. However, CT presents with significant disadvantages, including cost, ionizing radiation exposure, and the use of contrast materials, which may have adverse side effects in patients. 5
Currently with sonography, a single linear 2D measurement is commonly employed to obtain a liver measurement. However, there is no uniform consensus on how to measure the liver using a single linear measurement between sonographic clinical laboratories. 6 It has been observed that some clinical laboratories perform the linear measurement using the dome-to-tip (DT) approach; others use anterior-to-posterior (AP) method; and still others use the superior-to-inferior measurement. Clearly, a more reliable and accurate technique is essential for calculating a liver measurement consistently among sonographic clinical laboratories.
Sonographic techniques and formulas have been successfully developed to measure the liver volume.7,8 Childs et al developed a liver volume formula for assessing liver volume with sonography, that utilizes the same three planar measurements used in calculating liver volume with CT. 7 In addition, research has been done showing near perfect agreement between a sonographic and a CT volume measurement. 9 Despite this, most sonographic clinical laboratories still perform the single linear measurement. The reasons for this may be because laboratory administrators or sonographers feel that obtaining a single linear measurement is more time efficient than the liver volume measurement (LVM), and/or the possibly poorer inter-rater reliability of obtaining an accurate and consistent volume measurement. These potential concerns are particularly relevant to novice sonographers.
The objective of this study, therefore, was to compare how long it takes for both seasoned (expert) and novice sonographers to obtain a liver volume measurement as compared with a linear measurement. The aim was to show the time efficiency, for any sonographer, to obtain an LVM and evaluate the inter-rater reliability of obtaining this more accurate and consistent method for sonographic measurement of the liver. In this way, this endeavor was to reduce or eliminate the frequency of CT examination referrals, which would minimize patients’ exposure to ionizing radiation, while simultaneously acquiring the gold-standard liver volume measurement with sonography.
Materials and Methods
This study was approved by the State University of New York Downstate Health Sciences University’s (SUNY DHSU) Institutional Review Board. An inter-rater research study design was used.
This study was conducted in the Diagnostic Medical Imaging (Sonography) program’s scan lab at SUNY DHSU. Two experienced registered sonographers with 19 and 9 years of experience studied and practiced Childs et al’s liver volume measurement techniques. Then, during two 30-minute sessions, two experienced sonographers trained two novice sonographers (performing peer scanning) on the proper method for obtaining sonographic images/planes as well performing the three required measurements in order to calculate liver volume. These imaging measurements are based on Childs’ formula: Liver Volume (cc) = 343.71 + (0.84 × ABC).7,8 (See Figures 1, 2, and 3, which corresponds to the ABC of this equation.) Novice sonographers are defined in this study as entry-level sonographers preparing for registry certifications and have successfully completed 1 year of abdominal sonography clinical training.
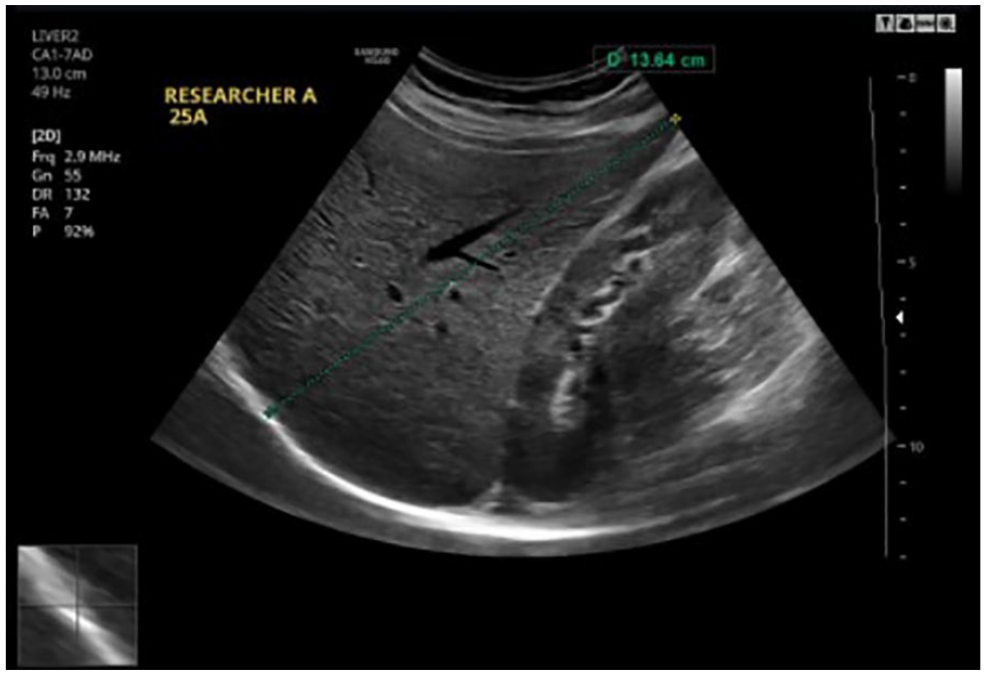
A sagittal sonographic image of the right lobe of the liver with a dome-to-tip (DT) measurement.
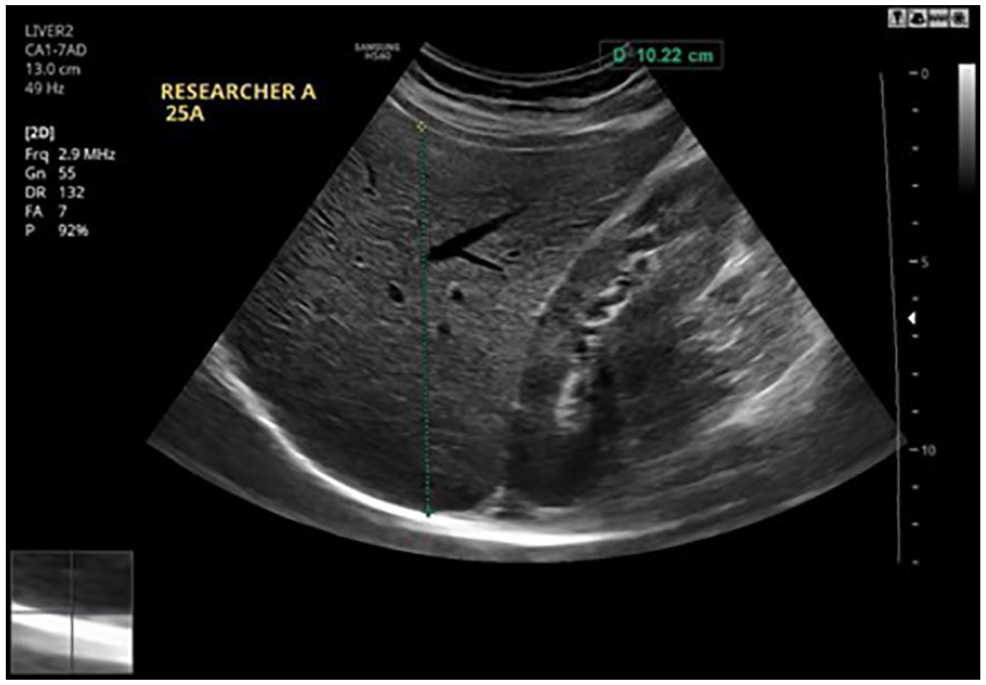
A sagittal sonographic image of the right lobe of the liver with an anterior-to-posterior (AP) measurement.
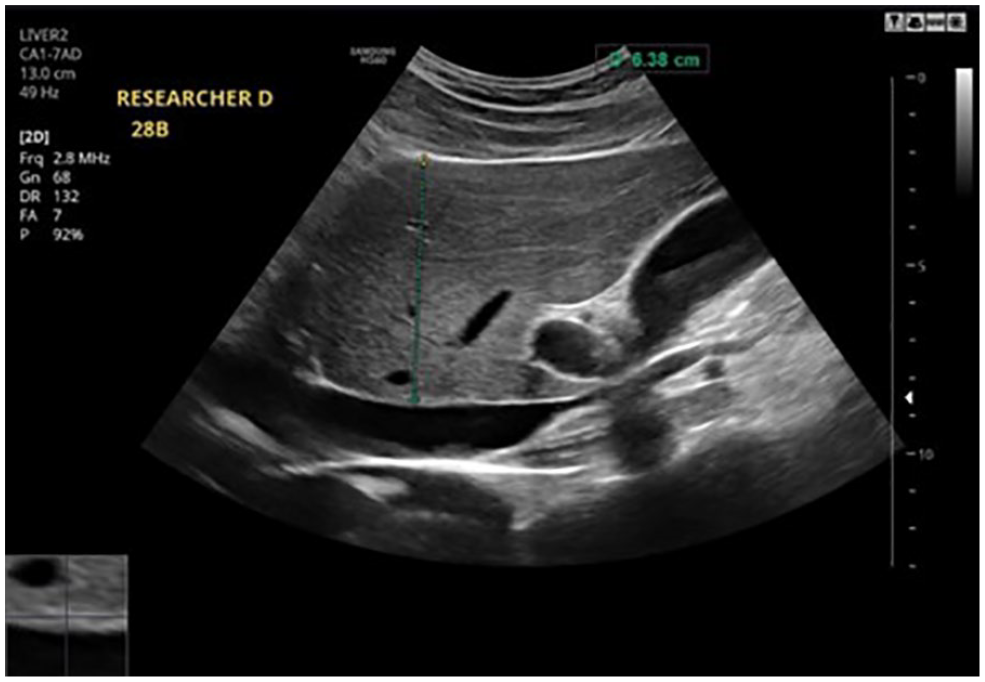
A sagittal sonographic image of the left lobe of the liver with an anterior-to-posterior (AP) measurement.
A third novice sonographer, the timekeeper, was trained on how to keep time, accurately record the measurements, and calculate the liver volume using Childs’ formula. At the end of the training sessions, the novices were able to obtain the proper planes for these three linear liver measurements.
Participants were recruited through informational flyers posted in various locations throughout the campus, utilizing a sample of convenience. Individuals who were interested in study participation were vetted for eligibility, using a screening tool. This questionnaire inquired about participant age, gender, height, weight, pregnancy status, and history of liver disease. Inclusion criteria for participants were members of the SUNY DHSU community, aged 18 and above, who had a body mass index (BMI) of less than 25, no known history of liver disease, and a negative pregnancy status, as any of these factors could have skewed the results.3,10 BMI was calculated using the formula (weight (lbs.) × 703 / height (in.)).7,8 Upon determining eligibility, each participant was then scheduled for the study appointment. Participants were instructed to fast for 6 to 8 hours prior to their appointment in order for the sonographers to be able to obtain optimal sonographic liver images. Participants reviewed and signed the informed consent document, were advised that the study was voluntary, and that they could decline participation at any time without penalty or consequence. Any health information collected was deidentified and anonymized. Study participants were positioned in a left posterior oblique (LPO, 45° angle) position, using a bolster to anchor their position, for all liver images and measurements (see Figure 4).
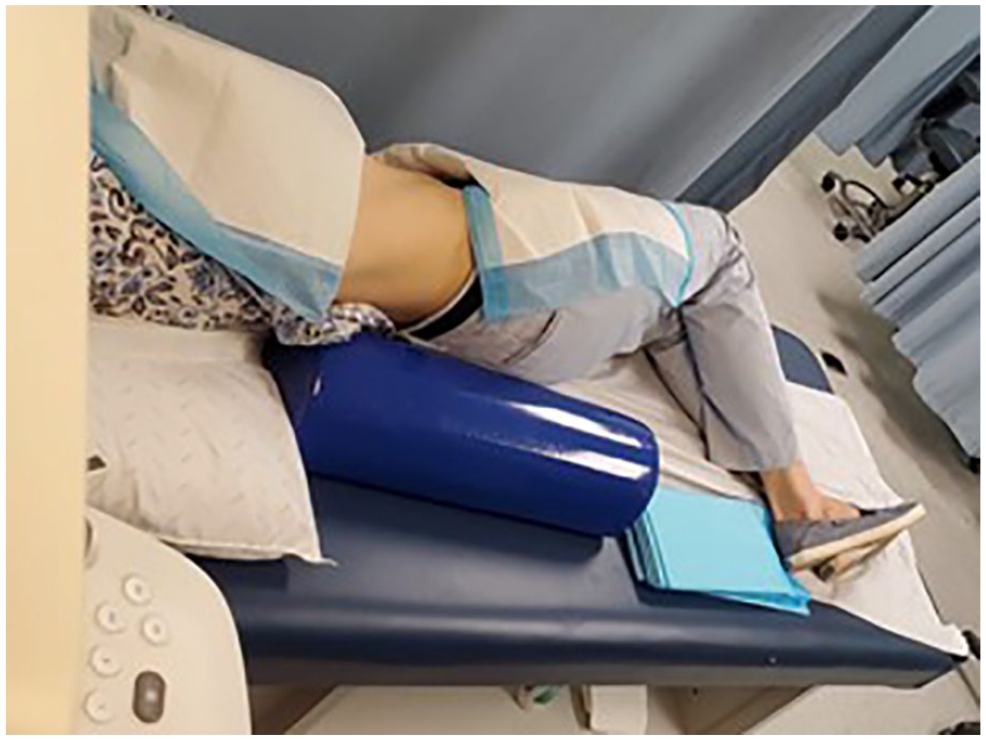
An illustration of a patient in the left posterior oblique position.
For both the right and left lobe images the transducer was angled slightly to the patient’s right. The right lobe of the liver was imaged by placing the transducer along the participant’s midclavicular line in sagittal plane (see Figure 5).
An illustration of the transducer angled toward the midclavicular line of the patient.
The liver took up 75% of the screen and included a portion of the right kidney. Two measurements were obtained from this image: Measurement A was taken from the dome of the liver, at the right hemidiaphragm, including as much of the tip of the liver as possible (see Figure 1). The time was paused and recorded by the timekeeper (accounting for the time to acquire and measure this initial image and measurement). The time was then resumed for measurement B, which was obtained using the same image, but measuring from the anterior surface of the liver to its posterior border, at its thickest dimension (see Figure 2). With the timer still running, the sonographer then acquired a sagittal sonographic image of the left lobe of the liver along the xiphisternal angle, including the main portal vein (see Figure 6).
An illustration of positioning the transducer at a xiphisternal angle.
Measurement C was then taken from the anterior border of the left lobe of the liver to its posterior surface, excluding the portal vein (See Figure 3). At the completion of measurement C, time was stopped for the second time and then the total time for all three image acquisitions and their respective measurements were recorded. Each of the four sonographers (two expert and two novice) repeated this entire process twice on each participant to control for inter-rater reliability.
A Samsung HS60 ultrasound equipment system (Seoul, South Korea) was used for all sonographic images and measurements. A P value of .05 was selected a priori to determine statistical significance.
Results
The study participants included 30 healthy individuals, of which 20 were female and 10 were male. The participants’ liver measurements, captured by each sonographer, were compared and analyzed for consistency, accuracy, and time efficiency. The liver volume was calculated using Childs’7,8 liver volume formula. A one-tailed t test and analysis of variance (ANOVA), as well as descriptive parameters were utilized to analyze the data. These tests compared the time it took expert and novice sonographers to obtain the linear versus volume measurements, respectively. The difference in volume measurements between expert and novice sonographers was also analyzed.
Based on the data, it took the novice sonographers an average of 32.33 seconds to obtain the linear measurement, and an average of 69.91 seconds for the volume measurement (see Figure 7). The expert sonographers took an average of 27.76 seconds to acquire linear measurement and 66.32 seconds for the volume measurement. The novice sonographers took an average of 4.57 seconds more than the expert sonographers to measure the single linear measurement, and 3.59 seconds more to capture the volume measurement. The t-test results indicated that the experts were faster in obtaining a linear measurement than the novices (P = .039). The difference was not statistically significant in the volume measurement between experienced and novice sonographers (P = .076).
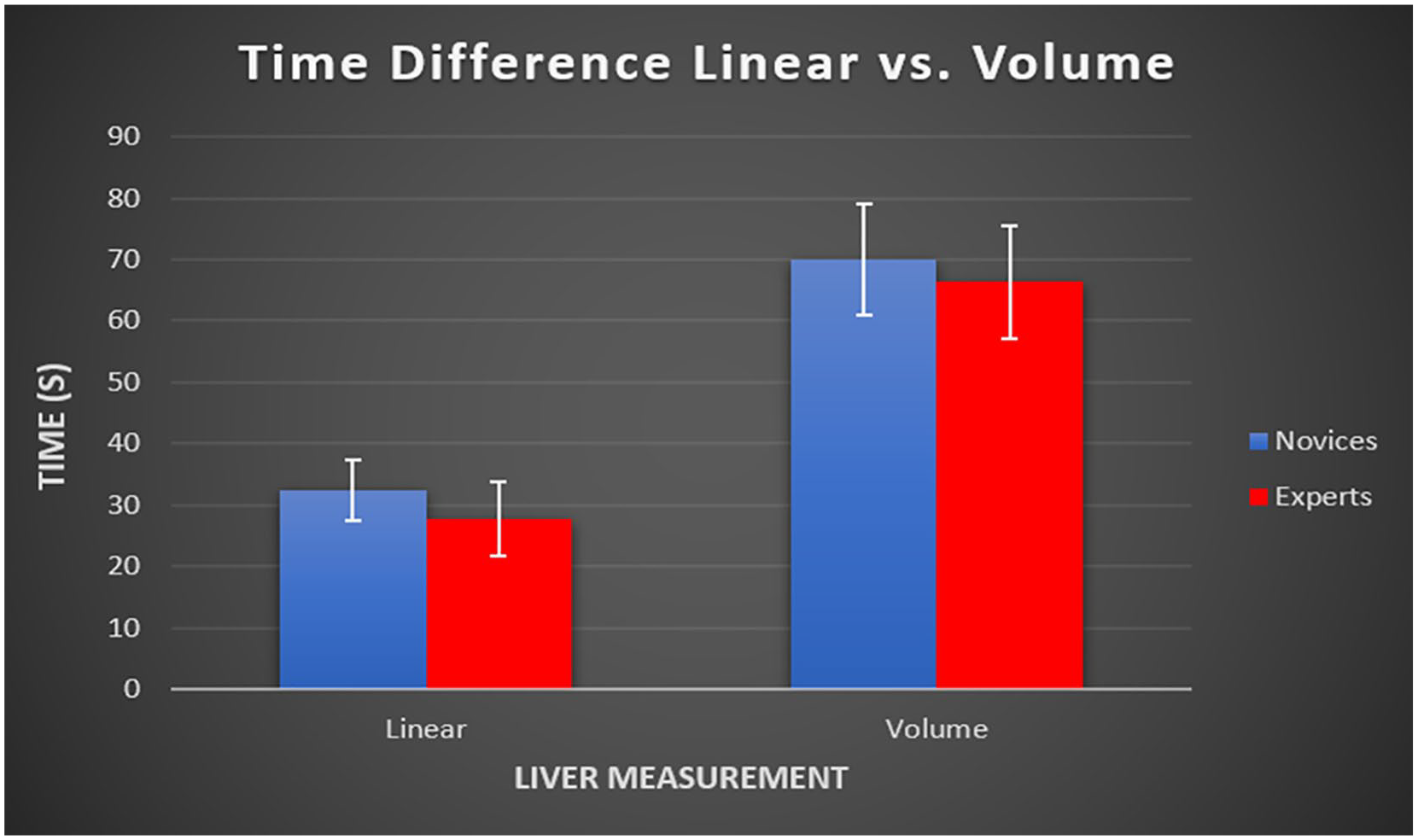
A box plot of the average time for linear versus volume for expert and novice sonographers.
The variability in volume measurements made by experienced sonographers when scanning participants in the BMI ranges of 17 to < 23 was less than the variability of measurements in patients from the highest BMI category (Table 1 and Figure 8). This result was demonstrated by ANOVA, F(3,26) = 4.06, P = .0172, and post hoc analyses showed the highest BMI group difference was significantly larger than the differences for groups 19 to <21 and 21 to<23 (Tukey HSD P = .036, P = .019, respectively).
Data Analysis for Volume Differences Versus BMI Range for the Expert Group.
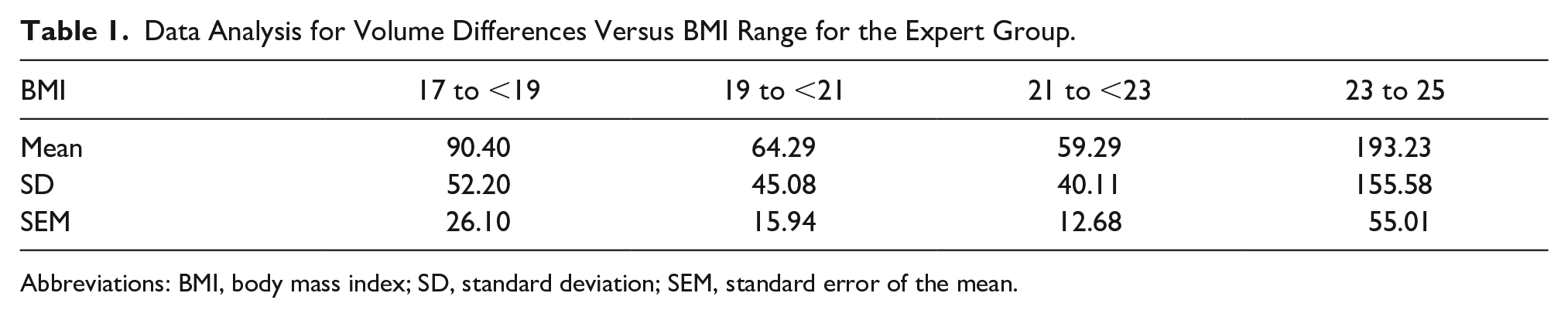
Abbreviations: BMI, body mass index; SD, standard deviation; SEM, standard error of the mean.
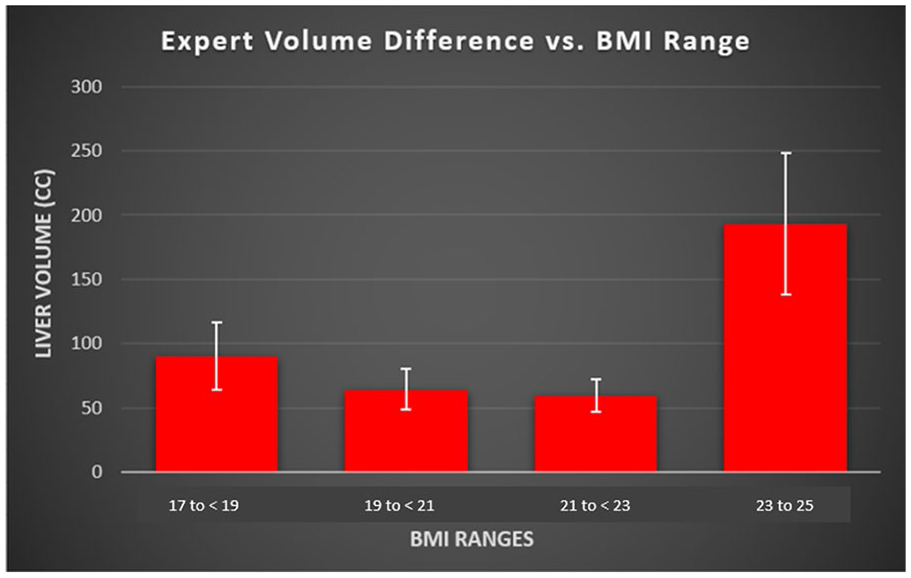
The box plot comparison of liver volume difference between two expert sonographers in relation to four ranges of BMI. BMI, body mass index.
As for the novice sonographers, the differences in their volume measurements varied greatly throughout all BMI ranges (See Table 2 and Figure 9). Variability between the novice sonographers was always higher than the expert sonographers.
Data Analysis for Volume Differences Versus BMI Range for the Novice Group.
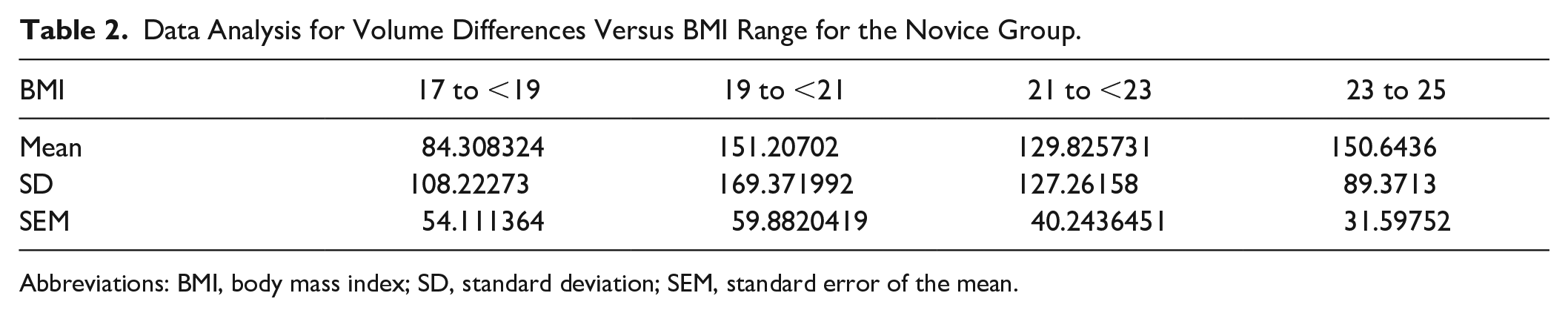
Abbreviations: BMI, body mass index; SD, standard deviation; SEM, standard error of the mean.
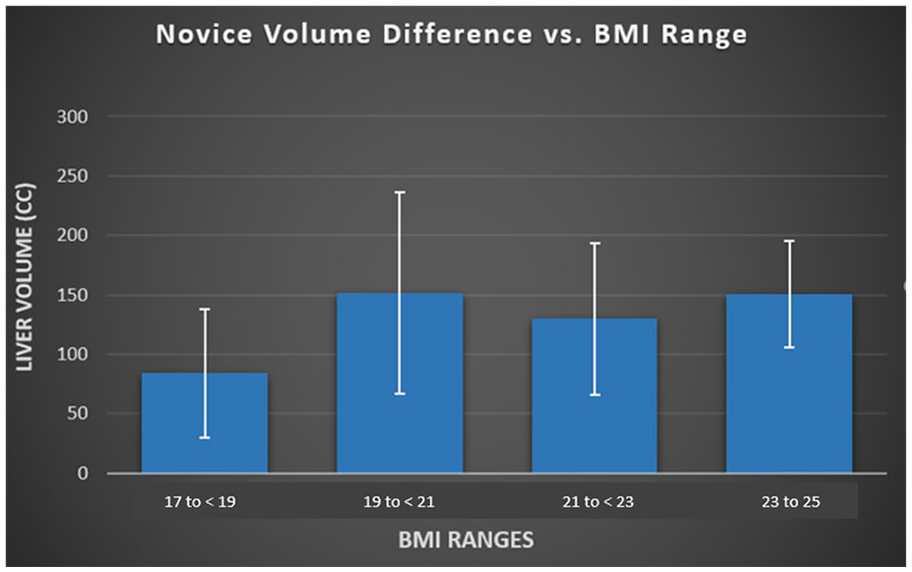
The box plot comparison of liver volume difference between two novice sonographers in relation to four ranges of BMI. BMI, body mass index.
A t test was performed to compare the volume measurement among each BMI range between the expert and novice sonographers. The LVM was the most consistent in the BMI range of 17 to <19 between the novice and expert sonographers (Figures 8 and 9).
There was a statistically significant increase in the time that it took for the volume measurement versus the linear measurement, for both expert and novice sonographers, with P < .0001 (see Figure 7). The average time for sonographers in both groups to obtain a linear measurement was 30.05 seconds. The average time taken for both sonographer groups to acquire a volume measurement was 68.12 seconds. This demonstrates that it took 38.07 additional seconds to obtain an LVM (See Figure 7) across both groups. Expert sonographers were significantly faster than the novice sonographers in obtaining the linear measurement (P = .039). However, both sonographer groups obtained the LVM in a similar amount of time (P = .076). The greatest variation in LVM among expert sonographers was observed in the highest BMI range of this study. Both sonographer groups showed consistency in LVM among the participants in the lowest BMI range.
Discussion
It is of great clinical importance to find the most accurate method to assess liver volume with sonography to establish a range of normal diagnostic values. Liver volume is a better assessment tool than a linear measurement, as it represents the entire liver rather than a single plane. 9 In a study done by Riestra-Candelaria et al, there was a lack of standard reference values for sonographic measurements of the liver. 11 Childs et al developed an equation that was straightforward and could easily be applied in clinical practice. The ideal equation was as follows: Liver volume (cc) = 343.71 + (0.84 × ABC), where A = (Left Lobe AP), B = (Right Lobe Dome-to-Tip (DT)), and C = (Right Lobe AP).7,8 Izranov et al then compared the Childs et al equation with the true liver volume using a water displacement method. In that study, the liver was extracted from the abdominal cavity of 34 cadavers. The liver was weighed and then placed in a container filled with water to determine the actual liver volume by measuring the water displacement volume. For the calculated liver volume, the right lobe of the liver (RLL) and left lobe of the liver (LLL) of the liver specimens were dissected. The liver width was measured at the outermost lateral aspect of both lobes of the liver in a horizontal plane. Results showed only a 1% deviation from the comparison. Therefore, Izranov et al showed the Childs et al liver volume formula was accurate in calculating liver volume sonographically. 12
Childs et al7,8 reported BMI to be an important factor incorporated into their equation. Moreover, Silva et al also stated that BMI was the most essential factor of liver diameter. In their study, to validate the influence of BMI over liver size, two percussion liver measurements from 81 adult volunteers (43 females and 38 males) were compared with ultrasound liver measurement at the percussion site.13,14 Participants with a high body mass index, or those with a BMI of greater than 25 kg/m2, proved more difficult in obtaining an accurate liver measurement.13,14
Therefore, based on the literature, the current study excluded participants with a BMI of greater than 25 kg/m2 from the study. Notably, the expert sonographer group in this study had the most variability in volume measurement in the highest BMI range (23–25) of the participants. Also, upon scanning the current study participants, it was noticed that certain body compositions were easier to scan than others. On a sonogram, participants with less body fat displayed more well-defined liver borders and echotexture. These characteristics made the three liver images and measurements easier to acquire.
Another study by Childs reported other factors that may have affected the results of their study, namely, a small sample size, sample of convenience, and/or operator dependence. Because their sample size was small (n = 12), each participant was re-scanned for each set of liver measurements, which strengthened the study. 14 The current study also had a relatively small sample size (n = 30); therefore, it was determined that each of the participants would be measured twice, to improve statistical outcome, specifically intra-rater reliability. Another limitation of Childs’ study was the inclusion of participants with liver pathology, causing inconsistencies in their measurements, since pathologic livers have different measurements and appearances than healthy ones and skews measurement results. Therefore, in the current study, participants were excluded with known liver disease to avoid these potential discrepancies. The time it took to obtain a volume measurement of the liver was greater than that of the single linear measurement. The results of this study showed a statistically significant increase in the time needed to capture the LVM versus the single linear measurement by both expert and novice sonographer groups. However, the increase in time needed to obtain the LVM over the linear measurement for both groups was only 38 seconds. As such, it is worthwhile for general sonographic clinical laboratories to incorporate the LVM into the liver measurement protocol of routine abdominal sonography. This will provide a more accurate liver size assessment and be more consistent with the current gold standard of liver volume measurement on CT,1,2 without compromising time efficiency.
Based on the results of this study, sonographer experience correlated directly with efficiency and speed. Thus, the linear measurements from expert sonographers were obtained more quickly and with more consistent results than their novice counterparts. However, novice sonographers were able to acquire volume measurements in a similar amount of time as expert sonographers. This shows that the volume measurement is easy to teach, easy to learn and has good inter-rater reliability. It should be noted that the two short training sessions to teach novices how to measure the volume of the liver were sufficient to learn how to obtain accurate and consistent LVMs. With a small amount of training and practice, novice sonographers would be able to acquire an accurate liver volume measurement comparably to their expert counterparts.
Another finding of this study was that BMI was not shown to be a predictor of obtaining an accurate and consistent LVM. However, the BMI range of 21 to <23 in the expert group came close to statistical significance, showing a P value of .09.
It is also worth mentioning that during the scanning sessions of this study, the tip of the right lobe of the liver was sometimes more difficult to visualize in participants in the higher BMI ranges. As such, it took more time to obtain any measurements on these patients. However, experts and novice sonographers were able to obtain the linear and volume measurements within the same amount of time.
Limitations
This research study has several limitations, including a small convenient sample size, threats to both internal and external validity, and self-reported height and weight used to calculate BMI. For future studies, a handheld body fat loss monitor may be utilized to improve accuracy in BMI calculations. This device precisely measures body fat percentage and BMI. Alternatively, researchers can record height and weight using the same standard scales and height charts for each participant. Another possible limitation that could have affected inter-rater reliability is that the participants in this study did not receive a follow-up imaging examination to verify that the expert measurements were accurate.
Conclusion
As is evident from this research, both sonographer groups acquired linear measurements and LVM in similar amounts of time, showing LVM is easy to teach, learn, and has good inter-rater reliability. Although novice sonographers were somewhat slower than experts in obtaining a volume measurement, the increase in time taken for both groups to obtain a liver volume measurement as compared with its linear counterpart was only 38 seconds. Moreover, sonography has already been shown to match the volume measurement to that of CT in accuracy and reliability. 9 As such, it seems practical to teach and use volume measurements of the liver with sonography.
Footnotes
Acknowledgements
The authors acknowledge SUNY Downstate Health Sciences University faculty members, Dr Rena Orman and Dr Mark Stewart for their invaluable contributions to this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.