
Abstract
Objectives:
The aim of this article is to offer insight into how professionals and patients understand and experience multimorbidity and how these accounts differ, and how they affect attitudes and engagement with self-management.
Methods:
Semi-structured interviews with 20 primary healthcare practitioners and 20 patients with at least 2 long-term conditions (including coronary heart disease, diabetes, osteoarthritis, chronic obstructive pulmonary disease and depression). Thematic analysis was used, and themes were identified using an open-coding method.
Results:
Practitioners associated multimorbidity with complexity and uncertainty in the clinic, leading to emotional strain and ‘heart sink’. Patient accounts differed. Some described multimorbidity as problematic when it exacerbated their symptoms and caused emotional and psychological strain. Others did not perceive multimorbidity as problematic. Self-management was seen by practitioners and patients to be a key element of managing multiple conditions, but drivers for prompting and engaging in self-management differed between patients and practitioners.
Conclusion:
This study suggests that recommendations for clinical practice for multimorbid patients should take into account the gap in perceptions between practitioner and patients about experiences of multimorbidity. Not least, practice would need to reflect the tension between practitioners’ and patients’ accounts about the role and benefits of self-management in the presence of multimorbidity.
Introduction
A number of studies show that older patients with long-term conditions generally have more than one condition1,2 (often referred to as multimorbidity). People with multimorbidity are predominately seen in primary care, and prevalence is set to increase. In the United States, 60 million people have multimorbidity, expecting to rise to 81 million by 2020, 3 and about two-thirds of total US healthcare spending may be devoted to these patients. 4 It is estimated that around 58% of patients attending general practice in the United Kingdom have multimorbidity and that they account for around 78% of all consultations. 4 People with multiple long-term health conditions were responsible for the greatest burden of disease in most Organisation for Economic Co-operation and Development (OECD) countries (34 countries who signed the Convention on the OECD) in 2011, and their cost and prevalence will increase in the future as populations age. 5
Current descriptions of multimorbidity tend to use a count or additive model whereby multimorbidity is construed as a state arising from the coexistence of two or more long-term health conditions. 6 However, conceptualising multimorbidity this way does not take into account the differentiated nature of multimorbidity, 7 the differences between related and unrelated conditions, synergistic or antagonistic conditions, or variation in the impact of multimorbidity on the functional capacity of the individual. Multimorbidity may also have an impact on individual conditions, or lead to new complications arising from multimorbidity itself. 8
Despite multimorbidity increasingly becoming the norm rather than the exception, 9 services of National Health Service (NHS) are generally not organised around the needs of patients with multimorbidity. 10 In high income countries with ageing populations and shrinking health budgets, there are growing financial pressures to manage increasing numbers of multimorbid patients more effectively and efficiently. 11 The use of disease-specific guidelines is aimed at improving care (including self-management) for patients with long-term conditions, but these guidelines are generally not aimed at patients with multimorbidity. 9 Use of single disease–based guidelines to treat multimorbidity may lead to burdensome and inappropriate treatment. 12
It has been suggested that health services, especially primary care, cannot continue to be organised around single conditions and that policy and practice need to be reconfigured to meet the challenge posed by multimorbidity.1,9 To understand how services might be more effectively delivered to cope with this growing problem, first, we need to understand in more detail how practitioners and patients conceptualise multimorbidity and how they understand the impact on important aspects of care such as self-management. The aim of this article is to offer insight into these issues and describe the implications for the development and delivery of new models of care.
Methods
This study was nested within a prospective cohort study examining engagement in and predictors of self-management in multimorbidity. The cohort study surveyed 1500 patients with at least two of five exemplar conditions: coronary heart disease, diabetes, osteoarthritis, chronic obstructive pulmonary disease and depression. These exemplar conditions were selected because they are highly prevalent in primary care populations, have varied symptomatology, and present patients and practitioners with different treatment and management challenges. Patients were identified from the disease registers of four general practices in Greater Manchester. A total of 20 patients were selected from 222 patients who responded to the survey, indicating that they would like to be considered for interview. Patients were purposively sampled on number and type of long-term conditions, age, gender and postcode deprivation score. This was to ensure that we recruited a varied group of patients who shared key demographic and clinical characteristics of interest. Four patients were unobtainable or unavailable for interview and were replaced with patients who had similar characteristics (e.g. age, gender and number of conditions). Practitioners (n = 15) were initially recruited from the practices taking part in the survey and the remainder from three other practices using snowball sampling. Practitioners were purposively sampled on deprivation (taken from the general practitioner (GP) practice postcode), practitioner role (e.g. partner/salaried GP/nurse) and gender. Tables 1 and 2 show the individual characteristics of each of the interview participants. Table 3 shows a summary of the patient sample characteristics.
Patient characteristics.
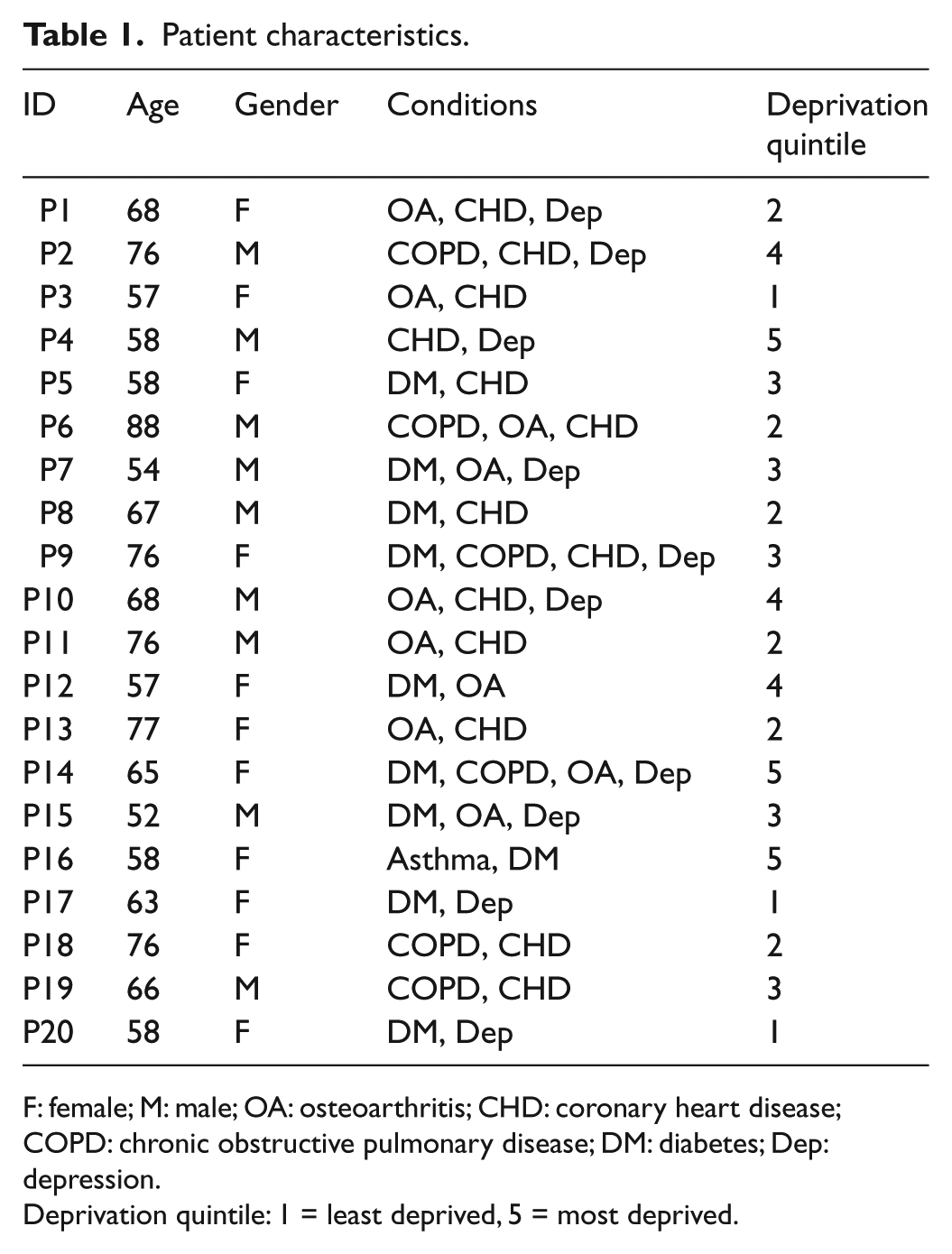
F: female; M: male; OA: osteoarthritis; CHD: coronary heart disease; COPD: chronic obstructive pulmonary disease; DM: diabetes; Dep: depression.
Deprivation quintile: 1 = least deprived, 5 = most deprived.
Practitioner characteristics.
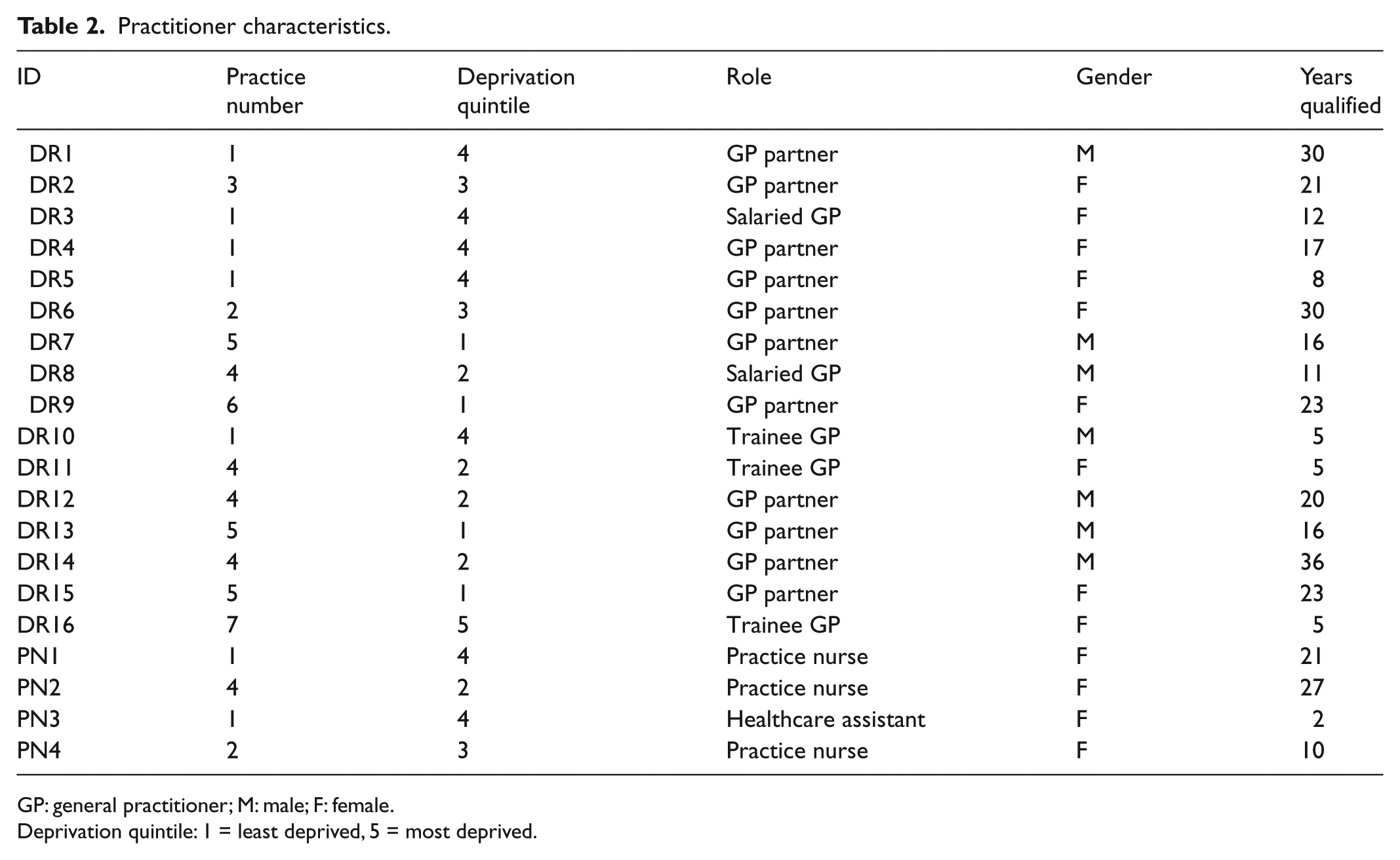
GP: general practitioner; M: male; F: female.
Deprivation quintile: 1 = least deprived, 5 = most deprived.
Patient sample.
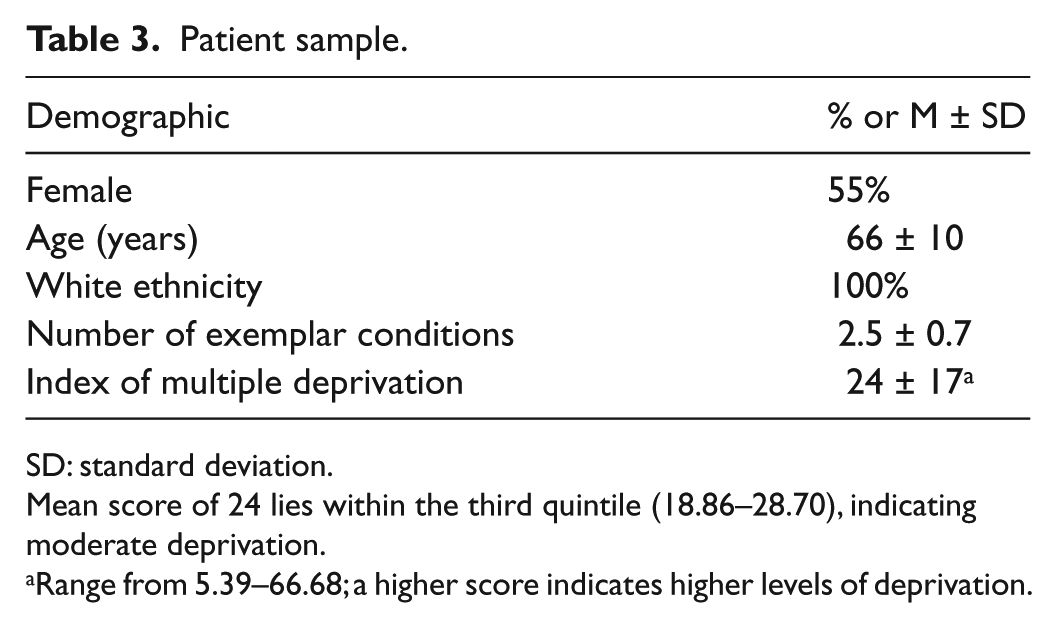
SD: standard deviation.
Mean score of 24 lies within the third quintile (18.86–28.70), indicating moderate deprivation.
Range from 5.39–66.68; a higher score indicates higher levels of deprivation.
Patient interviews were focussed around exploring their experiences of living with multiple long-term conditions, their understanding of self-management and its role in their health management, including eliciting accounts of their experience with healthcare services and supported self-management programmes. The term ‘multimorbidity’ was not used in the patient interviews. Instead, patients were asked to describe the impact of their health conditions on their daily routines and on their ability to effectively manage their health (Appendix 1). Practitioner interviews focussed on exploring their experiences of working with patients with multimorbidity and how it impacted on their clinical work, their experiences of promoting self-management and their perceptions of how self-management was regarded by patients, as well as on their knowledge of and experiences with supported self-management programmes (Appendix 2). An initial pilot interview was carried out by each of the interviewers (C.K. and L.F.). Sample recruitment continued until data saturation was reached, and no new themes emerged from the data.
All interviews were audio-recorded with consent and fully transcribed. Interviews lasted between 30 and 57 min (mean 38 min) for practitioners and between 10 and 72 min (mean 37 min) for patients. Field notes were made following the completion of each interview and reread for the purposes of data familiarisation. Analysis was conducted according to the constant comparative method, 13 whereby analysis was carried out concurrently with data collection so that emerging issues could be iteratively explored. Development of conceptual themes was inductive. Following data familiarisation, emerging themes were organised into a theoretical framework. 14 Transcripts were then indexed against this initial coding and checked to ensure that there were no significant omissions prior to framework refinement, data charting and synthesis. Themes were constantly compared within and across cases, paying particular attention to negative cases and possible reasons for differences.
Analysis was carried out by four researchers from different backgrounds (general practice, health services research and health psychology) to increase trustworthiness of analysis. 15 Transcripts were analysed independently and coded by hand; emerging themes were discussed until consensus was achieved, and a coding framework that included higher level themes and relevant data was assembled in Microsoft Excel. Each transcript was analysed individually and then in groups, with the healthcare professional transcripts analysed separately from the patient transcripts but with comparisons made across data sets. Quotes are used to illustrate key themes. (Participant codes: DR = GP, PN = practice nurse, P = patient; Key to conditions: OA = osteoarthritis, CHD = coronary heart disease, COPD = chronic obstructive pulmonary disease, DM = diabetes, Dep = depression).
Ethical approval was granted by Greater Manchester North Ethics Committee on 12/09/2011 (ref.: 11/NW/0563).
Results
Practitioner’s experiences of multimorbidity
Practitioners identified and characterised multimorbidity by drawing on narratives about how encounters with patients with multimorbidity challenged their clinical routines and challenged their ability to manage these patients effectively.
When talking about their interactions with patients with multimorbidity, three main issues emerged from the data:
Complexity – in terms of presentations, symptom management and patient characteristics;
Uncertainty – in terms of treatment and management;
Emotional strain – associated with managing complex patients who show little improvement or willingness to engage in their own care.
Complexity
Practitioners all stated that dealing with multiple conditions increased complexity. GPs highlighted that they often used clear and protocolised guidelines when dealing with single conditions, but lacked guidance and clear referral pathways when dealing with multiple conditions at once: Yes. I think a single long-term condition is much, much easier to deal with. From the point of interactions and how they feel and perceive themselves. Definitely, thinking of patients who unfortunately have a heart problem, but the problem’s been investigated at the hospital, dealt with, and there’s a clear plan of action as opposed to adding another scenario to that definitely. (DR2, female (F), GP partner)
Multimorbidity introduces a level of complexity about patient presentations and symptoms, with practitioners finding it difficult to separate out conditions to determine which symptoms relate to which condition, and to recognise the development of new conditions: And the challenge also is are those symptoms due to the medication or is there another physical symptom going on? Does she warrant another referral for investigation? (DR2, F, GP partner)
Some GPs described how multimorbidity also made it more difficult to process information and effectively monitor or predict potential problems: … treating becomes more complex but then I also think explaining things, watching things and being aware of all the different possible things that could happen physically, becomes more difficult so the side effects from all the drugs, all the interactions they all become more difficult. (DR16, F, trainee GP)
Complexity also framed relationships with patients with fatalistic attitudes to health and disease, making it difficult for nurses to engage some multimorbidity patients with advice about their health. When asked about what factors might impact on treating patients with multiple conditions, one nurse stated, You get a lot of patients who are in denial, don’t want to know, aren’t bothered and they’ll turn around and say ‘I don’t care, I’ve got this, I don’t care I’m just going to live my life to the full’. (PN2, F, practice nurse)
Uncertainty
Multimorbidity was seen to be inextricably linked to treatment complexity, which was essentially characterised by uncertainty about treatment decisions. This led to some GPs describing clinical uncertainty in treating patients with multimorbidity. This characterisation was not limited to GP trainees but also applied to senior GPs with many years of experience: Struggling yeah, it’s just not feeling that confident, not feeling that confident about managing one condition, but realising it has an impact on the other one, affecting it adversely. I’m not sure what balance to strike. (DR12, male (M), GP partner, 20 years qualified)
Much of this uncertainty was a result of the difficulties in prescribing appropriately and using disease-specific guidelines that do not take into account interactions owing to multimorbidity. For example, practitioners found it difficult to ensure that patients were prescribed all recommended medications without risking adverse interactions. But quite apart from concerns about adverse drug interactions, practitioners also encountered problems when monitoring conditions that may be unrelated, or where management is antagonistic between conditions. When asked whether working with patients with multiple conditions as opposed to those with single conditions presented specific challenges, a nurse recounted that … you might be thinking of giving them something but then you have to consider what other conditions they’ve got and the potential side effects and interactions and also whether what you’re going to put them on, is it going to cause a problem with another existing condition. So, yeah, they’re not straight forward. (PN1, F, practice nurse)
Some GPs emphasised that in the presence of such complexity and uncertainty, general practice became more reliant on a capacity to adapt existing evidence-based approaches to fit the heterogeneous needs of patients with multimorbidity: If you’ve just got atrial fibrillation and you fit in with the NICE Guidance then you can apply the evidence can’t you, its protocol driven medicine. So I think that’s the difference, when you look at protocol driven medicine, […] whereas really what you’ve got to try and do is use your acumen and your professional judgement to see to what extent you can apply these protocols to help people improve their health. (DR8, M, salaried GP)
Emotional strain
As a consequence of struggling with complexity and uncertainty, practitioners felt that treating patients with multiple and possibly competing health conditions threatened their resolve and resilience, leading to negativity that might spill over into the consultation: Not worn down, that’s not the right word, but they are difficult to manage because they don’t seem to get any better and then obviously that has a psychological impact probably on the doctor and on the patient. (DR9, F, GP partner)
In describing the psychological impact incurred, practitioners also highlighted that consultations with patients with multimorbidity affected their motivation and reduced their capacity to cope with uncertainty and complexity. One GP who regularly saw a patient with diabetes, depression, arthritis and fibromyalgia confessed that his ability to help complex patients with multiple conditions was sometimes seriously impaired by low motivation and an absence of a management plan: One is my own feelings because when that kind of person comes in my heart sinks a little because I’m thinking what do I do now? I’m thinking what am I going to do this time? Will I be able to cope? (DR1, M, GP partner, 30 years qualified)
Patient experiences of multimorbidity
When discussing patient experiences of multimorbidity, a number of themes emerged from the data. Impact on physical ability and emotional strain were key themes. In addition, the challenges of living with multimorbidity in terms of understanding interactions and relationships between conditions, complexity of treatment regimens and treatment burden were identified by many of the patients.
Multimorbidity was not a constant phenomenon across all patient narratives and only came into view for those patients where burden was heightened over and above that experienced in day-to-day life: … so I guess I kind of manage it day by day and sometimes you don’t realise how bad it is until you think, ‘Hang on a minute, I can’t do this, this and this’. (P3, F, 57 years, OA and CHD)
Many patients described the burden caused by the physical impact of their conditions, affecting their day-to-day and social lives: We don’t go out now, basically. I’ve been a Freemason for many years. Every Lodge Meeting has a dinner after. There are times when I can’t stay for dinner. I’m so tired I have to go. That is a bit embarrassing (P11, M, 76 years, OA and CHD)
Burden associated with multimorbidity often led to reductions in mobility, loss of independence and feeling slowed down by their conditions: Because there’s loads of things that I could do and can’t do now and I can’t do it without anybody with me, I can’t do anything if I’m on my own. (P1, F, 68 years, OA, CHD and Dep)
The progressive nature of multiple conditions could also lead to additional burden on patients: … but because I’ve got all these things going round, what’s happening is I’m just going down and down in a vicious circle getting physically … I can see it, getting physically more feeble. (P17, F, 63 years, DM and Dep)
Physical limitations caused by their health conditions also had mental or emotional implications for patients, especially following a new diagnosis (e.g. diabetes) after coming to terms with living with other long-term conditions (e.g. arthritis): So I think it wasn’t until about, probably about four or five months later that it started to hit me, the implications of that, and I found that very hard to deal with and I tried not to think about it. (P12, F, 57 years, DM and OA)
To what extent the impact of multimorbidity registered with patients was in part related to the social and psychological consequences of multimorbidity. For example, an inability to conceal poor health in social environments often led to feelings of embarrassment and frustration, affecting patients’ personal identity. Many patients also described the impact their health had on their mood, displaying signs of low mood and depression: My wife had to do everything. She does everything, I can’t do it. It’s embarrassing. I can’t lift anything. If we go anywhere and we’ve got a suitcase, my wife has to carry it. Well wheel it about and lift it. I can’t do it. I just can’t do it. It’s embarrassing. I don’t know I just get fed up sometimes. It’s very depressing, very depressing. (P11, M, 76 years, OA and CHD)
The presence of multimorbidity also registered with patients when the treatment and care were particularly burdensome, for example, when they received repeated appointments with different health services, You know, oh I can’t go shopping today, I can’t do this today because I’ve got to go to the nurse and you know it takes over your life really. (P1, F, 68 years, OA, CHD and Dep)
or when they were prescribed complicated medication regimens, Codeine can make me constipated and then I take stuff for constipation and that can give me tummy ache. And then you think, ‘Oh this is just horrible!’ But you know that you have…you know, you can’t just stop it altogether so you have to then take something to then counterbalance something else. (P3, F, 57 years, OA and CHD)
and also when they felt overwhelmed by the self-management advice given, I was getting myself all you know, anxious coming in, you know, I mean I didn’t fall out with my doctor but I told him I couldn’t do this physio thing because of the arthritis. (P10, M, 68 years, OA, CHD and Dep)
However, some patients reported very little impact from having multiple as opposed to single conditions, and not all patients felt that having multiple conditions led to additional burden associated with managing their health. These patients often described how they followed the advice they were given and took the medications they were told to take, requiring little further support from their primary care providers: Well I actually don’t find it a huge problem. I’m one of these people that thinks whatever you get in life you just get on and deal with it. And it doesn’t restrict me in any way really. (P8, M, 67 years, DM and CHD)
Most of these patients appeared to take a pragmatic view of life: I tend not to think about it, you know. It’s just one of these things. I’ve always been the same, I just get on with life. You’ve just got to deal with it. (P4, M, 58 years, CHD and Dep)
Of the 20 patients, 6 fell into this broad category (P2, P4, P8, P10, P15 and P18). There was no obvious pattern in terms of combinations or numbers of conditions (3 had 3 conditions and 3 had 2 conditions), presence of depression (4 had depression 2 did not) or levels of deprivation (3 were living in a deprived area and 3 were not; see Table 1) which characterised these patients.
The role and concepts of self-management
As well as exploring what multimorbidity meant to practitioners and patients, we also looked at how attitudes to self-management related to these concepts of multimorbidity. Here, we were interested to learn whether experiences of multimorbidity among practitioners and patients impacted on attitudes to and experiences of self-management. When discussing the concept of multimorbidity, the issue of self-management was seen as a key factor for all of the practitioners who were interviewed.
For healthcare practitioners, self-management was viewed as comprising many different health behaviours summarised into three themes: appropriate help-seeking, compliance with medication and healthy lifestyle choices. Practitioners described good self-managers as patients who presented to healthcare services at appropriate times and knew when to seek help, for example, at the time of an exacerbation. Patients were often perceived to be poor at differentiating when to and when not to seek help, leading to either an over-reliance on medical care, or presenting too late to receive appropriate treatment and prevent complications. Practitioners’ interests in promoting self-management in multimorbidity stemmed primarily from a need to reduce service use: Sometimes they’ll not always need to come, like, if they’ve got a cold and need to maybe up their inhalers slightly until they get over a cold, its not always necessary but identifying at what point is suitable to come in and hopefully, you know, lessen their appointments that they need by looking after themselves. (PN2, F, practice nurse)
In contrast, patients’ motivations to self-manage were not premised on a desire to reduce their use of healthcare. Indeed, many patients viewed seeing their GP or nurse as a ‘last resort’ and did not believe that they visited their GP as often as they would have perhaps preferred to. Often, their reluctance to visit their practice owed to their desire to see the same doctor as they valued the continuity of care: … but I thought it’s a waste of time making appointments, you’re just wasting time somebody else could use. So unless it’s something absolutely life threatening [I don’t make an appointment]. (P16, F, 58 years, Asthma and DM) … if you want to see a particular GP, sometimes, an appointment can be a month ahead and if you’re worried about your palpitations in the middle of the night, that’s not much of a help really, you know, so that’s quite difficult. (P5, F, 58 years, DM and CHD)
Many patients commented that they actually felt they had had little contact with healthcare services: … unless something flares up like it did last week on Tuesday, I don’t like going when I don’t need to go. (P4, M, 58 years, CHD and Dep)
Instead, patients tended to be motivated to self-manage to help reduce the impact of their conditions on their daily routine and lifestyle. When describing how they looked after themselves, patients often described instrumental activities aimed at improving their lives and their independence: And I’ve built in a downstairs toilet which has made my life so much easier, and … but self-care, yes, I’ve got showers. […] So I don’t actually need any assistance as such I’ve got rails up the stairs. So anything that I can do to make my life easier I’ve already put into place. (P3, F, 57 years, OA and CHD)
Discussion
Summary of main findings
Patient and practitioner concepts and understanding were driven by the impact of multimorbidity. Practitioners characterised multimorbidity in terms of complexity and uncertainty, which sometimes caused them emotional distress. The difficulties experienced by healthcare practitioners were universally recognised across the sample, with no difference by area (levels of deprivation), gender, years of experience or by role (GP/nurse). Patient experience was more varied depending on burden, disablement and emotional impact. Perceptions of increased treatment burden and increased disability led to patients reporting greater emotional distress. A key finding was that some patients did not perceive multimorbidity as problematic. The reasons for this are unclear, but this group should be recognised as a distinct subgroup, worthy of further research, rather than as deviant cases.
Self-management was seen by practitioners to be a key element of managing multiple conditions. However, there were differences in the practitioner and patient drivers for self-management and in their definitions of success. For practitioners, the aim of patient self-management was to reduce patients’ needs for healthcare appointments and use of unscheduled care. In contrast, patients felt that the value of self-management lay in enhancing their lifestyle and improving functioning and quality of life, and this has implications for measuring benefit of interventions designed to manage multimorbidity.
Strengths and limitations
A key strength of this research was the inclusion of both patients and practitioners to explore their views about the meaning of multimorbidity, its implications for key stakeholders and the role and purpose of self-management in multimorbidity, as previous qualitative studies have tended to focus only on one of these groups.10,16 Selecting the interview sample from patients who completed the survey phase of the study allowed us to purposively sample patients based on a range of demographic and medical variables, ensuring a diverse sample. There was a relatively low response from patients from ethnic minorities to the survey (1.6%; n = 7), and previous research has shown high rates of multimorbidity in minority populations, which are currently underserved by the health system. 17 Therefore, further research is needed to explore potential differences in the conceptualisation of multimorbidity and self-management within different minority groups. The majority of practitioners were also purposively sampled, but snowball techniques were also necessary because this study was not able to financially compensate practitioners for their time, which in some practices led to poor uptake. Sampling was limited by practitioner agreement and availability for interview.
Comparison with other studies
Increased burden and emotional strain were experienced by practitioners particularly when faced with patients who showed continued lack of improvement. This may suggest that these attitudes do not relate to multimorbidity per se, but to working with complex patients who fail to improve. GPs talked about how they had to overcome their own negative attitudes in relation to these patients who they described as ‘heart-sink patients’. As in the research of O’Brien et al., 7 in which practitioners described working with patients with multimorbidity as ‘exhausting’, ‘demoralising’, ‘overwhelming’ and ‘soul destroying’, practitioners in this study used similar emotive words when talking about patients with multimorbid long-term conditions. O’Brien et al. 7 concluded that the negative responses practitioners felt in response to multimorbidity were at least in part due to the pressures of working with socially deprived populations. However, we found that practitioners from practices from a range of affluent and deprived populations held equally negative views about multimorbidity, suggesting that negative attitudes in this context are more a response to dealing with complex patients than working with patients from poor socio-economic backgrounds.
Patients often only recognised multimorbidity when their coping mechanisms were exhausted and their illnesses became burdensome, or when their identity was threatened. This ties in with the work of Charmaz, 18 who described how long-term conditions that cause impairment intrude on a person’s daily life and undermine their perceptions of self, resulting in an enforced change in identity. However, not all patients experienced multimorbidity in this way. It is not clear why some patients were less troubled than others, but it may be that they were less ill, or that they were much more adept at undertaking key tasks assigned to sick roles, such as adhering to the advice of health professionals and taking medicines as prescribed. They may also have been more resilient than other patients, leading to a more pragmatic and flexible attitude about managing health. As in the research of Morris et al., 19 which reported that burden was not inevitably increased in all patients with multimorbidity, perceived levels of burden were subject to fluctuation and change over time. As the interviews in this study were completed at only one time point, it may be that patients’ views of whether multimorbidity increased burden may also change depending on how ‘well’ they felt at the time of interview. The differentiated response among patients to multimorbidity may also owe to the fact that some were more resilient than others. Resilience in the face of chronic physical illness is known to be a psychological trait associated with better mental health and enhanced capacity to cope with and self-manage illness, 20 but the extent to which this applies to multimorbidity is unknown and warrants further research.
Implications for research and practice
Self-management is seen as an important part of managing long-term conditions particularly in multimorbidity. As perhaps may be anticipated, problems about how to support self-management are magnified in people with multimorbidity. Self-management was recognised as important by both practitioners and patients. However, practitioners in this study felt that patients struggled to self-manage. This perception may have been reinforced by the burden and emotional strain practitioners faced when dealing with patients who failed to achieve good self-management. Alternatively, the burden and strain experienced by practitioners may owe to their own struggles to motivate patients to self-manage in the absence of guidance and support to help them achieve this aim. Barriers to self-management may therefore be present where practitioners and patients hold different motivations to promote and engage with self-management and define successful self-management differently. Practitioners typically signed up to service-led incentives to promote self-management which centre on initiatives to reduce demand for services, whereas patients were more motivated to self-manage for personal reward.
The use of existing condition-specific guidelines in the presence of multimorbidity is only likely to exacerbate complexity and uncertainty, rather than help solve problems. 12 Improved integration of clinical guidelines, which currently follow single-condition models,9,21 may help reduce the clinical uncertainty that practitioners face when dealing with patients with multiple conditions. However, before reconfiguring services of NHS, as suggested by many experts in the field,1,8,9 we need to take into consideration what multimorbidity means to different stakeholders. It has been recognised and our study would support that care for multimorbid patients should in part be driven by individual patient preferences and priorities, including a recognition of when to stop giving care. 22 Additionally, better healthcare for patients with multimorbidity may need to balance patient priorities with a need to allow clinicians freedom and confidence to make judgments in the face of complexity and uncertainty. 23
Research shows evidence of high levels of primary and emergency unscheduled care use in this population,4,24 but there has been little exploration of whether these patients feel that they do overuse services or what they would hope to achieve in successfully self-managing their conditions. One key difference in practitioner and patient views of self-management was that patients felt that they did not access healthcare unnecessarily and that their aim would not be to reduce the contact they have. The aim of the current NHS strategy for treating patients with long-term conditions is to improve self-management and therefore reduce patients’ need for healthcare appointments and unscheduled care. However, if patients do not think that they are using healthcare, excessively improving self-management may not result in reduced service use, which may in part explain the largely negative results of self-management interventions in people with long-term conditions. 25
Conclusion
There have been recent calls to improve existing guidelines to facilitate more effective management of multimorbidity. Indeed, in the English NHS, the National Institute for Health and Care Excellence is currently deciding on the scope of a multimorbidity guideline. However, this study suggests that guideline development of this kind should take into account the gap in perceptions among practitioner and patients about experiences of multimorbidity. Not least, guidelines would need to acknowledge the tension between practitioners’ and patients’ accounts about self-management in the presence of multimorbidity. Interventions that can enhance both practitioners’ and patients’ experience of living with multimorbidity and facilitate self-management are few, and there is scope to develop cost-effective interventions that can improve health outcomes among growing numbers of people with multimorbidity.
Footnotes
Appendix 1
Appendix 2
Acknowledgements
We would like to thank NIHR Primary Care Research Network – Northwest for its support in recruiting GP practices and in providing support with patient identification through quality and outcomes framework (QOF) registers. We would also like to acknowledge the practitioners and patients who took part in the interviews and also the support staff at the participating sites.
Declaration of conflicting interests
This article presents independent research commissioned by the National Institute for Health Research (NIHR). The views expressed in this publication are those of the authors and not necessarily those of the National Health Service (NHS), the NIHR, or the Department of Health. The funders had no role in the design and conduct of the study; the collection, management, analysis and interpretation of the data; and the preparation, review or approval of the article. None of the authors have conflicts of interests to declare.
Funding
This research was funded by the National Institute for Health Research (NIHR) School for Primary Care Research and a Research Capability Funding grant from the NIHR Collaboration for Leadership in Applied Health Research and Care for Greater Manchester.