
Abstract
Objective:
Patients with comorbid chronic conditions may prioritize some conditions over others; however, our understanding of factors influencing those prioritizations is limited. In this study, we sought to identify and elaborate a range of factors that influence how and why patients with comorbid chronic conditions prioritize their conditions.
Methods:
We conducted semi-structured, one-on-one interviews with 33 patients with comorbidities recruited from a single Veterans Health Administration Medical Center.
Findings:
The diverse factors influencing condition prioritization reflected three overarching themes: (1) the perceived role of a condition in the body, (2) self-management tasks, and (3) pain. In addition to these themes, participants described the rankings that they believed their healthcare providers would assign to their conditions as an influencing factor, although few reported having shared their priorities or explicitly talking with providers about the importance of their conditions.
Conclusion:
Studies that advance understanding of how and why patients prioritize their various conditions are essential to providing care that is patient-centered, reflecting what matters most to the individual while improving their health. This analysis informs guideline development efforts for the care of patients with comorbid chronic conditions as well as the creation of tools to promote patient–provider communication regarding the importance placed on different conditions.
Introduction
It is estimated that 24% of all Americans and 65% of adults aged 65 years or older have two or more chronic conditions. 1 A similar rate exists among older Veterans receiving care through the Veterans Health Administration (VHA). 2 The 2015 US Census reported more than 21.3 million Veterans, 3 and in 2015 there were an estimated 9.3 million US Veterans over the age of 65 years. 4 Older Veterans are more vulnerable to chronic health conditions; 5 it is reported that over a third of older Veterans have at least three chronic conditions. 6 Analyses have shown that Veterans are o diagnosed with more health conditions than the general population, 7 including high rates of hypertension, diabetes, osteoarthritis, chronic pain, and lung disease. 8 Compared to the onset of a single disease, the experience of comorbid chronic conditions (sometimes also referred to as multiple chronic conditions; per the literature, 9 we choose to use the term comorbidities) can cause considerable distress. 2 Many individuals with comorbidities struggle to address symptoms, maintain a sense of identity, and cope with their situation. 10 Patients with comorbidities experience more “hassles” than patients with single illnesses, 11 such as poor coordination of care. 12 Patients may feel tension across the tasks associated with each of their conditions or perceive tradeoffs among them. 13 Clinicians have described discordant conditions—those for which management differs from or competes with management of a comorbid chronic condition—as a critical aspect of medical complexity and by extension, complex patients. 14 In this context, understanding the importance that patients place on their different conditions becomes a salient issue. 15
As a concept, “prioritizing” refers to the act of organizing or approaching things in some order of importance. Previous studies have found that patients with comorbid chronic conditions sometimes prioritize the management of one condition over others that they have.16,17 As these authors explain, when faced with the complexities of managing comorbid conditions, such prioritizations may be a means for patients to gain a sense of control, focus their management efforts, and conserve limited resources. Although some studies have explored why patients prioritize their various conditions in the ways that they do,17–20 this work had not yielded a thorough accounting of the factors that influence those prioritizations. The ability to contextualize an individual patient’s situation 21 and understand how and why they prioritize their various conditions is critical for healthcare providers who seek to offer patient-centered care.
Patient-centered care has been defined as “the experience (to the extent the informed individual patient desires it) of transparency, individualization, recognition, respect, dignity, and choice in all matters, without exception, related to one’s person, circumstances, and relationships in health-care.” 22 In practice, any effort to deliver patient-centered care also requires patient-centered communication, which emphasizes understanding patients’ perspectives, needs, and values, and building a shared understanding between patients and providers regarding health problems and their treatment. 23 Patient-centered care has the potential to positively impact a variety of outcomes; 24 however, providing patient-centered care to individuals with comorbidities may also be inherently challenging. Chronic disease management is not a uniform, one-size-fits-all process, and what matters most to the patient across their conditions may change and align with or diverge from what matters most to their providers. Therapeutic efforts and self-management interventions that neglect to account for the relative priorities a patient places on their conditions can have the unintended consequence of diminishing quality of life, failing to improve health status, or introducing other problems. 25
In an effort to inform the delivery of patient-centered care for patients with complex health needs, we set out to understand more fully how and why Veterans with comorbid chronic conditions prioritize their conditions. Our specific objective was to identify and elaborate a range of factors that influence Veterans’ prioritizations of comorbid chronic conditions.
Methods
Study design
As part of a larger, one-year study focused on health information seeking and comorbidities, we conducted semi-structured, one-on-one interviews with Veteran patients receiving care through VHA. Founded on the principles of naturalistic inquiry, a qualitative methodology that emphasizes understanding social action from the viewpoint of social actors,26,27 the overall goal of the study was to describe the ways in which Veterans with comorbid chronic conditions seek and use personal health information and to examine the relationships that exist between those activities and self-management. The analysis presented here was an exploratory objective within this larger study. In describing our methods below, we address the major domains identified in the consolidated criteria for reporting qualitative research (COREQ) framework. 28
Study setting
This study was conducted at a single VHA Medical Center located in a large metropolitan area in the Midwestern United States. The facility provides a wide range of services, including primary, specialty, and extended care, and is also a tertiary care referral center for the surrounding region.
Study participants
Recruitment of participants was based on purposeful selection. 29 Our goal was to assemble a sample of patients who would meaningfully articulate their experiences managing comorbid chronic conditions. In addition, to support comparative analyses for the larger study objectives, we wanted to ensure that all study participants had at least one health condition in common. Based on the input from our study clinical advisors, its widespread prevalence in the Veteran population, and its association with other chronic health problems, 30 we selected diabetes as this common condition. Sampling inclusion criteria thus required that participants (1) be at least 18 years of age or older, (2) have a diabetes diagnosis, and (3) have at least two other diagnosed chronic conditions. For the well-being of participants and research staff, and given the potential for active terminal illnesses, significant cognitive deficits (e.g. dementia), and uncontrolled psychiatric illnesses (e.g. schizophrenia) to dominate perceptions and to shape the interview narratives in ways that would not be analogous to other participants, patients with such diagnoses were excluded from participation.
To facilitate recruitment, we worked closely with our study clinical advisors and affiliated nursing staff who provided a list of patients that they believed might participate based on the aforementioned inclusion/exclusion criteria. Upon receiving this list, a member of our research team (J.N.H.) conducted brief chart reviews to confirm that each individual met the study criteria. In addition to working with our clinical advisors, we also identified potential participants by taking a random sample of 300 patients using facility administrative data to create a list of patients who met the study criteria and then confirming their eligibility through subsequent chart review. We identified a total of 202 patients; 154 from clinical referral and 48 through the database search. We then excluded 53 patients who did not meet the inclusion criteria, 65 who did not respond to the invitations, and 29 who were not interested in participating in the study. Because we reached saturation in our interviews, the point at which little-to-no new information was being uncovered, we chose not to contact the remaining 22 patients. The final sample (N = 33) included 14 participants (42.4%) identified through referrals from our clinical advisors and 19 participants (57.6%) identified through facility administrative data. Patients who met the study criteria were sent a letter inviting them to participate which also included a declination postcard. Those who were not interested were given a 2-week period to opt out of participation by returning the postcard. Given the potential for discrepancies between self-report of chronic conditions and documentation in the medical record, 31 we conducted a final screening of all potential participants via telephone to confirm that they believed they met the study inclusion criteria, to confirm their interest in participating, and to schedule the interview session.
Data collection
To avoid the kind of systematic bias that can emerge from relying on a single interviewer, semi-structured interviews were conducted over a 3-month period by two study team members (J.N.H. and E.B.), who had substantial prior experience collecting qualitative data in complex patient populations. Patients were provided with an informational sheet explaining the purpose of the study and the voluntary nature of participation. Recognizing that having participant names on printed consent forms posed a potential risk to anonymity and privacy, each participant instead provided verbal consent prior to the start of their interview per the approved institutional review board protocol. During the sessions, participants completed a background questionnaire and a chronic condition inventory—a document containing a list of common conditions and space for participants to write-in other conditions that they were experiencing that were not represented on the list. The inventory prompted participants to indicate which conditions they had, and to rank order which conditions were of highest priority to them. These instruments were critical to contextualize the participants and describe the overall sample, and to clearly document the different comorbid conditions of participants. The semi-structured interview began after the background questionnaire and condition inventory were completed, and typically lasted about 60 min. This sequence of data collection activities was critical, as questionnaire and inventory responses supported targeted questioning during the interviews. Each participant was interviewed only once.
The open-ended, probe and follow-up questions that comprised the semi-structured interview guides were informed by the existing literature 10 and other data collection instruments previously used by the study investigators. Relevant topic areas covered during the interviews included (1) perceptions of overall health, (2) condition prioritization, (3) reasons for and factors influencing prioritization, and (4) concluding thoughts. The data collection instruments were tested in a series of four practice interviews conducted with volunteers who worked at the medical facility. Feedback and insights gleaned from these practice sessions were used to revise the instruments which were subsequently tested in an additional two practice interview sessions prior to the start of data collection.
Data processing and analysis
Questionnaire and inventory responses were logged in a spreadsheet to support descriptive statistical analysis. All the interview sessions were audio-recorded and transcribed verbatim by a study research assistant. Analysis of the interview data was conducted using constant comparative techniques 32 which involve deriving concepts from data and comparing them in order to support meaningful categorization. Two study team members (L.M.R. and J.N.H.), each with academic training and previous experience conducting qualitative analyses, served as primary coders for this analysis, and the study principal investigator (T.P.H.) served as a conceptual consultant. We initiated coding by creating a list of simple categories from the interview questions and then began to identify emergent subcodes within each of these categories and to document them in a codebook. To enhance rigor, the two primary coders began by independently reviewing five transcripts and then meeting to compare and contrast the subcodes that they identified. We drew upon MacQueen et al.’s 33 practical guidance for team-based codebook development. We assigned the responsibility for creating, updating, and revising the codebook to one team member (J.N.H.) and held regular meetings with two other team members (L.M.R. and T.P.H.) participating in the analysis to review codes and definitions, stating specifically what each code should and should not capture. In this way, our codebook development was both collaborative and iterative.
Using the initial codebook, the primary coders then began the process of coding all transcripts independently. The two primary coders met weekly to discuss the transcripts, compare interpretations of specific text segments, reach consensus around coding discrepancies, expand and refine codes, and update the codebook as warranted. The initial codebook naturally expanded during this process but became saturated after coding about 12–14 transcripts. Transcripts were recoded as necessary as the codebook evolved. The principal investigator also provided a final review of all coded transcripts to ensure that the team appropriately refined and consistently applied all codes. 32
Results
Description of sample
Table 1 presents the demographic characteristics of participants. The sample was comprised mostly of males (94%), 67% were ages 61–70 years, 82% were White, and 97% were of non-Hispanic origin. The majority of participants (88%) described their overall health status as fair or good; less than 10% considered themselves to be in excellent or very good health. The average number of conditions reported by participants was six (range, 3–11), with three being the minimum number of conditions per our recruitment criteria. This finding aligns with previous studies showing that on average, Veterans are diagnosed with 5.8 health conditions. 8 As shown in Table 2, the top three most commonly reported conditions were diabetes (100%), hypertension (88%), and chronic pain (52%). Diabetes was ranked as the highest priority condition by 58% of participants and among their top three priority conditions by 97% of participants. It is important to note that although having a diagnosis of diabetes was one of our sampling inclusion criteria, we did not tell participants that they were being invited to participate because of their diabetes, but rather because we wanted to discuss their various conditions. Hypertension was not ranked as a top priority condition by any participants, but was ranked among their top three conditions by 52% of participants. Chronic pain was ranked as the top priority condition by 9% of participants and was ranked among their top three priority conditions by 15% of participants. Other conditions often included in the top three priority conditions were heart disease (18%), kidney disease (15%), osteoarthritis (12%), and cancer (12%). Table 2 presents a list of conditions reported by participants and their priority rankings.
Demographic characteristics.

GED: General Educational Development.
Condition rankings.

Conditions not ranked in the top three were removed from this table.
Percentages based on number of participants in the sample who have the condition (not the total sample size).
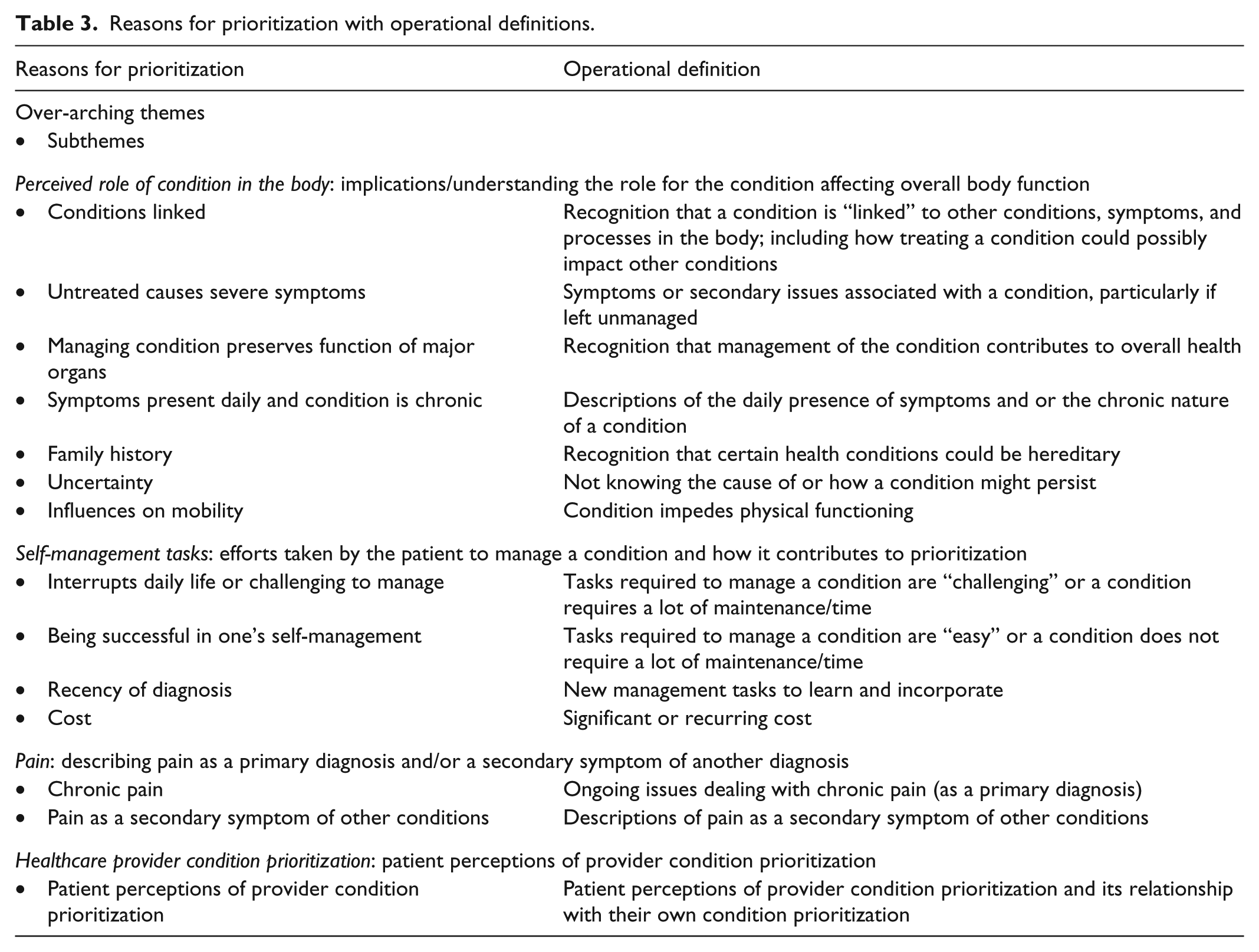
The aforementioned background questions were intended to gather information to guide the interview through various interrelated topics and to support our understanding of each participant’s context and its relationship with condition prioritization. For example, 58% of patients rated their health as fair or poor, and a third of these patients also described experiencing either chronic pain or pain associated with another health condition, and rated these conditions as their top priority due to the presence of pain. The interviews were used to explore such issues to further explicate the concept of prioritization and the factors influencing condition prioritization. Table 3 presents the list of factors that participants articulated for prioritizing their conditions and operational definitions of our codes. As we explain below, the diverse factors influencing condition prioritization that we identified largely reflected three overarching themes that emerged from our analysis: perceived role of condition in the body, self-management tasks, and pain. Interestingly, some participants also mentioned how they thought their healthcare providers would rank their conditions as an influencing factor in their own prioritizations. We present this point at the end of our findings section.
Reasons for prioritization with operational definitions.
Perceived role of condition in the body
Patients commonly have their own unique perceptions or explanatory models regarding their health and their health conditions. 34 Among the participants in this sample, the most commonly reported factors influencing condition prioritization were related to the perceived role that different conditions play within one’s body and their perceived effect on overall body function. We describe the factors that were reflective of this theme below.
Many participants mentioned family history as a factor influencing their prioritization and expressed anticipation that the same conditions that affected their parents would also impact their own body function. When discussing his reason for prioritizing anemia, a 69-year-old male participant said, “Mainly because my mother was anemic all her life and I feel that’s just something that’s going to come along” (Participant 3). Different from expecting a condition to develop is the uncertainty regarding why certain conditions develop in one’s body. Some participants discussed the experience of not knowing the root cause(s) of a condition or how it might persist as other factors influencing their condition prioritization.
For other participants, the notion of conditions being linked to one another within the body was significant, and they described how they felt that one condition could influence another condition. For example, with regard to rating diabetes as his number one priority, one participant with eight conditions said, “Well, because it complicates any of the other issues” (Participant 32). Participants also discussed how treating one condition could possibly alleviate the complications of other conditions. In the words of another participant with eight conditions who ranked diabetes as his number two priority, “Well, the diabetes is the key to all my health problems … You treat the major disease and you treat the rest of it by treating the diabetes.” And, “The principle of one thing takes care of the other. You have to watch what your diabetes does and what effect it’s having on your body” (Participant 24).
The presence of condition symptoms—particularly those affecting body functions that are instrumental to daily life—was another important factor for many participants. Participants discussed the influence of symptoms on their mobility, including concerns about how a condition caused physical disabilities and impacted their ability to walk, work, and keep medical appointments, limiting activities, and leaving them dependent on others. A 64-year-old participant who is currently employed at a large retail store described the neuropathy he experiences as a result of his diabetes, saying
I know how it affects me as to my mobility. It could even affect my ability to work if it gets too bad … I can no longer do certain things I was able to do before … I can’t do heavy lifting and twisting stuff. (Participant 2)
Related to the experience of symptoms, for other participants, the anticipation that a condition could have severe repercussions if left unmanaged was an important determinant of their prioritization. These participants discussed how different conditions could, for example, lead to severe adverse outcomes. In the words of one participant with five conditions, “I put heart disease first because if that goes it doesn’t make any difference. You’re not going to be around to worry about the others” (Participant 19). Other participants discussed prioritizing a condition because managing that condition preserves aspects of body function. Some participants described their knowledge of how certain conditions could affect their organs, for example, leading to crises. Regarding the prioritization of kidney disease, a 64-year-old participant with five conditions said, “It’s because what I’ve learned what the kidneys do for your body, even how they’re related to your anemia, that the kidneys produce red blood cells” (Participant 2). (Note: The kidneys produce erythropoietin which stimulates blood production from the bone marrow; the kidneys do not make red blood cells). Another participant with four conditions described how diabetes, his top ranked condition, affects multiple organs saying, “Because of the aggressive nature of the disease and what it affects; heart, eyes, kidneys, it goes on and on” (Participant 26).
Self-management tasks
Self-management—the work associated with handling symptoms, treatments, and the implications of a condition for daily life 35 —was also commonly discussed by participants as a factor influencing their condition prioritization. Having an understanding that a condition was chronic and would require such work for the rest of their lives weighed heavily on many in the sample. Participants discussed a condition as a priority in this context when the condition was demanding, interrupted daily life or treatment, or when medical monitoring was required. For example, with regard to prioritizing diabetes, a 62-year-old participant said, “I take care of my blood sugar every day so that would be the number one” (Participant 29), and a 63-year-old with six conditions who ranked diabetes as his number one priority commented, “It’s all consuming. It’s every meal you eat. Everything you pick up to eat. Then you got the pills to take, all the different pills to take each day, and checking your blood sugars. It’s quite consuming” (Participant 11). Other participants made the point more simply; a participant with five conditions who ranked his diabetes as his top priority said, “Well, the diabetes is the harder one for me to control” (Participant 21).
The concept of “control” in self-management emerged in another way as well. Being successful in one’s self-management efforts was also discussed as a factor influencing condition prioritization. In some cases, success was also associated with a condition being easier to manage or less burdensome than others. Still, however, the act of dedicating effort to the management of a condition and seeing positive results from that effort had a strong influence on one condition’s prioritization over another. A 64-year-old male with four conditions explained his ranking high blood pressure as a priority, “I bought a little checker, one of those things you stick around your wrist, and I take the medicine … all I have to do is remember to take the medicine and it’s fine” (Participant 27).
Other factors influencing condition prioritization emerged as part of our overarching self-management theme but were not noted as frequently. These included costs associated with condition self-management (e.g. a 68-year-old participant with eight conditions said, “That has caused me $1,000 with glasses” (Participant 24)) and the relative recency of a diagnosis and the corresponding implications for incorporating new self-management tasks into daily routines (e.g. a participant with four conditions who ranked cancer as his second priority and diabetes as his first priority said, “I would say when I was diagnosed with cancer, at that point, that took my primary focus because that was an immediate short term life adjustment” (Participant 26)).
Pain
Pain was another broad theme that recurred frequently when participants explained the prioritization of their conditions. Pain emerged as distinct from participants’ descriptions of other condition symptoms and was framed primarily in two ways, participants describing chronic pain and participants describing pain associated with another condition. Some participants experiencing chronic pain rated it as their highest priority because of its consuming nature. For example, a 59-year-old participant with six conditions said, “I’m focused on pain, I’m trying to relieve the pain. Everything else is secondary” (Participant 77). Other participants described pain they were experiencing as a result of a condition other than chronic pain. Despite this difference, participants described their pain in similar ways—as an experience that shapes the quality of their life. For example, a 69-year-old male participant with eight conditions who ranked pain as his top priority described phantom limb pain by saying
I rated them [my conditions] in order in which they affect my daily life. The phantom limb pain is the thing that changed my life the most … it’s not that being an amputee has made me disabled, it’s the phantom limb pain that makes me disabled. (Participant 9)
Healthcare provider condition prioritization
It is worth noting that in addition to the three overarching themes above, some participants in our sample also described the perceptions that they had of their healthcare providers and the rankings that they would assign to their conditions as an influencing factor in their own prioritizations. Participants described remarks made by their primary care providers and topics that their providers brought up to them during clinic visits, thus suggesting to the participant that certain conditions should be priorities. Interestingly, however, many participants reported that they had not explicitly talked with their provider about the importance of their different conditions or shared their priorities with their providers.
Discussion
Findings from this study contribute to the growing literature regarding the health and self-management contexts of patients with comorbid chronic conditions.36–39 More specifically, this study adds the perspective of Veterans with comorbidities to the existing evidence 14–17,37,38,40 focused on understanding how and why patients prioritize various conditions and the management of those conditions.17–20 As we explain below, findings from this and related work can inform efforts to highlight patient preferences and ultimately develop approaches to care that reflect what matters most to patients. 41 For patients with comorbidities, this will require more than just a shift in how care is delivered, but rather a change in conversation and how recommendations for care are developed and realized in practice. Recent meetings convened between the Institute of Medicine (IOM) and the Department of Health and Human Services (DHHS) to develop principles and improve guidelines for the care of patients with comorbid conditions have emphasized the importance of focusing on patient-centered care. 42 Similarly, other systematic reviews have emphasized the voice of the patient in constructing practical guidelines to inform care and to promote patient-centered outcomes among those with comorbidities.36,37
Among our sample of participants, the most frequently cited factors influencing condition prioritization reflected three broad themes: the perceived role of a condition in the body or its effect on overall body function, self-management tasks, and the experience of pain. Said another way, based on our analysis, patient prioritizations seem to reflect their thoughts on how a condition works, what must be done to manage it, and how it feels to have it. Condition prioritization may depend on single factors or factors that are interrelated and interplay with each other. For example, previous studies have shown that it is not just the number of conditions that affect prioritization but also the type and severity of the conditions themselves, 19 and a patient’s belief that one condition may be more serious than another. 17 These findings, coupled with trends showing overall increases in the number of conditions that patients are diagnosed with, suggest that patients may inherently feel compelled to prioritize certain conditions over others. 20 Furthermore, patients may tend to prioritize conditions that they understand over those that they do not understand, even if the misunderstood conditions present potentially more serious problems. 18
In our study, the perceived role that conditions play within one’s body and their effect on overall body function was the most prevalent overarching theme associated with the prioritization of a particular condition. Our findings demonstrate the power of family health history to make conditions personal and perhaps more salient. Subthemes regarding the presence of symptoms and symptom severity are similar to findings in previous studies showing that the experience of complications, including serious complications or “wake-up calls,” or the physical symptoms of a condition,13,16–19,43 increases the likelihood of higher prioritization and more attentive management of that condition.17,18 Our analysis also suggests that when patients perceive the management of a condition as being protective of the body or preserving body function, prioritization of that condition over others is likely. Other studies have also found that condition prioritization is not only shaped by patient perceptions of possible outcomes such as length of life and maintaining function41,44 but also by functional limitations resulting from the condition. 41 Moreover, when patients are concerned that a particular condition could be fatal, there is greater incentive for them to prioritize it over others.40,44 We did not assess participant knowledge of their conditions in this study, but aspects of our findings regarding the perceived role of a condition in the body also suggest the potential influence of such knowledge on prioritization. This is an important consideration for future work.
Another overarching theme that emerged from our analysis encompassed self-management tasks, and how the effort required to manage a condition could influence its prioritization over others. Previous studies have found that the presence of comorbidities may require patients to actively modify multiple health behaviors simultaneously, 45 resulting in self-management tasks that are both challenging and burdensome. 46 As noted earlier, the presence of comorbidities may also introduce conflicts or incompatibilities with self-management tasks across conditions. 27 The tension that is created in such situations may leave a patient feeling overwhelmed by one condition and cause them to pay less attention to others.25,47 Our findings regarding control in self-management, including the influence that perceived success in self-management tasks can have on condition prioritization, align directly with these themes. Finally, various studies have found that the presence of pain, especially chronic pain, is a major limitation to performing self-management tasks. 48 Our analysis supports findings from these as well as other studies which highlight the role that pain, whether experienced as chronic or as a secondary symptom, plays as a factor impacting prioritization of comorbidities. 49
Findings from our analysis also indicate that patient perceptions of how their healthcare providers would rank their conditions can be an influential factor in patients’ condition prioritization, 50 although the extent to which they and their providers actually talked about their perspectives on prioritization seemed limited. As noted above, few participants reported having an explicit conversation with their providers about the importance of different conditions or expressing what was a priority for them. Lack of dialogue around these topics may inadvertently promote discordance between provider and patient prioritizations and have unintended consequences for identifying the most advantageous approach to care for a patient. 51 For example, in one study, primary care physicians prioritized pain as a primary issue only 44% of the time when reflecting on the vignette of a patient whose self-described primary issue was worsening chronic low back pain, despite the fact that the patient described how experiencing pain impacted their management of other conditions. 52 Other studies suggest that providers sometimes value life-extending treatments more so than treatments that improve patient functioning. 40 Considered through the lens of patient-centered care, these findings underscore the importance of fostering patient–provider communication about patient preferences 36 and, in turn, balancing those preferences with evidence-based care approaches. They also speak to the need to develop tools and strategies to facilitate such communication. 53
Limitations
There are four key limitations to our study. First, we conducted our work within a single VHA Medical Center with a sample of Veteran patients, and these patients may be unique in ways that make it difficult to draw broader conclusions. Furthermore, Veterans themselves represent a unique population. For example, in one recent study, Veterans were found to have poorer health and functioning than civilians and military reserve members, were more likely to report cardiovascular disease than civilians, and reported getting less exercise than active duty military members and military reserve members. 54 For these and other reasons, it is quite possible that the experiences of Veterans with comorbid chronic conditions could be different compared to those of the broader population. Still, our findings are quite consistent with similar studies conducted in the general population, suggesting that Veterans with comorbidities share at least some similarities with other patients with comorbidities. Second, the selection of diabetes as an anchor condition might have inadvertently skewed our findings as those with diabetes may share characteristics (including specific co-occurring conditions) that are not representative of other patients with comorbidities who do not have diabetes. Future studies that explore prioritization in other clusters of comorbidities will help address this issue. Related to this point, there may be important linkages between diabetes and mental health conditions;55,56 our exclusion of patients in this study who had significant cognitive deficits or uncontrolled psychiatric conditions may have biased our findings. Third, our analysis of patient prioritizations of comorbid chronic conditions was only an exploratory objective in a larger study which limited our ability to probe deeply on this topic during our interviews and prevented related follow-up interviews. A study dedicated to this topic may have offered a more complete accounting of factors impacting prioritization. Finally, our results may have been biased by the fact that during data collection, we asked participants to rank order which conditions were of highest priority to them and did not explicitly ask whether or not participants prioritized their conditions at all. Future studies exploring why individuals may not prioritize their comorbid conditions could add further critical insights to this literature.
Conclusion
Studies that advance our understanding of how and why patients with comorbidities prioritize one condition over another are critically important to providing care that is patient-centered, reflecting what matters most to patients while improving their health and outcomes. 39 Our findings indicate that when prioritizing their conditions, patients are not only thinking about how a particular condition may work in their body but also what is entailed in its management and how it makes them feel. At its core, patient-centered care is about actively incorporating such perspectives into treatment. 57 Finding ways to improve the care and quality of life of persons with comorbidities is currently a prominent focus in healthcare policy and across government agencies. 58 Our analysis contributes a unique perspective to these initiatives and to the creation of tools and other strategies intended to support patient-centered communication regarding condition prioritization between patients and their healthcare providers.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimer
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the US government.
Ethical approval
Ethical approval for this study was obtained from Edward Hines Jr. VHA Institutional Review Board (approval no./ID: 10-030).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This material is based on the work supported by a Department of Veterans Affairs, Veterans Health Administration, Office of Research and Development and Health Services Research and Development grant.
Informed consent
Verbal informed consent was obtained from all subjects before the study.