
Abstract
Sonographers experience a high cognitive load in hospital-based care. High ambient noise and frequent noise-based interruptions include knocking on the room door, questions from others in the room or through communication technology, alarms, alerts from personal devices, and carts and people passing in the hallway. In addition, other providers turning on the overhead light is distracting for exams that need to be conducted in reduced lighting conditions. This article suggests strategies to improve working conditions for sonographers conducting exams on a patient in the hospital room. Our strategies emerge from human factors methods and principles, which derive from communication principles and theory. These strategies are organized by reducing noise-based and light-based interruptions in the hospital room and hallway, primarily through changes to the built environment and communication technology settings and reducing the use of speech during cognitively challenging time periods through training. Most of the strategies are low-cost and can be implemented within the current built environment and communication technology infrastructure. We anticipate that these strategies could enhance patient outcomes, increase patient satisfaction, improve sonographers’ job satisfaction, protect provider health, and increase procedural efficiency.
Nursing research has benefited from applying human factors to improve working conditions, particularly in the inpatient setting. Ultimately, improving working conditions and reducing cognitive distractions enhance the quality of patient care. For example, the relationship of the work environment and fatigue on performance has been explored with surveys of nurses.
1
There have been many initiatives to reduce the physical demands on the spine to move patients by nursing staff, including modifying the bed height while using lifting slings.
2
Although less common, some consideration has been given to reduce the cognitive load on nurses, for example, the auditory alarm burden in four hospitals from telemetry monitoring was reduced while simultaneously reducing nurse response times to critical cardiac alarms.
3
Limited research on cognitive ergonomics for sonographers has been conducted. For sonographers, ergonomic efforts to reduce ambient noise in the emergency department for healthcare providers might provide valuable insights to these efforts in other areas.
4
Human factors is
5
that field which is involved in conducting research regarding human psychological, social, physical, and biological characteristics, maintaining the information obtained from that research, and working to apply that information with respect to the design, operation, or use of products or systems for optimizing human performance, health, safety, and/or habitability.
5
(p. 35)
In diagnostic medical sonography, the room is darkened by closing blinds, patients are positioned and instructed when to breathe, and an image is captured for later physician review. For Doppler-based procedures, it is critical to hear and interpret cardiovascular signals accurately. For all procedures, being able to focus without cognitive disruptions is important to apply clinical skill and expertise to obtain a high-quality examination, of the requested physical area. For many procedures clinical imaging requires continuous access to patients in darkened and quiet conditions for 15 to 45 minutes. In most hospitals, particularly during daytime hours, it is likely that there will be multiple attempts to knock, enter the room, and/or turn on the main room light. Interruptions may come from nurses, nurses’ aides, physicians, environmental cleaning staff, physical therapists, occupational therapists, respiratory therapists, speech and language pathologists, phlebotomists, meal delivery staff, social workers, chaplains, engineers, IT staff, or patient visitors. These attempts to enter the room and other distractions from noise and lights make work more challenging, which can reduce the efficiency and quality of patient care. In addition to impacting image quality, disruptions can increase the risk of forgetting to document notes about relevant clinical information that could affect the physician’s interpretations of the study. For example, interpreting a pelvic sonogram depends on whether a female patient is premenopausal or postmenopausal and whether the patient has had prior surgeries. For a thyroid sonogram, knowing that a patient is on a particular thyroid medication can affect whether the gland is assessed to be large or small by the interpreting physician, as this could affect the ultimate diagnosis and grading decision.
Cognitive disruption is important to reduce for cognitively complex tasks, for which interruptions create risks of forgetting to complete activities or reducing the quality of performance. Healthcare is well-known to have high work complexity, the execution of diagnostic medical sonography and vascular technology are no exception. Work complexity is a function of (a) dynamics, (b) the number of parts and interconnections between the parts, (c) uncertainty, and (d) risk. 6 For dynamics, there is time pressure to quickly capture high-quality images, which provide the interpreting physician with the images needed to assess normal and abnormal features and provide physicians with information that supports a differential diagnosis and development of a treatment plan. The timing of when to gather the images needs to be negotiated with other providers who access the patient; other providers may include physicians during rounds, nurses during assessments and medication passes, meal providers, people who stock supplies in the rooms, environmental services that clean the rooms and empty garbage cans, and other staff and visitors. For interconnections between parts, sonographers and vascular technologists interact with many other providers, including interpreting physicians, specialist physicians, primary care physicians, nurses, nurses’ aides, patients, and visitors. The quality of care provided by specialist physicians depends on the image quality and information provided by sonographers and vascular technologists and relies on information shared by patients and caregivers. For uncertainty, it is not always clear whether the clinical study results are normal or abnormal, whether sonographic features have changed over time, and the underlying context of the patient’s status is essential in reducing uncertainty by providing critical information. Finally, the risk of missed diagnoses, delays in diagnoses, and inappropriate treatments is ever-present for all patients, exceptionally high with specific cohorts, such as imaging examinations that diagnose cancer or vascular disease.
Noise levels in hospital rooms have long been identified as a health hazard for all patients. Many have documented noise levels significantly greater than the World Health Organization (WHO), the National Institute for Occupational Safety and Health (NIOSH), and the Environmental Protection Agency (EPA) recommendations. 7 There is a wide range of noise generators in hospital rooms, including speech, alarms, and hospital technology-enabled communications, such as intercoms and hands-free auditory input devices. 8 There is also growing noise generation from mobile devices 9 of healthcare providers, patients, caregivers, and children. Particularly distracting noises include knocking on the door, hallway noise, and questions from family members in the room during the exam.
Light design in hospital rooms also contributes to distraction and particularly for interrupting patient sleep. 10 Alternatives to overhead lights may reduce distractions, including blue-depleted pods with task lighting at night. 11 Contributors to light levels include overhead lights, light from the hallway, outside, computer monitors, patient monitors and devices, TVs, and nightlights. Most imaging examinations need to be conducted in reduced lighting conditions for up to 30 to 45 minutes. Sonography is heavily operator-dependent, and although ideal imaging conditions may not always be possible, proper exam setup and reduced lighting is needed to optimize the exam. Patient rooms feature many obstacles to get ultrasound equipment systems set up. Closing the blinds can be challenging; computer monitors, TVs, and other devices may appear overly bright; and people turning the lights on and off can be distracting.
In this article, the authors explore strategies to reduce avoidable noise-based and light-based distractions in the hospital, including reducing and better timing communications with patients and family members. A vignette scenario is used to clarify how noise and light distractions relate to diagnostic medical sonography and a cardiovascular examination conducted in a hospital room. It is paramount that the cognitive load from interruptions and distractions is reduced for diagnostic medical sonographers so that clinical assessments can be made on reliably accurate interpretations and measurements from images and Doppler sounds. Reducing distractions would also enhance provider health and procedural efficiency. Improving working conditions for sonographers is ultimately expected to improve patient care outcomes and patient satisfaction.
Vignette Scenario: A Liver Doppler Conducted by a Sonographer
You are a sonographer, who receives an order to complete a liver Doppler for a 46 year old female patient in a medical-surgical room.
When you get to the hallway outside the patient’s room, you hear that the patient’s IV pump is alarming. Before you enter the room, you ask where the patient’s nurse is to alert them to the need to resolve the issue and turn off the alarm so that you can do the exam. Someone directs you to the nurse, who is administering medications to another patient. They tell you that they will come as soon as they can to address the alarm.
You enter the room and the patient’s head of the bed is oriented towards the doorway. The patient is watching TV with her sister, who is their caregiver. They are watching the show in Spanish, and you realize that you might need an interpreter to explain the procedure and get consent. You introduce yourself, which startles the patient who did not know you had entered the room. The patient does not speak English and the sister speaks some English, but you request an interpreter. While you wait for the interpreter, you begin preparing to do an exam for another patient on the unit.
An interpreter arrives and lets you know that they are ready to communicate with the patient, so you stop preparing for the other exam and return to the original patient’s room. You move the Workstation on Wheels (WOW) in front of the door so that you can enter with your equipment. You consider how best to move furniture in the room and avoid tripping on cords to get to the necessary side of the patient for the exam. You set up your equipment and the space around the hospital bed. You have difficulty completely closing the exterior window blinds, limiting how dark the room is. You turn off the television. You dim the lights.
The patient’s nurse knocks on the door, enters, and turns on the overhead room light. They explain that they are there to address the IV pump alarm, as requested. The nurse ensures no occlusion in the IV pump tubing and turns off the IV pump alarm. They explain to the patient that they will return in ten minutes to do an assessment and administer medications. You inform the nurse that the exam is expected to take at least 30 minutes, and they update the patient that the medications will be administered after the liver exam is done.
The interpreter works with you to explain the procedure to the patient and answer questions from the patient and sister while ensuring that neither looks confused and is willing to consent. You ask the patient through the interpreter what the specific date was of the last surgery that was conducted two weeks ago by taking out your personal cellphone and viewing the calendar and asking if Tuesday two weeks before was the correct date to enter into the electronic chart later in the day. The sister’s phone rings and she steps away to talk with their mother, who is calling for an update on her daughter’s health.
The patient monitors are causing a glare on your screen. So you change the lighting setting on the monitors so that you can fully see an accurate image.
The patient’s phone beeps as you listen to the Doppler signal, indicating that a text message was received. The monitor is beeping. The IV pump alarm goes off again. You help the patient extend her arm, which causes the alarm to go off so that a nurse does not need to be called to address it.
A nurse’s aide knocks on the door, opens it, and asks when you will be done so that they can get vital signs on the patient. You explain that you expect to be done in 30, but possibly 45, minutes because you are going to start the exam now. Then, you position the patient and begin the exam.
You receive a notification via the Vocera communication hands-free lavalier around your neck that a patient has checked into the outpatient clinic. (There is no need for you to be informed of this.)
A physical therapist knocks on the door, enters the room without closing the door, turns on the light, and asks if the patient is ready for therapy. While the door is open, you hear an overhead page, alarms going off at the nurses’ station, conversation for a group of physicians discussing where to go for coffee in the hospital, and a metal cart with metal trays and a squeaky wheel going past. You politely explain that you need the room as dark as possible to complete your exam and that the patient has to remain still, so the physical therapist agrees to come back later.
Halfway through the exam, the patient’s brother-in-law knocks on the door and enters. He speaks English as his first language. He stands directly behind you and begins asking questions about what you are seeing and pointing to your screen. You explain that you are unable to provide any clinical information and it is quite distracting to have him standing behind you. You ask the family member to wait outside the room until the exam is completed.
The interpreting physician calls you about an image from another patient examination, through the Vocera system. You respond that you are with a patient, and that you will call back when you are able to talk without another patient overhearing private health information.
You complete the exam and are checking to ensure that all of your images and data are there, the patient is comfortable, and the room is back in order. You have completed your patient’s study. You put the furniture back, get the patient comfortably situated, put the patient’s tray table back over the bed, hand the remote to the patient to turn on TV, put the blinds back, and tell the family members waiting outside that you are done. They ask for the results and you tell them that it will be sent to the interpreting physician, who will read it and write a report for the physician.
You receive a call from your co-worker. They ask you to complete an additional patient exam, on the same floor. You hurry to open the blinds, return the patient’s tray table, and move the recliner back to its original position in the corner.
You move on to the next patient. You plan to document information for all patients after all exams have been completed. Upon arrival back to your workroom, you begin filling out your worksheet to describe the exam to the interpreting physician. You realize that on one of your exams, you mislabled the side (e.g., right instead of left) for one of your images. It is likely that this happened when you were trying to answer questions from the patient’s family member that you were not allowed to answer about the clinical interpretation of the image on the device while he was standing behind you. You take the time to correct your mislabeled image to ensure that the physician’s report refers to the correct side, which is important clinically as well as to avoid triggering alerts related to potential fraud when the side with a clinical condition switches over time (e.g., a worker’s compensation claim may be refused if a shoulder with pain is not consistently reported as on one side over time in the electronic chart).
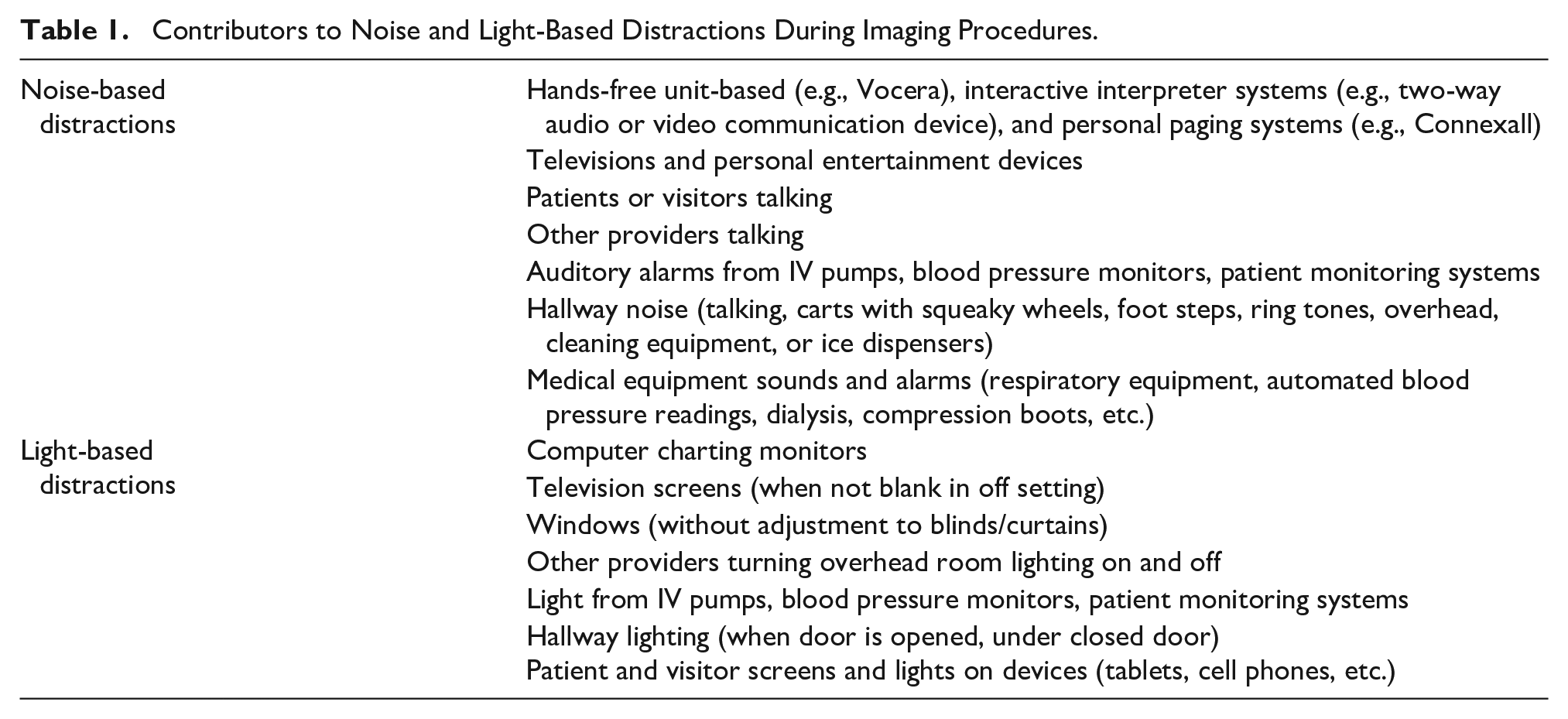
In reflecting on this scenario, avoidable distractions from noise and light contributors and interruptions include (see Table 1 for a summary of contributors to noise and light-based distractions):
A nurse entered the room to resolve an IV pump alarm, which could have been avoided by educating the patient or the sonographer on the strategy of straightening the patient’s arm to see if a kink in the tube is triggering the alarm. Alternatively, the nurse could have checked the room to ensure no IV pump, telemetry, or bed exit alarms going off right before the sonographer is requested to go to the hospital room.
The nurse changed their plans for when to administer medications to the patient after learning how long the exam would take, which could have been avoided if there was an electronic notification on the door with that information; there were unnecessary communications between the nurse, patient, interpreter, and sonographer because of the change in plans.
People knocked on the door, opening the door, and/or turned on the overhead lights to ask when the patient will be available after the exam.
People called through the Vocera system with questions that contain private health information regarding another patient and could not be discussed while the sonographer was in the room with a different patient.
The physical therapist was not aware that the patient was occupied for another 30 to 45 minutes with an imaging exam that requires quiet, darkness, and a carefully positioned patient who has to remain still, holds their breath, or talk during portions of the exam.
Sounds from personal mobile devices of the patient and visitors.
Clinical interpretation questions from a family member during the exam that could not be answered.
Exterior light from drapes that were difficult to fully close.
Glare from monitors, devices, and personal devices.
A broadly targeted notification about a patient in the outpatient setting that was not relevant to the sonographer’s duties during this work shift.
Contributors to Noise and Light-Based Distractions During Imaging Procedures.
From a human factors perspective, there are predictable types of outcomes from avoidable distractions. These include
Failures to re-engage with tasks that were interrupted during task-switching following an interruption, leading to dropped activities.
Mistakes due to distraction, including poor image quality or an incorrect measurement of image features (e.g., fundus height for gestational age).
Forgetting to correct mislabeled filenames for an image (e.g., “Right kidney longitudinal view” instead of “Left kidney longitudinal view”).
Forgetting to document information on a patient that will help the interpreting physician accurately interpret sonographic features.
Forgetting to involve interpretive services to gain truly informed consent or answer relevant questions about context.
Missing clinical patterns in Doppler signals.
Allowing a patient to breathe, move, or otherwise be poorly positioned when an image is being captured.
Having a low-quality interaction with patients and family members when need to speak loudly to be heard through the Vocera system or two-way audio or video communication device to access interpretive services, particularly for sensitive information (e.g., “you need to take your pants off so that we can do a pelvic exam”).
Having less-empathetic conversations and low-quality education for patients and family members due to burnout, fatigue, or looking at the interpreter or MARTI instead of the patient’s face to see what is being understood while communicating.
Experiencing avoidable risks to the sonographer’s health (e.g., having a patient blow air out into the face of the sonographer after holding their breath, tripping on a cord or doing an exam in an uncomfortable physical position).
In addition, there are predictable failure types in communicating with the many interdisciplinary members who coordinate to provide care with sonographers. These are 12
Communication omission: A communication is not given that is intended to be given. An example would be a nurse coming into the room to ask to be told when the room is available, but the sonographer is called away to another patient before telling the nurse.
Communication ambiguity: In addition to misunderstanding what other providers or patients are saying, there is a clinical scenario of misunderstanding the cues available with sound. Due to competing noise, there are misunderstandings. An example could be deciphering between abnormal and normal spectral readings.
Communication overload: Taking an image is a cognitively exacting procedure, particularly for complex patients with IVs who might not be able to sit independently or hold their breath. In these cases, it can be challenging to listen to clinically relevant information given quickly from a physician, such as during inpatient room ultrasound-guided procedures. In this situation, a physician is in the room who says all of the things that are needed clinically and what is expected afterwards. For example, a failure to document how much fluid was removed and how much was retained.
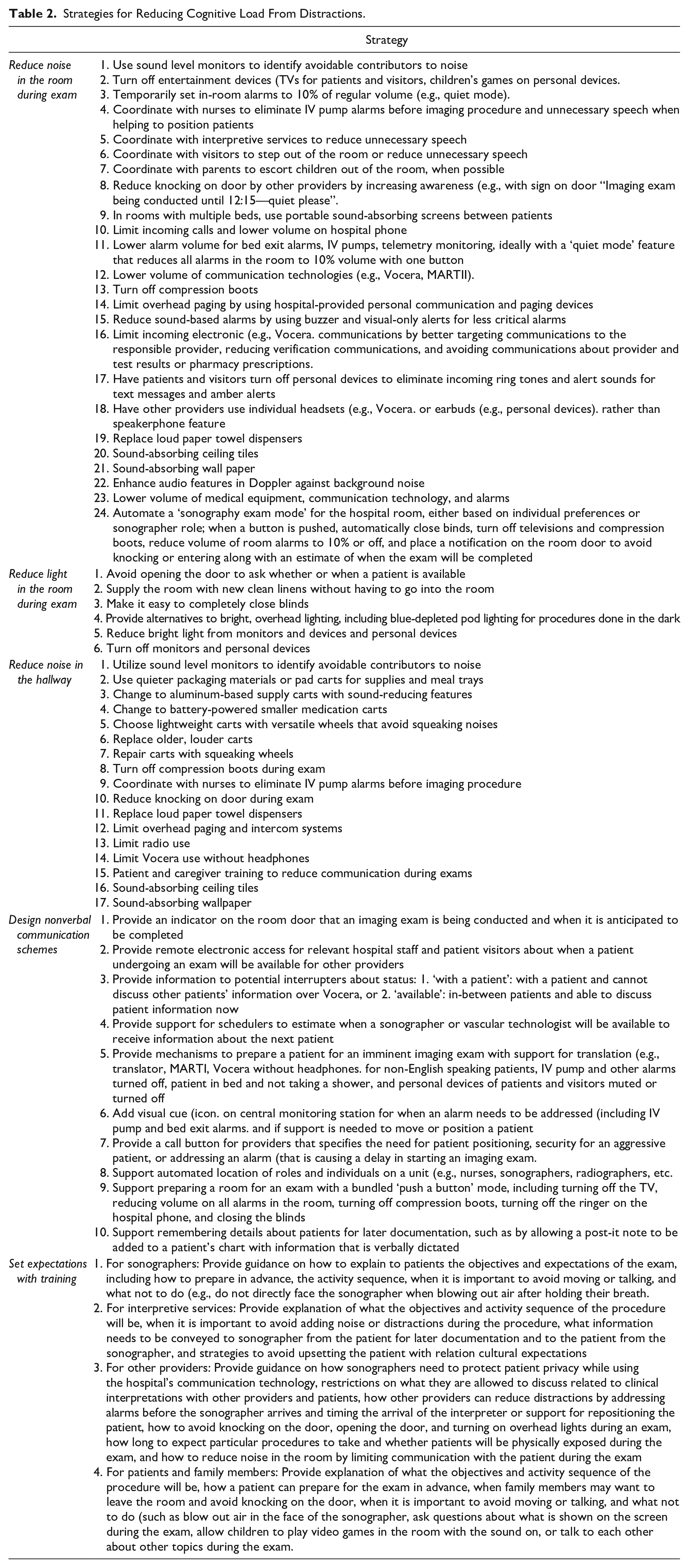
Proposed strategies are used to help reduce avoidable noise and light interference within clinical work. See Table 2 to see strategies to help reduce noise during exams, reduce light interference during exams, reduce hallway noise, and improved communication designs and training expectations.
Strategies for Reducing Cognitive Load From Distractions.
Conclusion
This article proposed strategies to reduce avoidable noise and light interference with clinical work in the hospital patient rooms. Many of the strategies can be implemented without changing the physical environment or underlying information technology infrastructure. Some strategies could be achieved through policy change or training initiatives, including reducing the use of speech during cognitively challenging periods through training. The working conditions for sonographers need to be improved for enhancing patient outcomes, increasing patient satisfaction, satisfaction with working conditions, provider health, and procedural efficiency. The contribution of cognitive ergonomics issues, such as a high cognitive load from avoidable noise-based and light-based interruptions, to poor working conditions, needs to be considered along with physical ergonomics concerns such as back pain.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.