
Abstract
Introduction:
Patient safety during surgical procedures is especially critical in resource-limited and conflict-affected regions such as the Gaza Strip. Nurses play a central role in implementing and monitoring safety protocols in operating rooms. However, their perspectives on safety practices have been understudied in this context. This study aimed to assess nurses’ views on preoperative and intraoperative patient safety measures in Gaza’s government hospitals.
Methods:
A cross-sectional descriptive study was conducted in 2023 across three major public hospitals in Gaza: Al Shifa Medical Complex, Nasser Medical Complex, and Gaza European Hospital. Using a census sampling method, 150 nurses working in the main operating rooms were recruited, resulting in a 92.6% response rate. Data were gathered using a structured, validated questionnaire based on the World Health Organization Patient Safety Assessment Tool. Demographic and professional characteristics were also recorded. Data analysis was conducted using SPSS version 26.
Results:
The sample was predominantly male (78.0%) with a mean age of 32.9 ± 7.3 years and an average of 7.23 years of surgical experience. Most nurses held a bachelor’s degree (71.4%), and 43.3% had specialized training in operating room care. High levels of reported adherence were observed in preoperative preparation (85.3%), preoperative assessment (74.7%), and operating room readiness (76.0%). Lower adherence rates were noted in documentation practices (68.7%) and identification of surgical risks (64.0%). No statistically significant differences were found between hospitals.
Conclusion:
Despite resource constraints, safety protocols are largely followed in preoperative procedures and operating room readiness. However, shortcomings remain in risk identification, monitoring, and documentation. The study highlights nurses’ key role and calls for better training, policies, infrastructure, and teamwork to improve surgical safety in conflict-affected areas.
Introduction
Patient safety during surgical procedures remains a critical global challenge, particularly in resource-limited and conflict-affected regions such as the Gaza Strip. 1 Operating rooms are inherently high-risk environments where errors can cause serious complications or death. 2 Nurses play a pivotal role in maintaining safety throughout surgical workflows 3 ; however, their perspectives, especially in conflict zones like Gaza, have been insufficiently studied.
The Gaza Strip’s public hospitals face severe challenges including political instability, frequent interruptions in essential services, and chronic shortages of equipment and supplies. 4 These systemic constraints adversely affect both elective and emergency surgical care. Previous research has highlighted limitations in the safety culture within Gaza’s healthcare system. For instance, Elsous et al. 5 found considerable variation in safety attitudes among nurses, with strong teamwork perceptions but weaker stress tolerance and hazard vigilance. Bottcher et al. 6 similarly noted positive general safety perceptions but identified critical gaps in incident reporting and formal patient safety education.
While prior studies have provided valuable insights into hospital safety culture,2,5,6 relatively few have focused specifically on operating room practices encompassing both preoperative and intraoperative phases. These stages require intricate coordination, adherence to protocols, and rapid decision-making under pressure. Research in similar contexts indicates that high stress and workload often undermine safety culture.7,8 A recent quantitative study across Palestinian hospitals, including Gaza and the West Bank, revealed that although about half of nursing staff perceived a positive safety culture, excessive stress, and overcrowding significantly hinder safe care delivery. 9 Qualitative data further emphasize communication breakdowns, resource constraints, and insufficient institutional support as major barriers. Moreover, compliance with intraoperative safety protocols, such as infection prevention measures, varies considerably and is influenced by factors including procedure type and operating theatre (OT) conditions. 10
The World Health Organization (WHO) Patient Safety Assessment Tool offers a comprehensive framework to evaluate safety practices throughout patient care stages, including preoperative assessment, intraoperative procedures, and risk identification. 11 Despite its broad use in hospital safety evaluations, application of this tool specifically to Gaza’s operating rooms from nurses’ perspectives remains limited. This study aims to fill that gap by assessing patient safety practices during preoperative and intraoperative phases in three major government hospitals in Gaza: Al Shifa Medical Complex, Nasser Medical Complex, and Gaza European Hospital. Using the WHO tool, we examine six critical domains: preoperative assessment and preparation, operating room readiness, counting and documentation accuracy, intraoperative monitoring, and identification of surgical risks.
Globally, tools such as the WHO Surgical Safety Checklist and the Joint Commission’s Universal Protocol have improved surgical outcomes by standardizing practices to prevent wrong-site, wrong-procedure, and wrong-patient surgeries.11,12 However, adherence to these protocols varies widely, particularly in emergency, conflict, and resource-limited settings where compliance ranges from 40% to 70%, often due to time pressures, insufficient training, or lack of oversight.3,13,14 In such contexts, emergency procedures frequently bypass some safety steps to expedite care, 15 a pattern relevant to Gaza’s politically unstable and resource-strained environment.
Focusing on nurses, essential members of the surgical team, this study provides crucial insights into the implementation of global safety standards under challenging conditions. Local evidence points to barriers including staff burnout, cultural factors limiting error reporting, and inconsistent protocol adherence.5,6 Our findings aim to guide targeted interventions to strengthen training, workflows, and support systems, ultimately enhancing surgical safety and patient outcomes in Gaza’s uniquely demanding healthcare landscape.
Materials and methods
Study design
This observational, descriptive, and analytical cross-sectional study aims to assess nurses’ perspectives on patient safety in operating rooms within government hospitals in the Gaza Strip. It utilized a survey design targeting all eligible operating room nursing staff across three major government hospitals in the region.
To ensure comprehensive and transparent reporting of survey methodology and findings, the study adhered to the Consensus-Based Checklist for Reporting of Survey Studies (CROSS) guidelines. A completed CROSS checklist is provided as Supplemental Material to confirm compliance.
Study location and period
This study was carried out in 2023, prior to the Gaza war, within the operating rooms of the three main governmental hospitals in the Gaza Strip: Al Shifa Medical Complex, Nasser Medical Complex, and Gaza European Hospital.
Study population
The study included all nurses, regardless of gender, working in the main operating rooms of the selected hospitals in the Gaza Strip, as long as they met the inclusion criteria and were present during the study period. Nurses with <6 months of experience, volunteers, those assigned to minor operating rooms, and those who chose not to participate were excluded.
A census sampling method was employed, inviting every eligible nurse in the relevant departments to take part. To qualify, nurses needed to have worked in the operating room for at least 6 months before data collection. Recruitment was conducted during regular working hours with the assistance of hospital administration to ensure staff availability.
Sample size and sampling technique
All nurses working in the operating rooms of the three selected hospitals who met the inclusion criteria during data collection were included using a census sampling method. Of 162 eligible nurses, 150 participated, yielding a 92.6% response rate. A post-hoc power analysis was conducted using G*Power version 3.1 to assess the study’s statistical power. With a total sample size of 150, a significance level of 0.05, and assuming a medium effect size (Cohen’s h = 0.30), the power was estimated at 0.78. This indicates sufficient power to detect moderate differences in adherence rates among hospitals but suggests limited sensitivity for smaller effect sizes.
Data collection
The data were collected by five qualified data collectors comprising the researcher and four nurses, who received an explanation and training from the researcher regarding the study. This included its purpose, objectives, procedures, and instructions on how to collect data using the observational checklist.
Interview-based questionnaire
Data were collected from the nurses using a structured, pre-tested, and validated questionnaire. The questionnaire consisted of two sections: (1) Demographic and professional characteristics of the participants, such as age, gender, qualifications, specialized education, training courses, and years of experience and (2) The WHO’s “Patient Safety Assessment Tool,” which was utilized to evaluate patient safety in the operating rooms of governmental hospitals in the Gaza Strip. 11 The patient safety assessment tool comprised six domains, including: (1) Pre-operative general assessment, (2) pre-operative general preparation, (3) operating room preparation, (4) count and documentation, (5) intraoperative monitoring, and (6) identification of suspected risks.
Scoring system
The total number of responses (both positive and negative) was calculated separately for each domain by summing the number of “Yes” and “No” answers for all sub-questions within that domain. This total (Yes + No) was then divided by the number of sub-questions in the same domain to determine the overall level of participation or response rate. Subsequently, the results were classified based on the number of “Yes” responses (positive responses) and “No” responses (negative responses), and this classification was used to analyze response patterns within each domain.
Pilot study
A pilot study involving 15 participants was conducted to assess the questionnaire and data collection procedures. Based on the feedback received, modifications were made to the questionnaire to enhance its clarity and accuracy for use in the main study.
Ethical approval
The study protocol received approval from the Palestinian Health Research Council (Helsinki Committee approval no. PHRC/HC/1213/22). The participants provided their written informed consent to participate in this study.
Data analysis
Statistical analysis was performed using SPSS version 26. The process involved defining variables, data entry, data cleaning, and subsequent analysis. Continuous variables were reported as means ± standard deviation, while categorical variables were presented as percentages. The chi-square test was applied to assess differences between categorical variables, and one-way ANOVA test was used to determine the mean differences in quantitative variables, with a p < 0.05 considered statistically significant.
Results
A total of 150 nurses were included in the final analysis, with 78% male and 22% female participants. The average age was ~33 years. Nearly half worked at Nasser Medical Complex (48%), followed by Al Shifa Medical Complex (37.3%) and Gaza European Hospital (14.7%). Most nurses (71.4%) held a bachelor’s degree, 27.3% had a diploma, and 1.3% had a master’s degree. Specialized training in operating room care was reported by 43.3%, while 41.3% had completed related courses. On average, nurses had over 7 years of operating room experience and worked around 37 h/week (Table 1).
Socio-demographic characteristics of the study participants by hospitals.

Continuous variables were reported as means ± SD, while categorical variables were presented as percentages. The chi-square test was applied to assess differences between categorical variables, and one-way ANOVA test was used to determine the mean differences in quantitative variables, with a p < 0.05 considered statistically significant.
SD: standard deviation.
The study found that 74.7% (n = 112) of nurses across all hospitals adhered to pre-operative general assessment protocols, with the highest adherence at Al Shifa Medical Complex (80.4%) and the lowest at Gaza European Hospital (63.6%); these differences were not statistically significant (p = 0.299; Table 2). Additionally, there was strong compliance with key pre-operative tasks: 85.3% confirmed necessary investigation reports were included in patient files, 90% documented nursing assessments, and 86.7% recorded provisional diagnoses. The anesthesia plan was documented in 72% of cases, while 89.3% reported pre-anesthesia evaluations were done at least 2 h before surgery. Anesthesia consent was obtained and documented in 67.3% of cases. Nurses verified consents for high-risk surgeries and anesthesia in 86% and 65.3% of cases, respectively. Immediate anesthetist re-evaluations took place in 87.3% of cases, with 78.7% confirming blood loss risk assessments and 83.3% reporting nurse assessments of hemodynamic instability risk.
Responses of the study participants for the pre-operative general assessment by hospitals.

Continuous variables were reported as means ± SD, while categorical variables were presented as percentages. The chi-square test was used to examine differences between categorical variables, with a p < 0.05 considered statistically significant.
SD: standard deviation.
As detailed in Table 3, 85.3% (n = 128) of nurses across all hospitals consistently followed pre-operative preparation protocols, with Al Shifa Medical Complex leading at 87.5%, followed by Nasser Medical Complex at 84.7%, and Gaza European Hospital at 81.8%. These differences were not statistically significant (p = 0.799). Most nurses (88.0%) reported that ward staff fully completed the pre-operative checklist, and 82.7% confirmed that blood was prepared in advance for major and moderate surgeries. Patient identification procedures were generally well adhered to, with 87.3% verifying patient files for name and identity, 86.0% noting identity bracelets, and 62.0% confirming verbal identification at admission. Furthermore, 84.0% confirmed patient or family verification of identity, and 82.7% reported proper surgical site preparation. About 77.3% indicated the presence of signed surrogate decision-maker forms, and 73.3% confirmed appropriate surgical site marking by surgeons.
Responses of the study participants for the pre-operative general preparation by hospitals.

Continuous variables were reported as means ± SD, while categorical variables were presented as percentages. The chi-square test was used to examine differences between categorical variables, with a p < 0.05 considered statistically significant.
SD: standard deviation.
Consent for blood transfusions was documented in 81.3% of cases, and 68.0% reported complete pre-operative checklists by operating room staff. Antibiotic prophylaxis was administered within 2 h before incision in 73.3% of cases, and post-operative instructions were provided in 88.0%. Additionally, 76.7% verified patient identity and checklist review upon operating room admission. The “Sign In” portion of the time-out checklist was read and marked before anesthesia in 74.7% of cases, while 66.0% of nurses observed adequate patient preparation by surgical staff.
Table 4 shows that 76.0% of nurses reported adherence to operating room preparation protocols, with similar results across the three hospitals and no significant differences. Most nurses confirmed that patients were kept warm (82.7%), essential and backup equipment were checked (75.3% and 84.7%, respectively), and anesthesia machines were inspected (71.3%). Strong compliance was also seen in safety practices such as proper attire (83.3%), blood bank notification (87.3%), scrubbing (79.3%), electric grounding (82.7%), and availability of safety belts (84.0%).
Responses of the study participants for the operation room preparation, and count and documentation by hospitals.
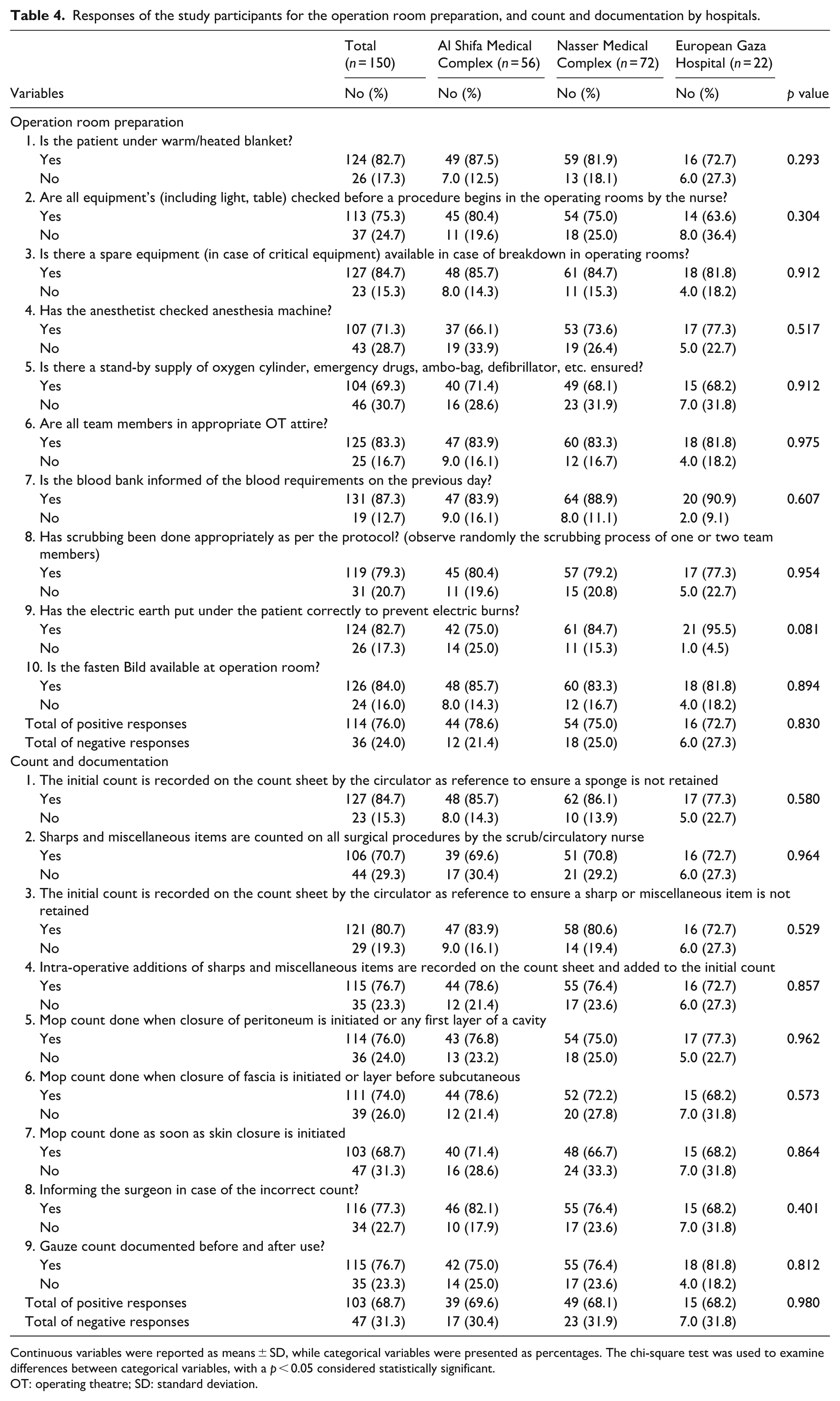
Continuous variables were reported as means ± SD, while categorical variables were presented as percentages. The chi-square test was used to examine differences between categorical variables, with a p < 0.05 considered statistically significant.
OT: operating theatre; SD: standard deviation.
In terms of count and documentation, 68.7% of nurses consistently followed protocols, including accurate counts of sponges (84.7%), sharps (80.7%), and mops at various closure stages. Most nurses (77.3%) reported communicating discrepancies to surgeons, and 76.7% ensured proper documentation of gauze counts. These adherence rates were consistent across all hospitals without significant differences.
Table 5 shows that 80.0% of nurses reported adherence to intra-operative monitoring, with rates of 83.9% at Al Shifa, 79.2% at Nasser, and 72.7% at Gaza European Hospital (p = 0.522). Key monitored parameters included heart rate (80.7%), temperature (78.7%), end-tidal CO2 (80.0%), and oxygen saturation (69.3%). Safety alarms were available (82.0%), vital signs were continuously monitored (71.3%), and a patient safety committee was present (79.3%). Additionally, 80.7% confirmed the time-out checklist was read before incision, 72.0% reported anesthesiologist presence, and 78.0% noted a quiet operating room.
Responses of the study participants for the intra-operative monitoring, and identify suspected risk by hospitals.
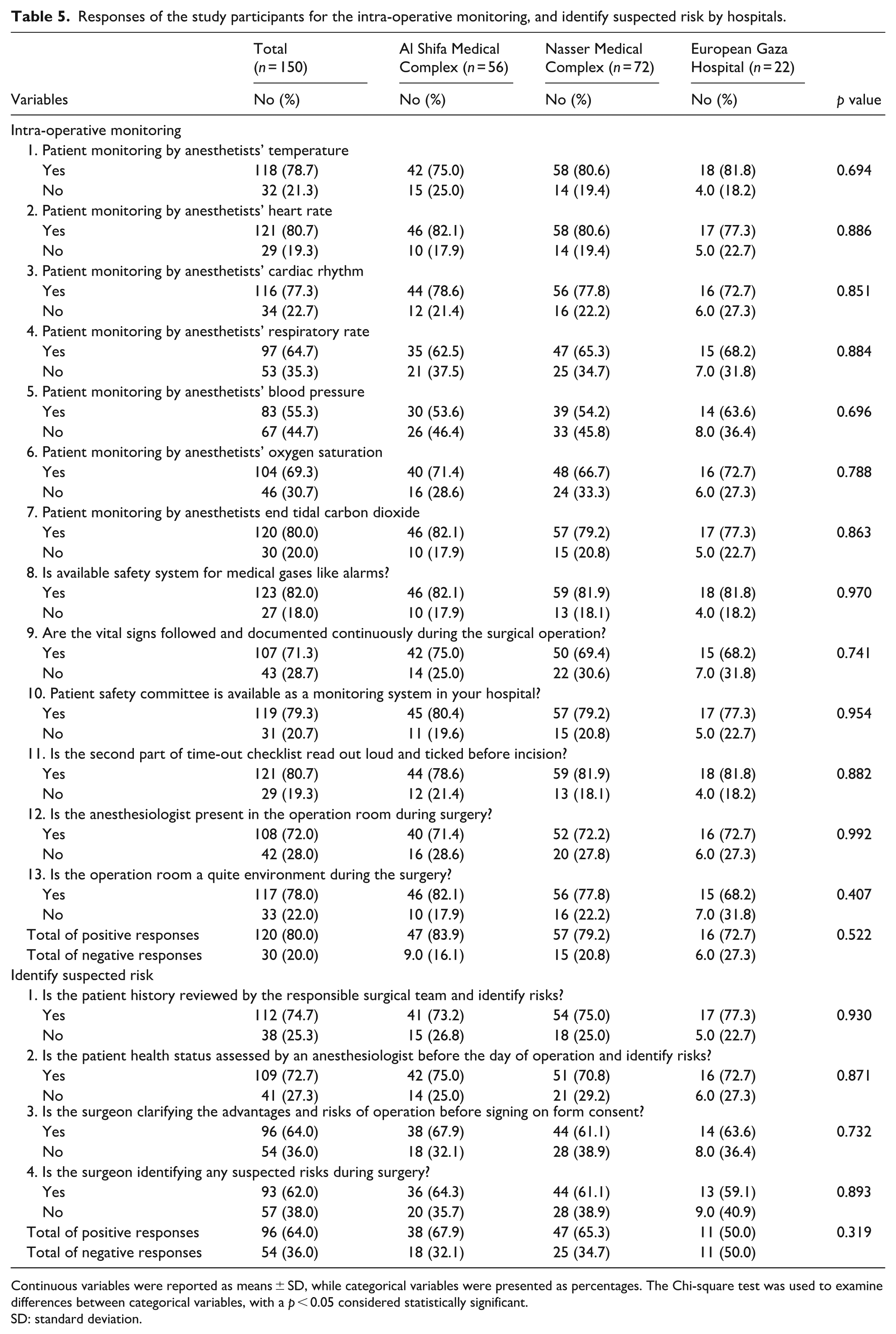
Continuous variables were reported as means ± SD, while categorical variables were presented as percentages. The Chi-square test was used to examine differences between categorical variables, with a p < 0.05 considered statistically significant.
SD: standard deviation.
Regarding suspected surgical risks, 64.0% of nurses reported proper identification and management, with rates of 67.9% at Al Shifa, 65.3% at Nasser, and 50.0% at Gaza European Hospital (p = 0.319). Other practices included reviewing patient history (74.7%), anesthesiologist pre-surgical assessments (72.7%), surgeon explanations of risks before consent (64.0%), and identification of intra-operative risks (62.0%).
Discussion
This study offers a detailed evaluation of preoperative and intraoperative patient safety measures in the operating rooms of three key governmental hospitals in the Gaza Strip, based on nurses’ perspectives. The findings reveal that while many safety procedures are consistently implemented and show encouraging trends, significant deficiencies remain particularly in areas such as risk identification, intraoperative monitoring, and documentation accuracy. These results are especially pertinent given Gaza’s challenging healthcare context, characterized by chronic resource limitations, political instability, and infrastructural constraints.
Preoperative assessment and preparation
Our results indicate a relatively high adherence to preoperative assessment protocols, with 74.7% of nurses reporting positive compliance. This supports Elsous et al.’s findings 5 of an overall favorable patient safety perception among Gazan nurses, despite variability across different safety domains. Documentation practices were notably robust, with over 85% of nurses confirming completion and recording of essential evaluations, investigations, and consent procedures. Timely pre-anesthesia evaluations were also reported by 89.3% of respondents, demonstrating effective implementation of foundational safety checks.
Regarding general preoperative preparation, 85.3% of nurses reported positive practices, echoing Bottcher et al.’s observations 6 that checklist usage is common but inconsistently applied in Gaza. Indeed, 88% of nurses confirmed full completion of preoperative checklists by ward staff, while 68% noted completion by operating room staff, reflecting findings from Paterson et al.’s WHO multi-country checklist study, 12 which linked rigorous checklist adherence to improved surgical outcomes. Nonetheless, the verbal confirmation of patient identity was only acknowledged by 62% of nurses, indicating a critical area for improvement in communication and verification protocols, especially vital in the high-stress OT environment.
Operating room preparation
Approximately 76% of nurses reported that operating room preparations met safety standards, a positive indicator given Gaza’s resource scarcity. The availability of essential equipment (75.3%), adherence to proper attire (83.3%), and the use of backup systems (84.7%) suggest a strong procedural culture within surgical teams. These results align with studies in other resource-limited contexts where operational readiness is often sustained through routine practice and informal protocols despite the lack of formal systems.13,14 Although Gaza European Hospital showed somewhat lower performance than Al Shifa and Nasser Medical Complexes in several areas, the differences were not statistically significant, likely reflecting standardized Ministry of Health policies and similar staffing across hospitals.
Count and documentation procedures
Compliance with counting and documentation of surgical materials was confirmed by 68.7% of nurses, the lowest adherence among the six evaluated domains. While sponge and sharp counts had relatively high compliance (84.7% and 80.7%, respectively), documentation during certain closure stages, such as skin closure was less consistently followed (68.7%). This partial compliance mirrors international concerns emphasizing that intraoperative communication and documentation are crucial to preventing retained surgical items, particularly in overburdened settings.3,15 The moderate adherence may be attributed to staff shortages, high surgical caseloads, and limited institutional oversight, underscoring an area requiring urgent improvement.
Intraoperative monitoring
Eighty percent of nurses indicated consistent adherence to intraoperative monitoring protocols, highlighting the professionalism of surgical teams. Vital parameters such as heart rate (80.7%), end-tidal CO2 (80.0%), and oxygen saturation (69.3%) were commonly monitored, whereas blood pressure (55.3%) and respiratory rate (64.7%) were less consistently tracked. This gap reflects wider trends in low-resource environments where monitoring suffers due to multitasking staff and limited or malfunctioning equipment.16,17 Additional concerns include the moderate availability of safety alarms (82.0%) and continuous vital sign documentation (71.3%), likely compounded by frequent electricity outages and inadequate biomedical maintenance in Gaza.
The observed adherence to the surgical safety checklist’s time-out phase (74.7%) compares favorably with global data from similarly high-pressure and conflict-affected settings, where compliance often ranges between 40% and 65%.16–18 Furthermore, the high rates of checklist completion by ward staff (88.0%) and preoperative site marking (73.3%) align with or surpass benchmarks from comparable contexts. These findings suggest that despite systemic challenges, Gaza’s governmental hospitals maintain a relatively strong safety culture during elective and semi-urgent surgeries. However, compliance during emergency surgeries, marked by urgency and limited surgical availability may be lower, a hypothesis warranting further investigation.
Identification of suspected surgical risks
This domain showed the lowest positive response rate (64.0%), encompassing critical activities such as surgeon-patient risk discussions, anesthesiologist evaluations, and thorough patient history reviews. Such low compliance may stem from systemic barriers like heavy caseloads, restricted operating time, hierarchical communication norms, and limited nurse involvement in these discussions, all of which undermine comprehensive risk assessment and informed consent.18–20 The protracted crises and overburdened health system may also contribute to procedural shortcuts, particularly in emergency settings. The low rate of risk identification highlights the need to strengthen structured briefings and encourage multidisciplinary communication to better manage surgical risks.
This study demonstrates that while Gazan government hospitals have integrated many WHO Patient Safety Assessment Tool components, significant system strengthening is needed, particularly in documentation, intraoperative monitoring, and risk identification. High compliance with basic protocols reflects a culture of procedural diligence despite chronic underfunding, unstable power supply, and import restrictions. Conversely, lower adherence to advanced monitoring and risk evaluation points to underlying structural challenges, including staff burnout, insufficient training on updated protocols, and limited ongoing professional development. The variability across domains further emphasizes the necessity for targeted interventions.
Given nurses’ frontline role, their insights are crucial for understanding compliance and gaps. Consistent with Sexton et al., 21 fostering teamwork, leadership support, and multidisciplinary communication can improve safety outcomes. Recommended measures include regular in-service training focused on intraoperative risk assessment, documentation, and monitoring technology use; establishing routine audits with feedback mechanisms; standardizing patient identification and informed consent protocols; investing in essential monitoring equipment, potentially with international support; and empowering nurses to actively participate in surgical briefings and risk assessments to enhance accountability and safety culture.
Finally, the chronic conflict in Gaza heavily impacts healthcare, contributing to staff shortages, equipment gaps, and disruptions that affect patient safety adherence, especially in monitoring and risk identification. Although data were collected before the latest conflict, ongoing instability likely worsens these challenges, particularly in emergencies. This study offers a crucial baseline for surgical safety in conflict zones and highlights the need for adaptive strategies to improve care quality and resilience.
Strengths and limitations
A major strength of this study is its exceptionally high response rate of 92.6%, achieved through a census-based sampling strategy. All eligible operating room nurses from the three participating government hospitals were invited to participate, and nearly all agreed. This high level of engagement likely resulted from several key factors. First, the use of peer data collectors’ nurses embedded in the clinical environment and trusted by their colleagues fostered openness and participation. Second, the study’s focus on surgical patient safety resonated with the nurses’ daily responsibilities, increasing its perceived relevance. Third, administrative support from hospital leadership allowed staff to complete the survey during work hours, further facilitating participation. While some of these factors such as centralized health governance and professional solidarity in conflict settings may be specific to Gaza, the methodological approach used here offers practical strategies that could be adapted to similar low-resource or high-stress environments. Another strength is the inclusion of multiple major government hospitals across the Gaza Strip, enhancing the representativeness and generalizability of the findings within this conflict-affected region. The relatively large sample size and participation rate further support the internal validity of the results and may provide a useful reference point for patient safety practices in other under-resourced or emergency settings.
Despite these strengths, several limitations must be acknowledged. First, the study relied on self-reported data, which can be subject to social desirability bias, especially in high-stakes clinical environments such as the operating room. Survey participants may overreport adherence to safety protocols such as surgical time-outs and checklist use, compared to actual observed behaviors. Research by Poon et al. 22 highlighted this issue, demonstrating discrepancies between reported and observed compliance with surgical safety checklists, and cautioning against relying solely on survey data when assessing patient safety behaviors. Second, the study focused exclusively on the perspectives of nurses, omitting insights from physicians, anesthesiologists, and other surgical team members. This presents a missed opportunity to assess interprofessional alignment and communication, particularly concerning perceived safety practices. Differences or concordance between professional groups, especially across hierarchical gradients, are known to be predictive of safety culture and team effectiveness in surgical settings. Third, existing evidence suggests that nurses may report higher compliance rates for safety practices than other clinicians, potentially inflating perceptions of adherence. 22 Without triangulation from direct observation or input from other roles, the findings may overestimate actual implementation of protocols such as time-outs and checklist verification. Future research should consider mixed-method approaches, including observational studies, structured audits, and interviews across multidisciplinary teams. Such approaches would yield a more nuanced and accurate understanding of actual practices, underlying challenges, and interprofessional dynamics affecting patient safety implementation.
Conclusion
This study provides a detailed evaluation of preoperative and intraoperative patient safety practices in government hospitals in the Gaza Strip from the nurses’ perspective, revealing a generally positive adherence to safety protocols despite the region’s resource limitations and systemic challenges. High compliance was observed in areas such as preoperative assessment, preparation, and operating room readiness, while notable gaps remained in risk identification, intraoperative monitoring, and documentation. These findings underscore the critical role of nurses in ensuring surgical safety and highlight the need for targeted improvements in training, policy enforcement, infrastructure, and multidisciplinary collaboration. Strengthening these areas can enhance patient outcomes, support frontline staff, and help align local practices with international safety standards, especially in conflict-affected and resource-constrained settings like Gaza.
Supplemental Material
sj-docx-1-smo-10.1177_20503121251393340 – Supplemental material for Assessment of preoperative and intraoperative patient safety measures in government hospitals in the Gaza Strip: The nurses’ perspective
Supplemental material, sj-docx-1-smo-10.1177_20503121251393340 for Assessment of preoperative and intraoperative patient safety measures in government hospitals in the Gaza Strip: The nurses’ perspective by Mohammed A. Abu Rahmah, Bothyna B. ELssyed Etewa, Fatma Al’Haj Ahmad and Abdel Hamid El Bilbeisi in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121251393340 – Supplemental material for Assessment of preoperative and intraoperative patient safety measures in government hospitals in the Gaza Strip: The nurses’ perspective
Supplemental material, sj-docx-2-smo-10.1177_20503121251393340 for Assessment of preoperative and intraoperative patient safety measures in government hospitals in the Gaza Strip: The nurses’ perspective by Mohammed A. Abu Rahmah, Bothyna B. ELssyed Etewa, Fatma Al’Haj Ahmad and Abdel Hamid El Bilbeisi in SAGE Open Medicine
Footnotes
Acknowledgements
We gratefully acknowledge the nursing staff who generously contributed their time and expertise to this study. We also extend our appreciation to the hospital administrations and data collectors for their essential support throughout the research process.
Author contributions
M.A.A.R. was responsible for the conceptualization, data collection, data curation, formal analysis, and writing of the original draft. B.B.E.E. contributed to the methodology, supervision, validation, and writing review and editing. F.A.A. conducted the literature review, assisted in data collection and project administration, and contributed to the original draft. A.H.E.B. performed the statistical analysis, interpreted the results, and contributed to the writing review and editing, as well as supervision. All authors have read and approved the final version of the article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.