
Abstract
An increase in providing hospital bedside imaging examinations could be contributing to the risk of musculoskeletal injuries among imaging professionals. Given the increasing demand for portable bedside imaging, a research project was conducted in three phases: (1) interviews and focus group sessions, (2) full-scale mock-up sessions where occupational stakeholders created prototype rooms, and (3) evaluation sessions of inpatient room prototypes by all stakeholders. The study data from diagnostic medical sonographers (DMS), cardiac sonographers (CS), vascular technologists (VT), and radiographers (RTs) were retrospectively pulled from the overall research to address the following research question: What hospital room designs and components facilitate or hinder medical imaging professionals in providing bedside imaging? Data analyses utilize constant comparative analysis, quantitative counts, and discourse analysis across all three phases of the project. The results highlight the importance of a working area surrounding the patient’s bed that allows for imaging and patient care activities. And this study provides new evidence to inform design considerations that could facilitate the performance of diagnostic patient care at the bedside and reduce exposure to work-related musculoskeletal disorder risks factors.
Sonographers (US) and radiographers (RT) are medical imaging professionals who work in clinic settings, rooms of hospital patients, hospital emergency departments, and procedure rooms to obtain internal views of patients via ultrasound and x-rays, respectively. Sonographers typically work as general diagnostic medical sonographers (DMS), or they can specialize as cardiac sonographers (CS) or vascular technologists (VT). A hospital is the primary employment site for 59% of RT 1 and 68% of DMS (including CS and VT). 2 All imaging professionals who work in hospitals spend significant portions of their work time positioning patients and equipment and working with computers. Positioning patients and imaging equipment often requires high levels of physical effort.
Published studies consistently report musculoskeletal (MSK) symptom prevalence of 50% to 80% in surveyed CS, which is similar to symptom reports for DMS and VT.3–7 Research shows that the prevalence of MSK discomfort in RTs is quite high as well, at 60% to 75%, similar to US and other direct care medical professionals such as nurses.8–10 These statistics indicate that a large percentage of imaging professionals may be working while experiencing pain.
Many studies of imaging professionals are epidemiological in nature, conducted to describe work activities, assess morbidity, and identify risk factors that could contribute to the high prevalence of MSK symptoms in these health care workers. In general, few studies have focused on understanding the challenges imaging professionals face in acquiring images in patient rooms, although portable bedside examinations that entail taking the ultrasound equipment to the patient have been associated with work-related musculoskeletal disorders. 11 Further, portable exams and the factors associated with them, including room size, moving furniture to set up for the exam, and awkward working postures, were issues raised by both US and RT in a study conducted in the USA by Sommerich et al.12,13 The objective of that study was to identify issues and develop interventions to address some of the higher priority issues identified by study participants. Similar concerns about portable exams, in particular the lack of space in patient rooms contributing to poor work postures, were also raised by sonographers in a study conducted in Sweden. 14
Roll et al. 15 provided observational data while working with patients, and it was their conclusion that the work environment and equipment design could be contributing to the risk factors among DMS and VTs. However, no significant differences were noted in exam efficiency when portable examinations were completed with laptop-style ultrasound machines (compact, lightweight) versus conventional full-size ultrasound machines on wheels. 16 Smaller equipment could lead to less physical strain on the imaging professionals during transport, and although it may be more easily positioned in a crowded hospital room, the DMS would still need to maintain proper body posture while completing examinations. As such, laptop-style ultrasound machines may still be associated with musculoskeletal symptoms. In the Roll et al. 15 study, the observed DMS did make use of height-adjustable examination beds, yet the bed height continued to be associated with poor body posture. In a study of patient handling–related injuries that occurred during a seven-year period preceding the start of a minimal lift policy in a large hospital system in the USA, Pompeii and colleagues 17 reported that 25% of injuries to RT were associated with lifting patients, repositioning, or pulling them up in bed.
In light of these concerns for imaging professionals when working in patient rooms, we proposed to take a more expanded examination of work performed in hospital patient rooms to determine how the designs of these rooms affect hospital workers from varied occupations, including imaging professionals. The goal of the research was to develop design recommendations informed by a multiphase participatory process that engaged hospital workers, patients, and visitors.18–20 For this paper, the study data from the imaging professional participants (DMS, CS, VT, and RT) were retrospectively pulled from the three phases of the study in which they participated to provide a focused examination to address the research question: What hospital room designs and components facilitate or hinder medical imaging professionals in providing bedside imaging?
Methods
Thirty-five imaging professionals (DMS, CS, VT, and RT) consented to participate in a University Institutional Review Board–approved study, staged in multiple phases, that engaged members of hospital staff from 23 occupations that spend time working in patient rooms.18–20 Table 1 provides demographic information on the 35 imaging professionals who participated in the study and the phases of the study in which they participated. To manage the scope, the study focused on medical/surgical (med/surg) rooms. Participants were volunteers who responded to posted flyers, word of mouth, recruitment presentations at staff meetings, or direct invitation to participate in the study. The data, which were generated from multiple sessions across the three phases of the study in which hospital staff participated, provided in-depth information about what components were needed in an ideal hospital room, meaning a room that facilitates the work of all of the occupations that work in the room. Given the varied data sources that were captured, a mixed method analysis was used that included constant comparative analysis, quantitative counts, and discourse analysis.21–28 Additionally, hypothetical zones within the patient room were initially imbued on the overall interior space to better track work tasks.24–28 This mixed methods analysis generated descriptive statistics as well as rich qualitative data. Word searches were used across the full project’s database, and a member check was completed to add content validity.
Demographics of Study Participants and Study Phase Participation.
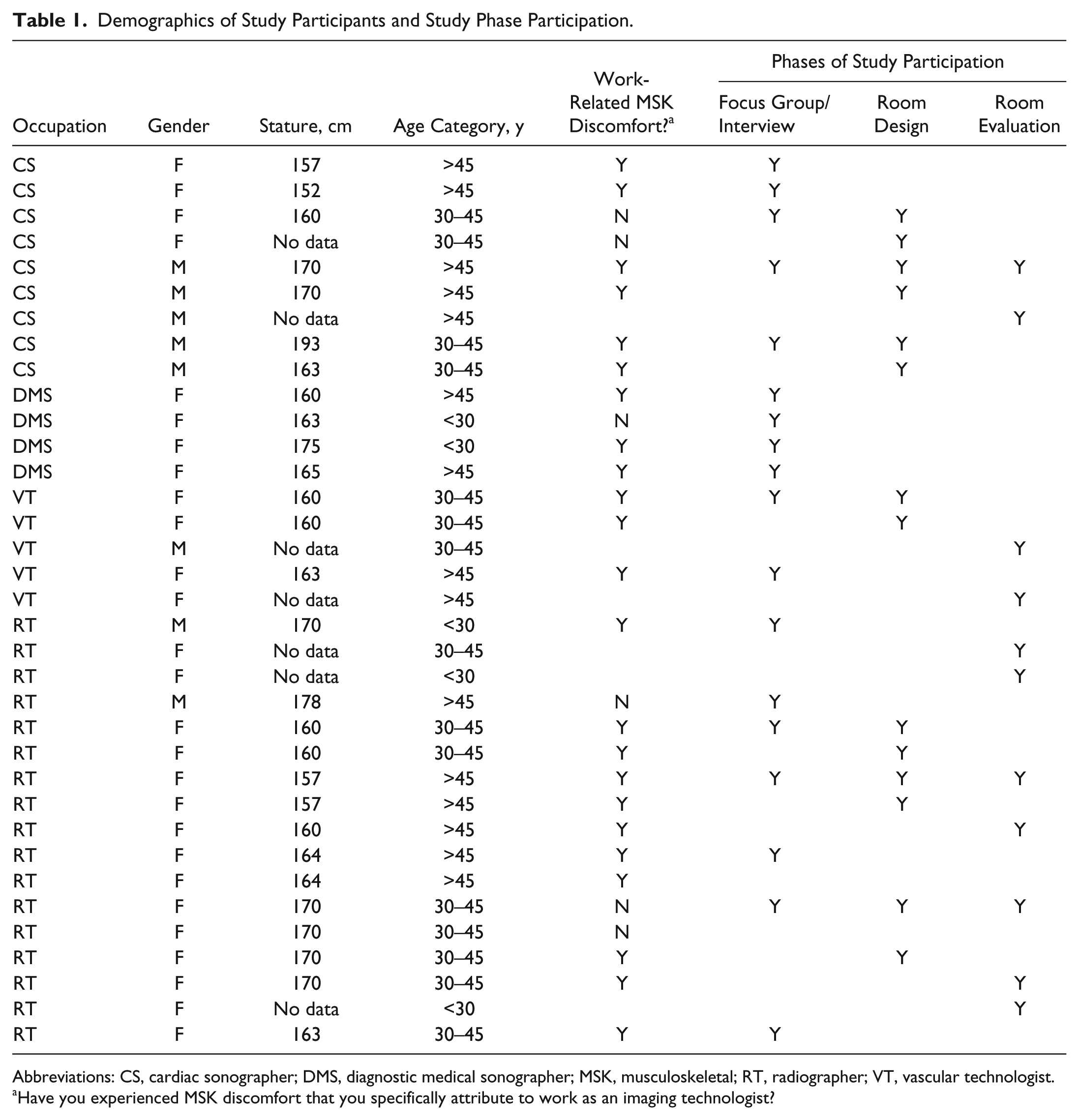
Abbreviations: CS, cardiac sonographer; DMS, diagnostic medical sonographer; MSK, musculoskeletal; RT, radiographer; VT, vascular technologist.
Have you experienced MSK discomfort that you specifically attribute to work as an imaging technologist?
Starting Phase: Focus Groups for Discovery
The objective of this phase was to learn from hospital staff members (18 imaging professionals) how the design of the patient room in which they work facilitated or hindered their work (e.g., reduced productivity, required more physical effort, etc.). Focus group and interview sessions consisted of occupationally homogeneous groups. Prior to attending a session, participants completed a questionnaire about interactions they had with objects and elements present in hospital patient rooms. They were requested to take photos of elements of patient rooms without patients or visitors that either facilitated or hindered their work (Figure 1). At the start of the focus group or interview session, the participants were shown photographs, some from research participants and others provided by the research team. The photos were used to seed the discussion about the participants’ issues and concerns with the setup and design of the patient rooms in which they worked.

Participant photograph of a typical hospital room that is difficult to work at the bedside.
The main categories of room design parameters were shown to the participants to help them understand the scope and range of what was of interest to the research team: room size and shape, room layout (including zones, furniture, etc.), and task-based design components (including electric outlets, storage, etc.). A list of room components was then shown to the participants. Specific examples of items were provided under each of these broad headings (e.g., utilities: electrical outlets, light switches, reading light, window coverings, blinds/curtains, TV controls, nurse call buttons, mounted computer, and computer on wheels). Following the discussion, the participants were shown the issues that they had discussed, which had been documented on sticky notes by two members of the research team. Participants were asked to cluster the issues and label the clusters. Following this activity, each participant identified the individual issues or clusters of issues that were most important to him or her using colored “priority” stickers.
Room Design Phase
The objective of the next phase was to provide the opportunity for hospital staff members (including 14 imaging professionals) to build a full-scale mock-up of a patient room that would work for everyone, including staff, patients, and visitors. For staff, this meant the room design should facilitate the performance of their work and not add time to performing their work tasks to serve patients and visitors, feel like a healing space, and facilitate the healing process. Participants in this phase were recruited from the same 23 occupational groups that participated in the prior phase. However, in this phase, occupationally heterogeneous participant groups were constructed to avoid designing a room that only worked for a single occupation. At least one imaging professional participated in 7 of the 27 room-building sessions held in this phase.
Participants were given a defined square footage (300 sq ft; 27.9 sq m) that was bound with immovable walls and contained a hospital bed and a sleeper/sofa/couch for visitors as a starting point. Participants worked with actual and representative furnishings and room elements to completely outfit the full-scale mock-up space. The room design had to incorporate a fixed list of items, but participants had full control over where items were located (including the bed and the bathroom), could choose different versions of some items (e.g., hinged or sliding bathroom door), and could add optional items (e.g., hooks on certain doors or walls, labels on light switches, remote control of window blinds). Audio, video, and digital photography were used to record the progressive building of the room designs. The participant team gave a video-recorded guided tour at the end to explain the reasons for their choices and demonstrate how the room would work for each participant in their group.
After running 27 room design sessions, the researchers worked to compare and contrast the 27 different room designs that had been created. As a result, the researchers collapsed the 27 designs into five hybrid room designs. The consolidation was based mainly on the location of the head of the bed related to the hallway door and whether the bathroom was inboard (bathroom near hallway and entry door) or outboard, which meant that the bed was closer to the hallway door. The eventual five hybrid room design prototypes incorporated some modification recommendations from patients and family members, environmental service staff, and architects.
Room Design Prototype Evaluation Phase
The objective of this phase was to identify any remaining concerns of hospital staff members, including potential design conflicts (design elements that work for one group but may cause issues for another), to ensure that the final designs would meet the needs of everyone who works in or spends time in a med/surg hospital patient room.
This final phase was devoted to discussions involving imaging professionals (N = 11) and other members of hospital staff, for the purpose of evaluating the five hybrid room designs, with each session typically reviewing three of the five rooms (due to time constraints). Each room was viewed by seven to nine groups of participants, and all five rooms were reviewed by at least one imaging professional. Small group sessions began with a review of the top view diagram of a room and then an actual tour of the space of that room prototype. Participants were given a set of surveys, one survey per room, to rate each room and its features while they were in the room. After each room was toured, the group discussed what they liked and disliked about each room design. This process was repeated for each room that was shown in a given session. At the end of the session, participants were asked to identify the rooms that they favored most and least. Conflicts over the space and room features were also discussed to identify trade-offs and, where possible, achieve resolution. The discussion of conflicts was conducted near the end of the session.
Results
Starting Phase: Focus Groups for Discovery
In the first phase, 18 imaging professionals participated (5 CS, 4 DMS, 3 VT, and 6 RTs). The information provided regarding the room design features was first analyzed separately for each session. Based on the counts of the priority stickers, a system of spheres was used to illustrate the level of emphasis and importance of each of the room features. The spherical analysis provided a visual display of the items both by importance and the overlap of their interaction. See Figure 2 for the complete analysis of the imaging professionals’ priorities of room design features.
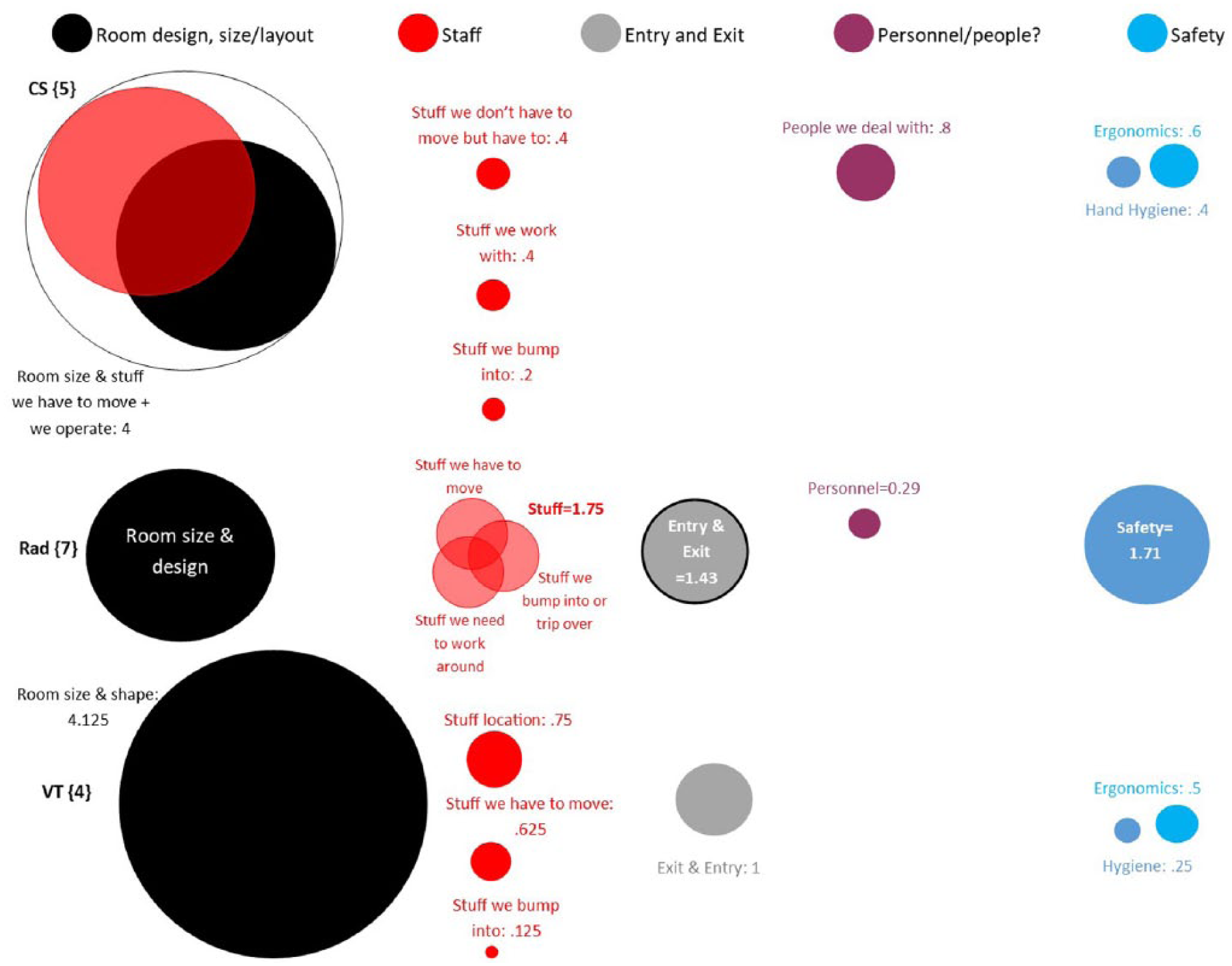
Analysis of focus group data based on CS, RT, and DMS’s interactions within the hospital room parameters and specific items.
One example of the evocative data collected was from the CS group, whose members indicated that room design, size, and layout were most important (black sphere) and definitely interact with “stuff” they have to move and operate. Specifically, one of the CS participants discussed how imaging innovation was hampered by working at the patient’s bedside: I was exclusively trained to make 3 dimensional imaging studies of the heart. This required a full size ultrasound machine to be taken to the patient room for 3D imaging studies. Due to all the problems with access, these studies have been phased out. I was one of the last people on the staff to have this training and this may be a major issue in the field with the increased use of 3D technology. No solution exists for getting these 3D cardiac ultrasound studies in the patient’s room.
Referring to a photo provided by the research team, a participant stated: I don’t like the blinds, they have to be dark. But I think that there could be darkening curtains, so that would be a must. You have to make the room dark so we can see our ultrasound image. So that’s really important to have that feature in every room, darkening curtains. You can have both, the light, but you’ve got to have access to the blinds so we can lower them down and make the room dark.
In contrast, the DMS participants tended to rate the room size and shape as most important. They raised concerns about their interactions with things and people in the room, particularly with reference to touching or bumping into them when trying to maneuver their machine within the room. DMS were concerned with the exit and entry ways for moving equipment. One DMS participant described some of the difficulties with performing imaging and moving the hospital room furniture: These patients have many ports, hoses, and lines that can be easily disconnected so rearranging the bed is a hazard. Likewise the rooms require a great deal of furniture to be rearranged. The nightstand is the biggest problem as it often is positioned so that it’s hard to move the bed to the left. Rearranging the furniture in the room can take 10–15 minutes of work added to the cardiac echogram. This is a very inefficient use of a professional’s time with patients.
DMS participants discussed concerns for hitting the venous compression pump, commonly hung on the footboard of the patient bed, with their equipment. Cords, tubes, and lines are a major concern for DMS with respect to worker and patient safety. “The bed should have a system for ‘tucking up’ all the cords and wires to prevent tripping hazards and accidental disconnections.”
The RT participants also prioritized room size and design as a major concern and specifically brought up the problem of needing to deal with stuff/clutter in the patient room. On the other hand, they described that location, mobility, and what they bump into were interrelated factors. The RTs also prioritized worker safety as a concern when working in a patient’s room; extra time and effort (due to machine and personnel maneuvering) has to occur to ensure RTs are not physically “trapped” in the room and then exposed to radiation during image acquisition.
Room Design Phase
In this phase, there were six CS, two VT, and six RTs who joined other health care professionals in a total of 27 groups that worked to construct med/surg patient rooms through a collaborative process.
By requiring that a bathroom be designed by each interdisciplinary group, it quickly became clear that imaging professionals were much less engaged in the design of the bathroom compared to their engagement in other elements. For example, few of the imaging professionals entered the bathroom area at all or presented elements of the bathroom during their team’s walkthrough. In contrast, they were actively engaged in determining the placement of the bed, utilities (i.e., light switches and electrical outlets), and the overall room space. Some of these elements are located in the “clinical zone.”25–27 In the patient room, the clinical zone is defined as a work area for health care staff that is separate from but in close proximity to the “patient zone.” Interestingly, the imaging professionals made it clear, in their contribution to the room design groups, that using their imaging equipment required moving into the patient zone so that their clinical work could be accomplished. They were also explicit about their preferred location of the head wall utilities and electrical outlets. Often during the room design process, imaging professionals would place (i.e., affix pictures of) several electrical outlets on the walls of the clinical and patient zones to emphasize the need for access to more outlets and would locate that at a specific height to avoid having to repeatedly bend over (in each room) to plug in and unplug their imaging equipment. They also expressed a strong desire for uniformity, from \room to room, in the organization and labeling of light switches, location and types of lighting, and type and control location of window blinds. Imaging professionals typically need to turn off lights or dim them to perform an imaging examination, so this uniformity would reduce confusion and likely produce some time savings.
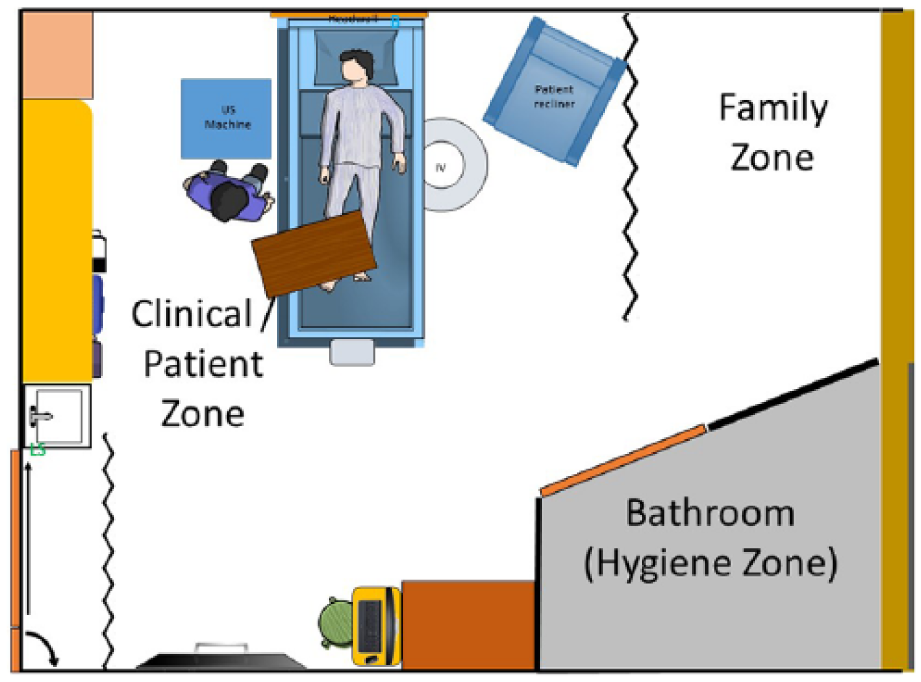
The area designated for the family—“visitor/family zone”25–27—was also of great interest. CS and VT participants mentioned that they preferred to avoid having visitors and family asking about the imaging results, so the farther visitors were located from the clinical-patient zone, the better. Such queries are uncomfortable because sonographers are not permitted to discuss the images they acquire; images must be interpreted and reported by a physician. For RTs, the use of ionizing radiation precludes having visitors or family in the room for the examination, which meant designing a room family and visitors could easily exit. The visitor/family zone was a difficult space to negotiate since the imaging technologists wanted this area isolated or minimized so that more space could be devoted to the clinical-patient zones. One example of room design that had both a CS and VT as participants actively involved was an outboard bathroom and series of privacy curtains for the patient and the visitor/family area (Figure 3). Novel or inventive ideas contained in the room designs were identified by the research team and were subsequently rated for their innovativeness. A list of ideas attributed to CS participants appears in Table 2.
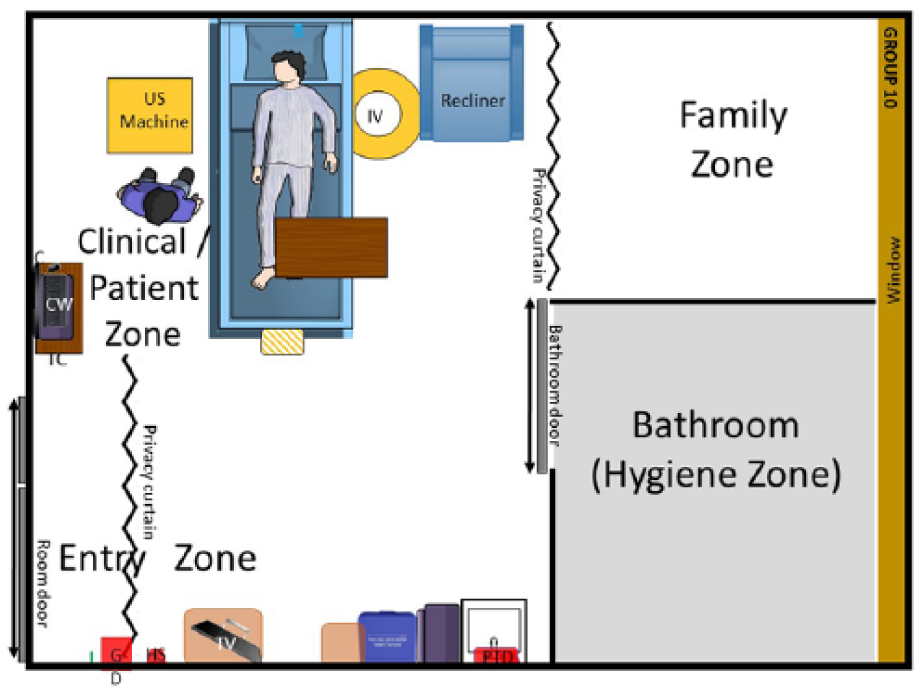
Room design that had both a cardiac sonographer and a vascular technologist’s input into the design for imaging at the bedside.
Cardiac Sonographers’ Innovative Input to Include in a Properly Designed Hospital Room. a
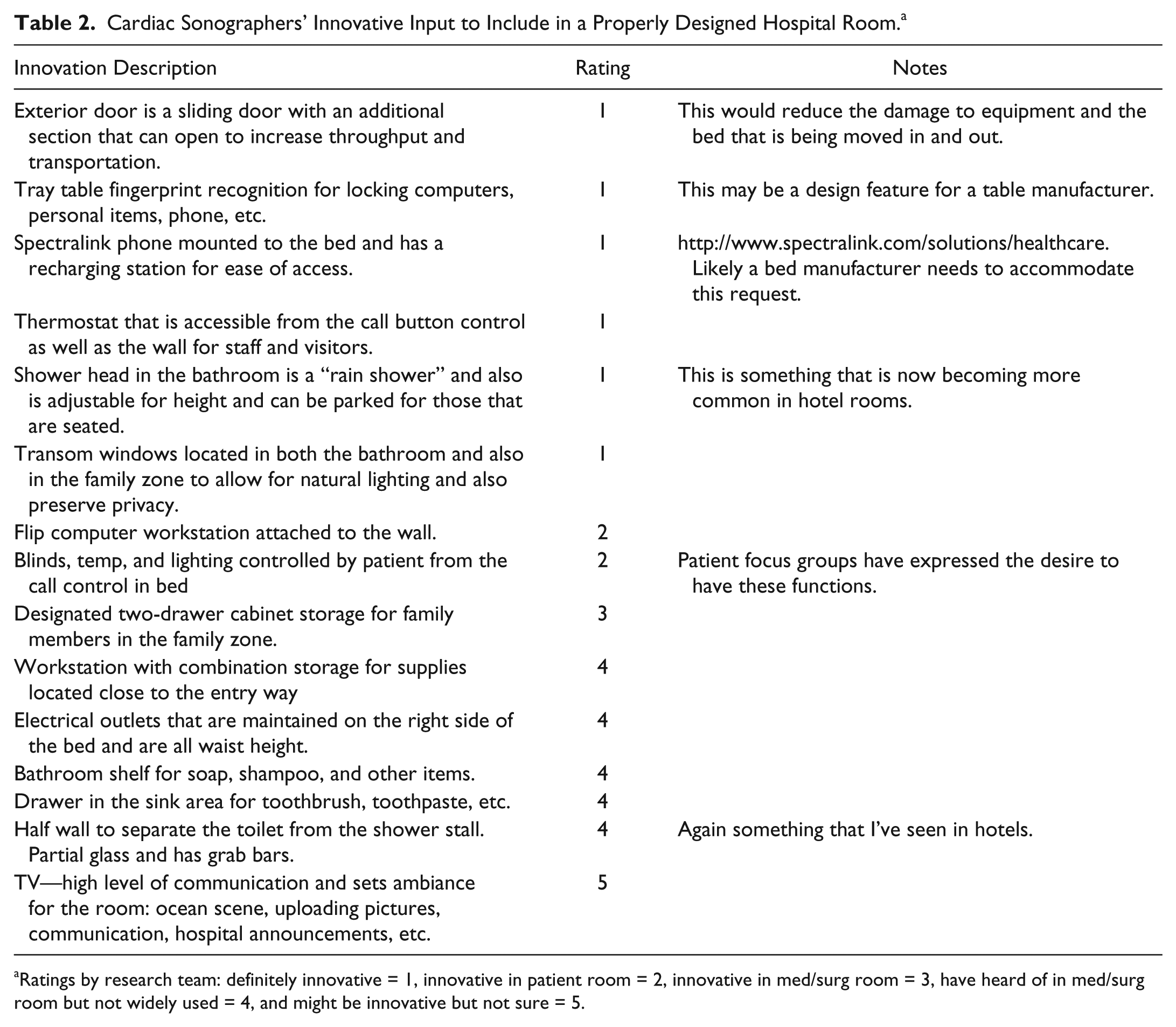
Ratings by research team: definitely innovative = 1, innovative in patient room = 2, innovative in med/surg room = 3, have heard of in med/surg room but not widely used = 4, and might be innovative but not sure = 5.
Room Design Prototype Evaluation Phase
In the final phase of the project, 11 imaging professionals participated in the rating of the five final hybrid room design prototypes, three shown by rotation in a session. These participants provided input and ratings with 7 RTs participating (N = 21 room reviews), 2 CS participating in 1 session (N = 6 room reviews), and 2 VTs participating (N = 6 room reviews). A total of 33 complete room reviews were submitted. Table 3 demonstrates a sample of the evaluation comments relative to the room components that were nested within the room designs that were shown to a participating RT and VT.
Room Evaluation: Evaluation of Room Components and Reviews of the Room Designs Shown to Interdisciplinary Teams.
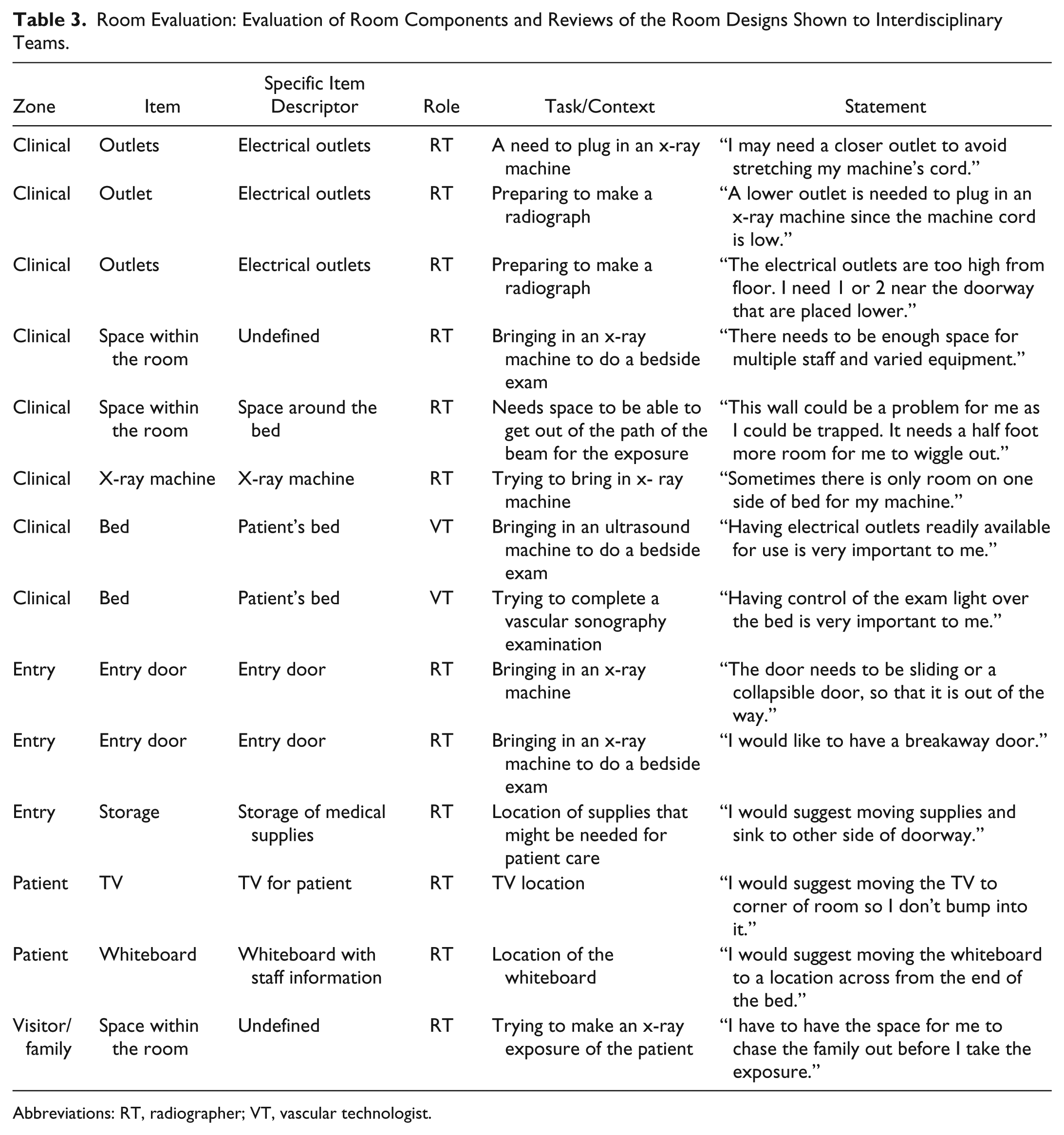
Abbreviations: RT, radiographer; VT, vascular technologist.
The room prototype layout No. 1 was the clear favorite of the imaging professionals (see Figure 4). The room had an open entryway (rather than an entry hallway) and outboard bathroom, and it provided open access to both sides of the patient bed and a split headwall with a number of electrical outlets on either side of the bed. Imaging technologists were united on the need to have easy access to enter the room and set up their imaging equipment. For imaging professionals, room designs with an inboard bathroom with a swinging (hinged) bathroom door complicated bringing imaging equipment into the room. They also reinforced the desire to be able to position the patient so that high-quality imaging could be accomplished at the bedside. Control of lighting, window shades, and other environmental conditions were essential so that they could visualize their work on the computer screen of their imaging equipment. Participants acknowledged that other patient care services conducted at the bedside by physicians, nurses, and dietitians often took priority in that they would typically be completed before an imaging professional would enter the room and complete their imaging examination.
Example room that was favorably rated by radiographers, cardiac sonographers, and vascular technologists.
Discussion
This subset of participants (DMS, CS, VT, and RT) provided specific information on how they perform their unique imaging tasks at the patient’s bedside and how med/surg patient room design and components often posed challenges to completing their work. In the design and evaluation phases of this study, imaging professionals were given the opportunity to work with colleagues from other occupations to design and critique patient rooms that were intended to facilitate the work of all members of hospital staff who work in patient rooms. Empirical evidence on workload for imaging professionals is scant; however, a study completed by Village and Trask 29 observed 11 DMS and included postural assessment. They followed this cohort for an entire shift across six hospitals. They found that DMS did make some equipment adjustments for imaging patients; however, they held their right arm statically for 73% of the exam time, and the variance in arm position was dependent on the exam type. 29 In this same study, VT were observed to exhibit trunk twisting and reaching across with their left arm to augment blood flow when evaluating lower extremity venous exams. 29 Although this only represents descriptive information about these imaging professionals, it would help explain their inherent need for space around the patient’s bed. It also underscores the desire for room designs that allow for the ability to position their equipment and make adjustments that will facilitate their work with the patient. A similar study was conducted with DMS that followed them on portable exams to the neonatal intensive care unit, and similar findings were noted. 30 No statistically significant changes were detected between pre-post measures for work demands, physical and mental health, or pain scores as a result of portable scanning sessions. Interestingly, that cohort of DMS was given space around the infant isolet to conduct their work, which may have contributed to a lessening of the work demands and personal stressors. In the current participant group of imaging professionals, 80% of those from whom the data were collected (n = 22 of 35) reported experiencing MSK discomfort that they attribute to their work with patients. This is similar to previously published reports.6,7,31–35
In an interventional study by Pais et al., 36 RTs commonly had the following poor postures: rotating the trunk and lifting of the arms, hip flexion, standing for prolonged periods of time without rest, exertion to hold equipment, and handling heavy and unconscious patients. This observation underscores the reason that the current study of RT made specific critiques of the various hybrid room designs. The room layout No. 1 that was the favorite design of the imaging professionals provided a lot of area around the patient bed (clinical zone) to not only position the patient for imaging but also allowed for handling imaging equipment such as digital imaging receptors or computed radiography cassettes. The RT participants in the current study also made it clear that visitors and family members needed to have passage to exit the room to avoid x-ray exposure, as did the RTs. Space for two RTs, one positioning the patient and the other to adjust the x-ray equipment, takes up significant space and could result in “trapping” one of the radiographers in a room that is too narrow.
A recent publication by Quan et al. 37 described the development of an evidence-based set of tools to assist architects and designers when creating highly functional hospital patient rooms. As part of their work, they state that no prescriptive numbers (e.g., space size, distance, or length of the headwall) are provided because they feel that an optimum number of features would depend on an in-depth understanding of the needs of patient care and the budget for a project. 37 Certainly this detailed analysis of the data provided by the imaging professionals in the current study demonstrates that diagnostic bedside imaging requires specialized equipment, control of the environment (e.g., lighting), work space for personnel, and safety precautions. Throughout this project, imaging professionals made it clear that conducting imaging examinations in the patient’s room is impacted by furniture and other room components (“stuff”) that impose constraints and interference for them in the course of conducting their work.
While some authors describe separate zones within the patient room, the current study demonstrated the great extent of the overlap between the clinical zone and the patient zone. Virtually all of the imaging professionals’ time in the patient room is spent performing clinical work at the patient’s bedside. CS often image the heart from the patient’s left side, while the DMS commonly access the right side. RT and VT position themselves and their equipment in relation to the body part being examined, so the size of the clinical zone for imaging is expansive and varies. It was also clearly noted that electrical outlets were needed for plugging in some types of imaging equipment. Outlets needed to be easily accessible and placed throughout the medical imaging professional’s working area. A diagram has been constructed that attempts to represent this clinical zone that takes up the majority of the patient room space (Figure 5). This newly defined clinical zone should ideally be free of stuff or room components that would result in bumping into or the need to move objects out of that area in order to work.
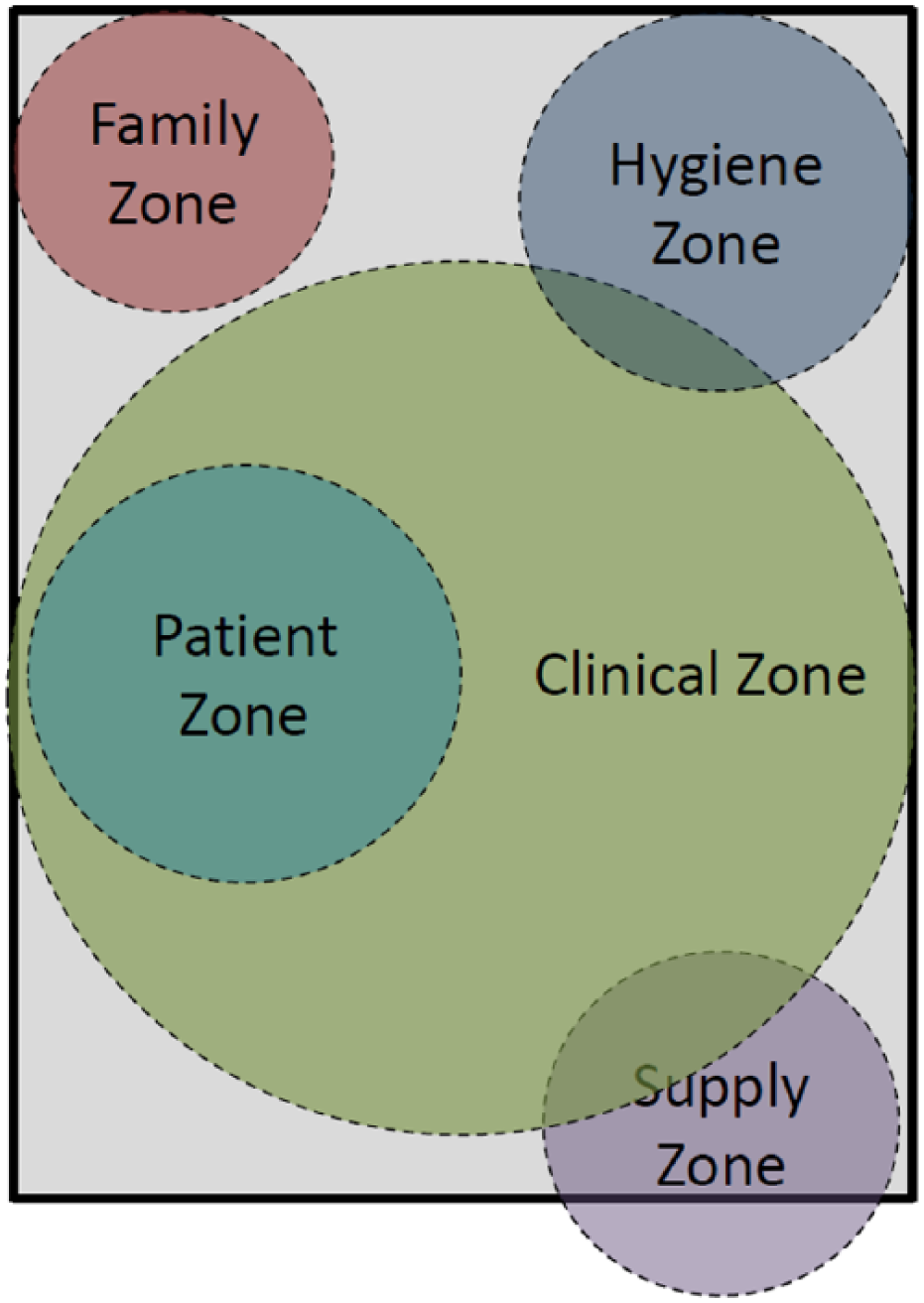
Adjusted zone designations based on in-depth analysis of medical imaging professionals’ data from focus group, room design, and room design evaluation phases of the study.
The patient room entry zone was highly evaluated by imaging professionals. Through the interviews, observations, surveys, and discourse analysis, it became clear that pushing imaging equipment into the patient room was a paramount concern. The door itself was highly discussed, and the need for a breakaway portion of the doorway was added to give more room for equipment and also for transport of beds to the imaging department. During the room design evaluation phase, it was common for imaging professionals to role play and push simulated imaging equipment through the entry zone for evaluation. It was through role playing that the movement of imaging equipment into the room and setting it up at the bedside was emphasized. They also demonstrated how a lack of space contributes to contorted body postures while performing their diagnostic work.
The preference of the RT was to provide a smaller visitor-family zone in order to provide more space for the patient and clinical zones. This would provide more space for the RT to work, especially in situations where there are two RT and they are wearing lead aprons to shield against scatter radiation. Further, family and visitors must leave the room prior to RT doing their work, so this adds to the perception that there is no need for a larger family space. In contrast, DMS, CS, and VT work with non-ionizing radiation for imaging; therefore, the visitors and/or family members are allowed to stay in the room. However, some participants noted that excusing visitors and family members helped reduce the number of questions and cognitive stress they felt. In general, more limited interaction with family and visitors, either due to safety requirements or preference, led to a preference of medical imaging professionals for a larger patient/clinical zone and a smaller family-visitor zone. In Quan et al.’s 37 efforts to publish evidence-based guidelines for hospital room design, they note a lack of knowledge for certain areas of patient room design decision making. Given that standard of care has evolved to a point where imaging is being brought to the patient’s bedside, the configuration of the room, its zones, and room components need to be reevaluated.
Limitations
Onwuegbuzie et al. 21 have noted that focus groups present a unique complexity for analysis and that group dynamics can be quite influential to determining the final outcome. It is for this reason that the data provided in the room design and room design evaluation phases could have been biased; the heterogeneous composition of the focus groups could have influenced the responses from the imaging professionals in those settings. However, the mixed group discussions afforded members of different occupational groups to gain some insight into the challenges faced by fellow staff members, which could be an added benefit to their participation in the study. Given that this was a purposive sample of participants, the results cannot be generalized beyond this cohort. This descriptive research does provide a richer understanding of the issues related to providing imaging examinations at the patient’s bedside.
Conclusions
The participating imaging professionals provided a work-specific set of design suggestions to facilitate their work. To this end, the designation of patient room zones, which are classically used in architectural design 38 , are inadequate to capture this cohort’s need for space to promote proper body posture and position (e.g., clinical zone, patient zone, etc.). Imaging professionals have unique concerns for working in the hospital patient room that stem from their need to have a clinical zone with access to both sides of the patient bed. Mixed methods analysis of data across three phases of this project points to a redefinition of the room zones. The hope is that a better defined work area could minimize the risk of work-related MSK discomfort and promote diagnostic quality. This analysis would suggest that there are significant overlaps between at least some of the “zones” when providing care to patients during imaging. Understanding the space needs for imaging professionals is critical for architects and others who design these workplaces.
Additionally, the entry zone is important to facilitate easy access and egress for imaging equipment. This cohort made it clear that the entry zone needs to be large enough for imaging professionals to easily push their equipment into and out of the hospital room. Without adequate egress, the entry zone could be a design feature that also contributes to the risk for an overexertion injury. A secondary issue was the location of the visitor/family zone which should facilitate the exit of visitors and family members from the room in preparation for a radiographic imaging examination.
We propose a set of Venn diagrams that captures our participants’ desired entry zone, clinical zone, patient zone, and visitor-family zone. The clinical zone for imaging professionals should be considered to be dynamic as it moves and expands for various imaging examinations, significantly overlapping with the patient zone, and then contracting once their work is completed.
Footnotes
Acknowledgements
The research team would like to thank our graduate and undergraduate students who provided hours of work to orchestrate the setup, data collection, and ultimate analysis of this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was funded by CDC-NIOSH R01OH010181 A participatory design process addressing the ergonomics of hospital patient rooms.