
Abstract
Objective:
The objective of this study was to determine the hemodynamic changes in the umbilical artery (UA) and middle cerebral artery (MCA) with oligohydramnios, during third trimester of pregnancy.
Materials and Methods:
A cross-sectional descriptive study was done in a perinatal ultrasound center, over a 9-month period. The participant sample size was 64, and all of the women were conveniently consented and selected for the study. All individuals were referred for obstetrical sonography in the third trimester, with oligohydramnios. All fetal anomalies, such as a neural tube defect, dwarfism, an abdominal wall defect, were excluded from the study.
Results:
The mean systolic to diastolic (S/D) ratio for the UA was 3.01, within a range of 1.49 to 5.60 (± 0.79 SD). The mean pulsatility index (PI), of the UA, was 1.11, within a range of 0.41 to 5.51 cm (± 0.64 SD). The mean resistive index (RI) of the UA was 0.66, within a range of 0.33 to 1.25 cm (± 0.13 SD). The mean S/D ratio of the MCA was 5.68, within a range of 2.05 to 26.10 (± 3.10 SD). The mean PI of the MCA was 1.67 within a range of 0.75 to 2.55 cm (± 0.45 SD). The mean resistive index (RI), of the UA, was 0.82 within a range of 0.51 to 1.77 cm (± 0.82 SD).
Conclusion:
The Doppler indices may rise as pregnancy advances, especially in fetuses with oligohydramnios. In these types of patients, the flow within the MCA may decrease, with an increase in the gestational age. Consequently, it appears that oligohydramnios may lead to vascular remodeling of the UA and MCA.
Amniotic fluid has vital role for proper growth and survival of the fetus, within the uterus. 1 Oligohydramnios (low amniotic fluid) is typically diagnosed with an amniotic fluid index (AFI), below 5 cm. 1 Only lately has the significance of the amniotic fluid content, as a fetal status indicator, been recognized. 2 In fetal development, the amniotic fluid plays a variety of developmental roles. It protects the fetus from injury, is antimicrobial, and helps the gastrointestinal as well as the musculoskeletal systems mature. 2 It aids in the regulation of fetal body temperature, fluid homeostasis, and fetal mobility. Amniotic fluid volume keeps amniotic fluid pressure constant, preventing lung fluid loss, which is crucial for pulmonary development. The fluid also ensures that the umbilical cord is not compressed. 2 A decrease in amniotic fluid content is often one of the earliest signs of a fetal defect or a maternal illness. The 5 cm AFI threshold has been linked to an increased risk of problems in term and near-term pregnancies and includes a small-for-gestational-age (SGA) neonate, a non-reassuring fetal heart rate, stillbirth, and neonatal mortality. 3 Ruptured membranes, congenital anomalies, and placental insufficiency are all common etiological reasons for oligohydramnios. It is thought to be linked to a higher risk of maternal and fetal morbidity. The elevated risk of caesarean births for mothers due to fetal distress, low Apgar scores, and meconium aspiration syndrome, in the fetus, contribute to perinatal morbidity and mortality. 3 Fetal hemodynamics can be assessed noninvasively with ultrasound Doppler. 4 Doppler investigations of the umbilical arteries (UA) offer information about perfusion of the fetoplacental circulation, and specific fetal organs which are valuable in detecting hemodynamic changes occurring in response to fetal hypoxia and anemia. 4 Clinicians must be aware of temporal variations in the fetal circulation. These variations are connected with changes in fetal size as well as other tests of wellness, in order to maximize the Doppler information of the fetal circulation. 5 There have been reported longitudinal data of fetal circulation, using Doppler, but these investigations began after a diagnosis was made of fetal growth restriction or impairment.5-7 To quantify both the UA and middle cerebral artery (MCA), spectral Doppler waveforms (SDW) and Doppler indices, such as resistive indices (RI) and pulsatility indices (PI), have been widely used. When the RI is employed, the SDW is only displayed on a scale of 0 to 1, while some authors use >1, if the end diastolic velocities are missing or inverted. 1 The PI, on the other hand, allows continuous SDW analysis across a wide range of waveform patterns, potentially providing a more accurate analysis, of downstream vascular resistance. 8 When SDW indices are taken, in different segments of the MCA and are analyzed, only the PI shows significant changes. 9 Furthermore, with large data sets employed, reference ranges for cardiopulmonary resuscitation (CPR), using the RI, demonstrate a linear relationship with gestational age (GA).10-13 Normal UA SDW, but abnormal UA and fetal MCA waveforms, are more likely to develop distress and require an emergency caesarean section, with SGA fetuses. The risk of miscarriage is extremely high (86%) when both the uterine and the fetal cerebral waveforms change at the same time, which would indicate that delivery, as soon as fetal maturity is reached, is the optimum alternative. When both vessels have normal waveforms, however, the likelihood of fetal distress is low (4%), and expectant care is the best option. 14 Doppler velocimetry is a non-invasive, quick technique that offers vital information about the fetus’ hemodynamic status, is an effective diagnostic test for fetal peril, and aids in the management of high-risk pregnancies. 15 Early detection and remedial intervention are critical for reducing the perinatal morbidity and fetal mortality, with oligohydramnios. Although a fetus may fail to reach or exceed its projected development potential, this can be caused by a variety of prenatal problems and the most prevalent pathway is uteroplacental insufficiency. 16 The umbilical and intracranial arteries are the most routinely studied vessels in fetuses with oligohydramnios. SDW examination of the UA, particularly the MCA, and the aortic arteries, proves beneficial in predicting fetuses with neonatal wasting, in a sample of high-risk pregnancies. The SDW analysis and clinical result have a substantial relationship. Doppler studies became more widely available, resulting in better obstetric care decisions. 17
According to research, a variety of biophysical approaches are employed for diagnosing and monitoring fetal well-being in intrauterine growth restriction (IUGR) fetuses. Doppler velocimetry has been shown to be the most accurate in identifying and managing IUGR fetuses. The goal of Abdel Aziz et al’s work was to identify the fetal UA and MCA Doppler velocimetry, in detecting IUGR, and to link the Doppler findings with perinatal outcomes. 18 In comparison to the normal group, the aberrant Doppler velocimetry group had a poor overall perinatal outcome. 18 They found that fetal circulation research was useful not only for monitoring growth restricted babies, but also for finding fetal compromises in the early stages of IUGR, as well as determining the best timing for delivery. 18 When compared with infants born with normal growth, oligohydramnios is a sign of an elevated risk of perinatal and long-term death and morbidity. The incidence of oligohydramnios varies significantly among populations. It affects nearly one third of newborns born with a birth weight of less than 2500 grams. 1 Similarly, the incidence of oligohydramnios is dependent on economic growth, with a lower incidence in industrialized countries (4%–8%) than in developing countries (6%–30%). 1 In the general population, oligohydramnios affects about 8% of pregnant women. 1 Oligohydramnios is the result of an aberrant condition in about 35% to 40% of instances. 1 Some of the known risk factors for oligohydramnios include placental insufficiency, maternal hypertension, cardiovascular illness, diabetes, infections, low socioeconomic position, prior history, and preeclampsia. 2 Oligohydramnios has been linked to poor pregnancy outcomes; more than half of stillbirths are due to oligohydramnios, and approximately 10% of neonatal mortality is due to undiscovered oligohydramnios.
According to Malik and Saxena’s research, the prevalence of oligohydramnios in normal term pregnancies in 2002 was 4.4%. 19 The range of prevalence of oligohydramnios was between 4.4% and 8% based on prior published studies.2,19 The systolic to diastolic (S/D) ratio mean value decreases with fetal age and at 20 weeks, the 50th percentile is 4, at 30 weeks, 2.83, and at 40 weeks, 2.18. 20 The average RI value falls from 0.756 to 0.609, while the average PI value falls from 1.270 to 0.967. 20 The typical MCA/UA PI ratio decreases with gestational age, and unusually low MCA/uterine artery PI ratios are linked to poor outcomes. The MCA/uterine artery PI ratio appears to have a predictive value similar to the MCA/UA PI ratio. 21 Doppler indices of the MCA and UA are very helpful in the determination of fetal status, especially in cases of oligohydramnios. But unfortunately, not all perinatal ultrasound clinics are not considering these parameters in practice. Although most of the modern ultrasound equipment systems are equipped with Doppler, it may not utilize, due to either a lack of awareness or knowledge. Doppler indices of the MCA and UA are considered representative of the blood flow in the fetus. The application of Doppler indices in cases of oligohydramnios can help determine the status of the fetus and appropriate clinical management. With oligohydramnios, resistance in the fetal UAs increases, while decreasing in the MCA. Such a hemodynamic remodeling, of these vessels, indicates fetal distress and requires prompt clinical management. The objective of this research was to determine the Doppler indices, in the MCA and UA, for those patients with oligohydramnios, in a specific practice cohort.
Materials and Methods
A cross-sectional descriptive study was done in a Lahore perinatal ultrasound center, over a 9-month period. The participant sample size was 64, and these women were conveniently selected and consented to the study. All individuals referred for obstetrical sonography in the third trimester, with oligohydramnios, were invited to the study. All fetal anomalies, such as a neural tube defect, dwarfism, an abdominal wall defect, were excluded from the study. A Toshiba (Xario prime) ultrasound equipment system was used, with a convex probe (frequency range of 3–6 MHz). All the patients were sonographically examined with an empty bladder, in the supine position or in the right or left oblique position, to detect oligohydramnios. AFI was measured using the deepest vertical pocket of fluid and free of any fetal part or portion of the umbilical cord. The MCA was measured by taking an axial view of the fetal head at the level of the cerebral peduncles. Color Doppler was used to visualize the circle of Willis, and to place the Doppler samples within 1 cm of the MCA’s origin. This was easily identified as a major branch running anterolateral from the circle of Willis, toward the lateral edge of orbit. The PI was calculated, and the results were recorded. 19 The UA was inspected near the placenta insertion site in the free loop of the cord. Color Doppler was used in each case to identify the UA. An SDW was acquired from the free loop of the umbilical cord (UC) with a sample volume of 4 mm. In the event that acquiring the free loop of the UC proved challenging, the placental implantation of the cord was followed, to assist in locating the free loop. The Doppler insonation angle was kept between 0 and 60 degrees. Over three cardiac cycles, the PI and RI were measured manually and automatically. The measurements were repeated, and the study was completed when two consecutive readings yielded the same results. For the purpose of scanning protocol, the American Institute for Ultrasound in Medicine (AIUM) criteria for obstetrical sonography was followed. 20
Results
A total of 64 pregnant females, with oligohydramnios, were included in this cohort study. The mean age of the patients was 33.65, within a range of 27 to 41 years (± 3.67 SD). The mean gestational age was 33.57, within a range of 27 to 39 weeks (± 3.37 SD). The mean expected fetal weight was 2450.54 grams, within a range of 1055.00 to 3686.00 grams (± 758.95 SD). The mean AFI was 4.20, which was within a range of 2.00 to 5.50 cm (± 0.84 SD) (see Table 1).
The Descriptive Statistics Collected on the Cohort of Patients, With Oligohydramnios.

The mean S/D ratio of the UA was 3.01, with a range of 1.49 to 5.60 (± 0.79 SD). The mean PI of the UA was 1.11, which was within a range of 0.41 to 5.51 cm (± 0.64 SD). The RI of the UA was 0.66, which fell within a range of 0.33 to 1.25 cm (± 0.13 SD) (see Figure 1). The mean S/D of the MCA was 5.68 and this was within a range of 2.05 to 26.10 (± 3.10 SD). The mean PI of the MCA was 1.67, which was within a range of 0.75 to 2.55 cm (± 0.45 SD). The mean RI, of the MCA, was 0.82 and was within a range of 0.51 to 1.77 cm (± 0.82 SD) (see Table 2 and Figures 2 and 3).
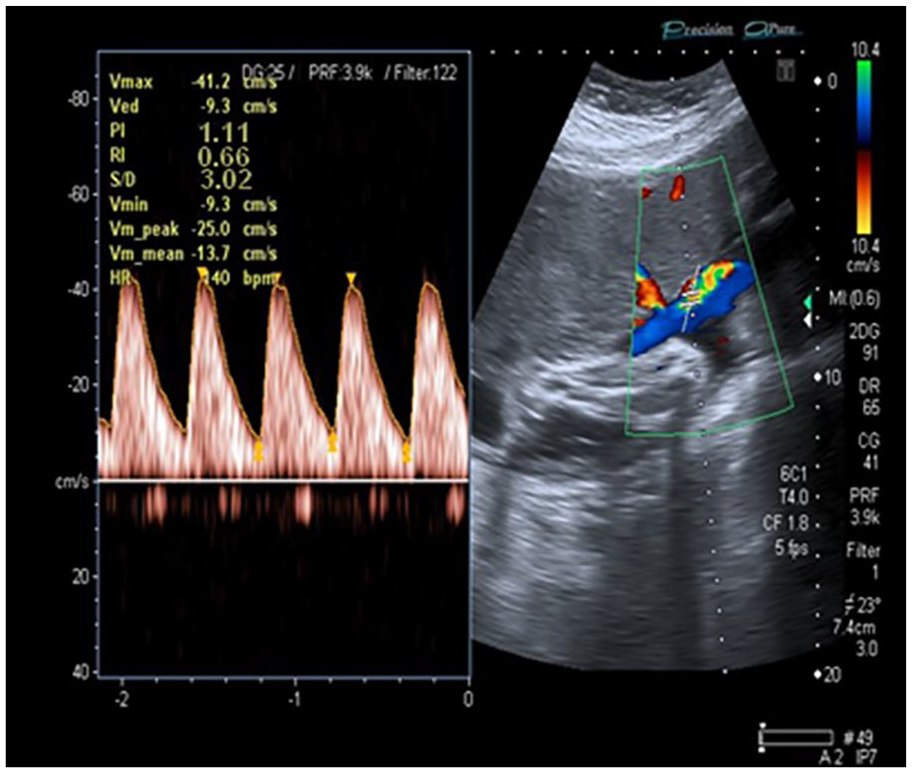
A sample of this umbilical artery segment’s Doppler indices.
The Doppler Indices of Umbilical and Middle Cerebral Artery Recorded From the Fetal Cohort.
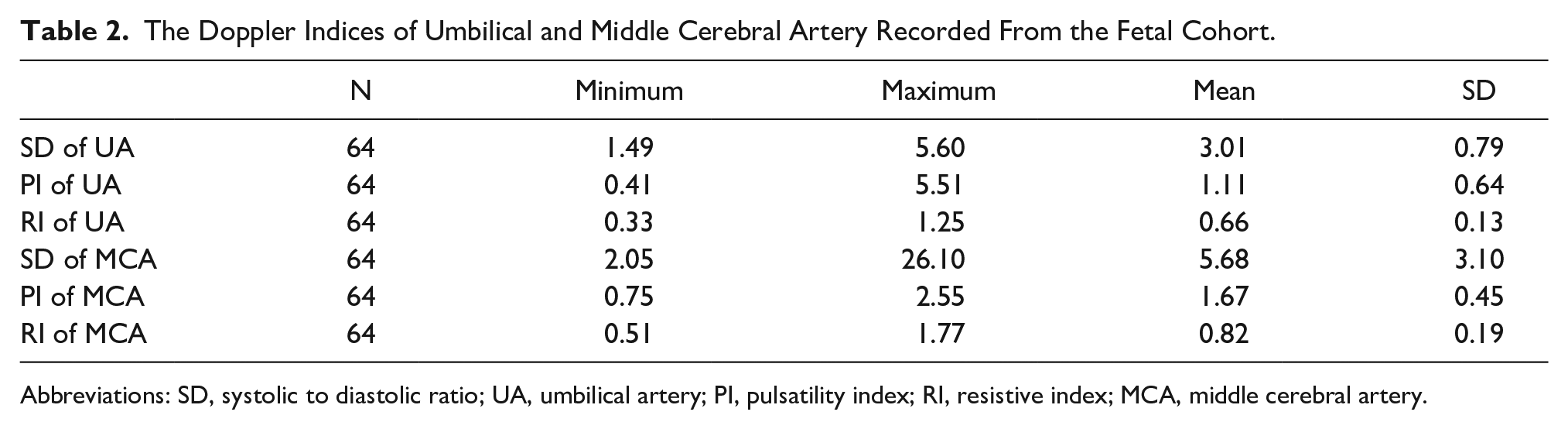
Abbreviations: SD, systolic to diastolic ratio; UA, umbilical artery; PI, pulsatility index; RI, resistive index; MCA, middle cerebral artery.
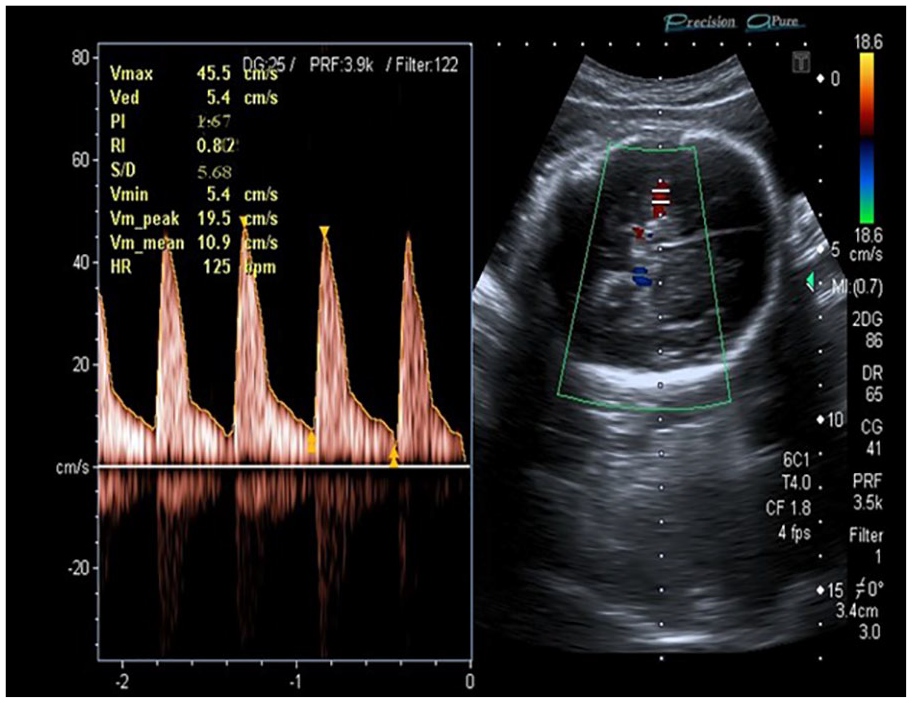
A sample of this middle cerebral artery segment’s Doppler indices.
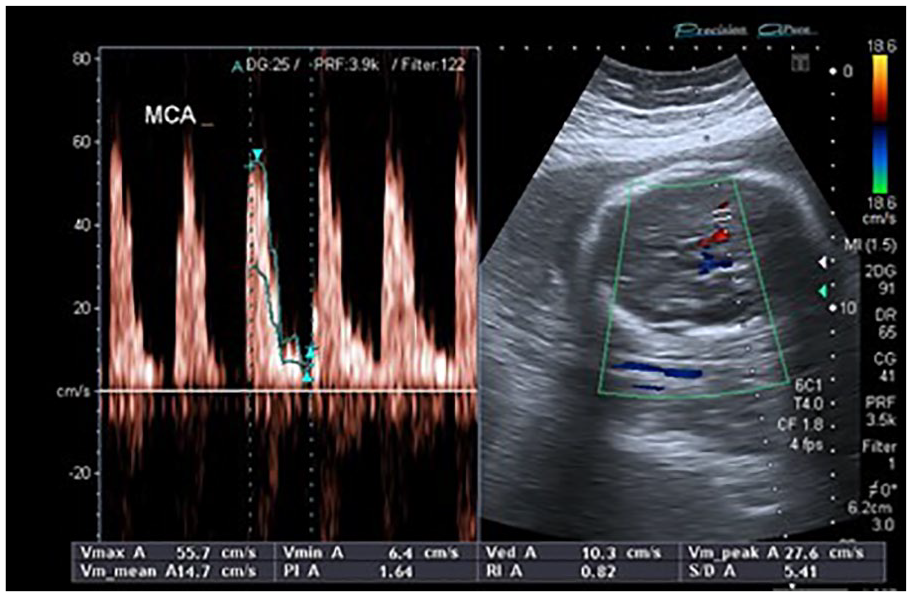
An example of a 0.82 resistive index value, recorded in the middle cerebral artery at 30 weeks, as a result of oligohydramnios.
In the study cohort, sonographic data were taken at the following key gestational ages: At the gestational age of 27 weeks, the mean AFI was 4.30 (± 0.78 SD) and was noted in 3 patients. The mean AFI was 4.03 (± 0.55 SD) at 28 weeks in 3 patients. The mean AFI was 4.14 (± 1.01 SD), at 29 weeks, in 5 patients. The mean AFI was 4.30 (± 1.00 SD) at 30 weeks in 4 patients. The mean AFI was 4.04 (± 1.22 SD) at 31 weeks in 5 patients. The mean AFI was 3.58 (± 0.84 SD) at 32 weeks in 5 patients. The mean AFI was 3.58 (± 0.77 SD) at 33 weeks in 6 patients. The mean AFI was 4.54 (± 0.91 SD) at 34 weeks in 5 patients. The mean AFI was 3.85 (± 0.85 SD) at 35 weeks in 4 patients. The mean AFI was 4.72 (± 0.42 SD) at 36 weeks in 5 patients. The mean AFI was 4.52 (± 0.79 SD) at 37 weeks in 9 patients. The mean AFI was 4.65 (± 0.51 SD) at 38 weeks in 4 patients. The mean AFI was 4.30 (± 0.91 SD) at 39 weeks in 5 patients.
Discussion
Amniotic fluid volume depends on many parameters, such as fetal urine production, uteroplacental perfusion, and maternal hydration. 21 The purpose of this study was to determine the hemodynamic changes in the UA and MCA, with oligohydramnios, in third trimester of pregnancy. Manning et al looked at a large, pre-screened group of patients and discovered that oligohydramnios was a highly accurate predictor for these complications. 22 Philipson et al, conversely, wanted to see how useful sonographically determined oligohydramnios would be in a more clinical environment.19,23 Since the application of ultrasound Doppler, in obstetrics, the UA has become the first and most studied fetal artery. In Tannirandorn and Phaosavasdi’s work, the absence of diastolic flow was often linked to negative pregnancy outcomes, such as oligohydramnios and fetal hypoxia.19,24 Yoshimura et al discovered a connection between the MCA/UA pulsatility index ratio and the HC (Head Circumference)/AC (Abdominal Circumference) ratio. 25 They also discovered a clear connection between the MCA/UA PI ratio and birth weight. Banu recently tested the RI and PI in the UA and MCA, as well as the RI and PI ratios between the two arteries. 26 The researchers found that although measuring the PI value in the UA is sufficient to detect IUGR per se (due to a decrease in placental vascular bed), the ratio of indices between the UA and MCA is more reliable than independent evaluations in identifying fetuses in distress (due to a brain sparing effect as well as fetoplacental insufficiency). 19 The aim of Carroll’s published work was to determine the function of the UA Doppler velocimetry, in the management of oligohydramnios. Pregnancies with oligohydramnios were detected using UA Doppler velocimetry. Patients who had ruptured membranes or had complex congenital abnormalities were not included in the study. 27 The remaining measures of perinatal morbidity were associated with reported S/D ratio values, including delivery of a small-for-gestational-age baby, preterm delivery, hyperbilirubinemia, need for blood transfusion, and other cardiovascular or pulmonary complications. 28 Seventy-six subjects were selected for research based on the findings. Sixty-six had usual S/D ratios, with 17 (37%) of them being linked to perinatal morbidity. Morbidity occurred in five patients after prematurity due to delivery for the sole reason of oligohydramnios was ruled out (11%).29,30 In contrast, 80% of the 30 patients with irregular Doppler indices had a negative outcome. 31 Pregnancies with oligohydramnios and normal UA Doppler velocimetry were found to be substantially (P < .001) less likely than those with abnormal Doppler indices to have an abnormal perinatal outcome. 32 Oligohydramnios and a regular UA Doppler velocimetry have been shown to reduce iatrogenic morbidity due to prematurity by up to 26%. 33 Selam et al conducted another study with the aim of comparing fetal arterial and venous Doppler parameters in post-term pregnancies with oligohydramnios to those with normal amniotic fluid. 23 Cross-sectional research was conducted in 38 pregnancies, with a gestational age of more than 41 weeks. The PI for the fetal MCA, renal artery, UA, IVC (Inferior venacave), and ductus venosus was determined using pulsed Doppler. According to the findings, oligohydramnios was found in ten cases, while a typical AFI was found in 28. 23 The PI of the MCA was reduced in oligohydramnios. The UA PI ratio was found to be abnormally high. 23 Finally, oligohydramnios in post-term pregnancies is linked to arterial redistribution of fetal blood flow, indicating a brain sparing effect, as well as decreased MCA resistance and increased fetal UA resistance. 34 The average age of the pregnant women in our sample was 33.67 years. In that cohort, the average gestational period was 33.57 weeks. The estimated fetal weight was 2450.54 grams, and the average AFI was 4.20 centimeters. 23
According to international studies, Doppler indices, in the umbilical artery, decreases with increasing GA. 35 However, in the present study, the Doppler indices increased with an increase in GA, for fetuses with oligohydramnios. Conversely, according to international studies, the Doppler indices in the MCA decrease with an increase in the GA. 36 In the present study, it was noted that Doppler indices also increased, in this cohort. Consequently, oligohydramnios may lead to a vascular remodeling of the UA and MCA.
Limitations
This is a cohort study; therefore, the results are confined to these patients and cannot be generalized to the population. The study design and convenient sample result in threats to internal and external validity.
Conclusion
The results of this cohort study demonstrate that the Doppler indices taken increased with increasing in GA, in patients with oligohydramnios. Alternatively, in the MCA Doppler indices decreased with increasing GA. Consequently, this pre-experimental cohort study would indicate that oligohydramnios may contribute to the vascular remodeling of the UA and MCA. Further research studies are needed with stronger designs and larger sample sizes to provide stronger evidence.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.