
Abstract
Pregnant patients with sickle cell anemia (HbSS) are at risk of adverse outcomes to the mother and the fetus due to unique pathophysiologic changes. The purpose of this study was to determine the umbilical artery (UA) Doppler indices at 26 weeks gestational age (GA) in HbSS women with uncomplicated pregnancies and compare with the obstetric outcome. In this cohort study, 60 HbSS and 60 normal hemoglobin (HbAA) women with uncomplicated pregnancies were recruited from the antenatal clinic and prospectively followed to delivery. UA velocimetry, fetal biometry, maternal hematocrit, and parity were assessed at 26 weeks. Fetomaternal outcomes were also documented. UA Doppler indices and estimated fetal weights were comparable to those of HbAA control subjects at 26 weeks GA. There was a statistically significant increase in adverse obstetric outcomes in HbSS patients. There was no correlation between maternal hematocrit and artery indices. Further research is required to determine cutoff values and optimal timing for sonography in HbSS patients.
Sickle cell disease (SCD) and its variants are genetic disorders resulting from the presence of a mutated form of hemoglobin, hemoglobin S (HbS). 1 The prototype of these diseases is sickle cell anemia, an autosomal recessive disorder, which results from point mutation and leads to substitution of valine for glutamic acid, at the sixth position of the beta-globin chain. The resultant hemoglobin molecule has abnormal physiochemical properties that lead to the manifestation of the chronic disease state. 2
SCD affects 20 to 25 million people globally. 3 The exact prevalence is unknown in the United States, 4 but a study by Brousseau et al. 5 on the number of people with SCD in the United States showed 89,079 people in 2005. Prevalence in India varies per tribe from 1% to 40%, with Madhya Pradesh having the highest load with an estimated number of 961,492 heterozygotes and 67,861 homozygotes. 6 In Nigeria, by far the most populous country in sub-Saharan Africa, 24% of the population are carriers of the mutant gene, and the prevalence of sickle cell anemia is 20 per 1000 births. 3 This would indicate that in Nigeria alone, 150,000 children are born with sickle cell anemia every year. 7
The pathophysiology of sickle cell anemia is based on the distortion of red blood cells when these circulate through areas of low oxygen tension. With time, the cells become irreversibly sickled and are either removed from circulation by the reticuloendothelial system or occlude small capillary beds, which can lead to an infarctive crisis. 2
During normal pregnancy, various physiological changes occur, including changes in the hemodynamic status of the patient. Plasma volume increases by 10% to 15% at 6 to 12 weeks of gestation and expands rapidly until 30 to 34 weeks, after which there is only a modest rise.8–11 The total gain at term averages 1100 to 1600 mL and results in a plasma volume of 4700 to 5200 mL, with 30% to 50% above that found in nonpregnant women. 12 This results in physiological anemia during pregnancy, and in women who already have baseline anemia, the condition is exaggerated.
Advances in medical and obstetric care have led to a continuous improvement in outcome for pregnant women with sickle cell anemia, but complication rates and mortality remain significantly increased compared with normal hemoglobin (HbAA) pregnancies. 13 Complications of sickle cell anemia can be classified into maternal and fetal. Maternal complications include pre- and postpartum painful crises, placental thrombosis, urinary tract infections, and pneumonia. Fetal complications are preterm delivery, growth restriction, stillbirth, and miscarriage. Of these, the most common fetal complication is growth restriction. 14
Intrauterine growth restriction (IUGR) refers to a rate of growth of a fetus that is less than normal for its growth potential at that particular gestational age (GA). 15 A growth-restricted fetus is one whose estimated weight is below the 10th percentile for its GA and whose abdominal circumference is below the 2.5th percentile. 16 Intrauterine growth restriction is further classified into early and late-onset IUGR, with these two groups having different clinical, biochemical, and histological features. 17 Early onset IUGR occurs before 32 weeks GA 18 and is associated with abnormal umbilical artery Doppler indices and preeclampsia. Late-onset IUGR is associated with fewer changes in the umbilical artery flow pattern. 19
The severity of growth restriction is important as such fetuses have a 5- to 10-fold risk of dying in utero. 20 Length of growth deficit is also associated with worsening perinatal morbidity. 7 Antenatal detection of growth-restricted fetuses has also been found to significantly improve outcome. 21
Fetal circulation consists of parallel blood flow pathways and two shunts. 22 The fetus receives nutrient-rich blood from the placenta through the umbilical vein, while fetal blood is transferred via two umbilical arteries to the placenta. During pregnancy, blood flow increases in the low-impedance uteroplacental circulation, reaching 500 mL/min at term. 23 Placental flow increases until 25 weeks’ gestation and then remains unchanged. 24 It has been found that most cases of growth restriction correlate with placental insufficiency. 25
Doppler sonography provides a noninvasive method of assessing blood flow within the fetoplacental circulation and is considered a gold standard in the assessment of fetal hemodynamics. Placental function evaluation by umbilical artery Doppler is a clinical standard used to distinguish between small for GA and IUGR.26–28 Abnormal waveforms (principally the loss of forward end-diastolic flow velocity) in the umbilical arteries of many pregnancies can be complicated by either preeclampsia or severe IUGR and provides an important insight into their pathophysiology. 22
Doppler sonography also plays a fundamental role in the diagnosis of IUGR and also has the potential to determine the timing of deliveries of some growth-restricted fetuses. Doppler sonography of the umbilical artery and middle cerebral artery, in combination with biometry, provides the best tool to identify small fetuses at risk for adverse outcomes. 29 Various studies have demonstrated its usefulness in improving obstetric outcome. 30 Resistive index (RI), also known as Pourcelot’s index, is a measure of resistance to blood flow caused by the microvascular bed distal to the site of measurement. 31 Studies have also shown that vascular compliance also has an effect on RI. 32
Anyaegbulam et al. 33 prospectively studied the uterine and umbilical artery Doppler velocimetry of women with homozygous SCD in their third trimester; they noted that the incidence of abnormal peak systolic velocity to end-diastolic ratios (S/D) for the umbilical artery was significantly higher in pregnant women with sickle cell anemia compared with sickle cell trait (HbAS) and HbAA patients. Hwang et al. 34 also showed that Doppler sonography can also be used as a predictor of adverse pregnancy outcomes in women with anemia during the third trimester.
The aim of this study was to assess umbilical artery Doppler findings in women with sickle cell anemia in the local environment at the onset of the third trimester. This has the potential to assist in health care delivery, the timely management of pregnant women with SCD, and improved fetomaternal outcomes.
Methods and Material
Study Design
This was a cohort study of pregnant women with sickle cell anemia and homozygous normal hemoglobin patients referred from and registered for antenatal care at the Obstetrics and Gynecology Department of a teaching hospital. Differences in umbilical artery indices and fetomaternal characteristics were analyzed. Recruitment into the study was carried out over a period of 18 months, from January 2014 to June 2015. Ethical consideration was obtained from the Lagos University Teaching Hospital (LUTH) Health Research and Ethics Committee prior to the study’s commencement.
Sample Size
Sample size was derived using the formula designed to calculate the sample size for study comparing means of a variable in two populations. 35
where
n = sample size of each group,
u = one-sided percentage point of the normal distribution corresponding to 100% power (the power of this study was 90%),
v = percentage point of the normal distribution corresponding to a two-sided significance level,
u1 = expected mean (hypothetic mean): mean birthweight in healthy newborns is 3.0 kg, 36 and
u0 = universal mean = mean birth weight seen in the literature in sickle cell pregnancies. 37
Universal mean (u0) from the literature 38 is 2.6 ± 0.6. Thus, the expected subject mean (u1) is 3.0 ± 0.79. At 90% power, u = 1.28. At a significance level of 5%, v = 1.96.
This was rounded down to 60. A control group of 60 HbAA pregnant women was also consecutively recruited following informed consent, giving a total of 120 participants. The study and control groups were matched for GA using a combination of early dating scans and last menstrual period. Results were also disclosed to the managing obstetrician(s).
Inclusion criteria comprised pregnant women with sickle cell anemia (HbSS) as the test group and pregnant women with HbAA as the control group. These pregnant women had singleton gestations and were regular attendees at the antenatal clinic.
Exclusion criteria were pregnant patients with other hemoglobinopathies (e.g., hemoglobin SC genotype, as well as Sβ-thalassemia), sickle cell trait (HbAS), hypertension, twin gestation, sonography-confirmed congenital abnormalities, and diabetes.
Obstetric Sonography and Umbilical Artery Doppler Technique
The procedure was explained to the participants and consent obtained before recruitment into the study. All sonographic examinations were performed by the researcher (a senior resident) under the supervision of a board-certified consultant radiologist using the standard Doppler sonography procedure in the institution. Real-time ultrasound equipment (Toshiba Nemio XG Diagnostic Ultrasound System; Toshiba, Tochigi ken, Japan), equipped with vascular software for 2D imaging, color, spectral Doppler, and a convex 3.5-MHz curvilinear transducer, was used for imaging. A high-quality monitor on the ultrasound equipment was used during acquisition of the images.
Recruited patients were scanned on one occasion during the 26-week GA period. GA was confirmed with a combination of last menstrual period and early dating sonograms. For those consented patients who were encountered prior to 26 weeks GA, they were followed up via antenatal clinic appointments and enrolled at the end of the second trimester.
B-mode sonography was employed in identifying the fetus and measuring the biometric parameters (biparietal diameter, head circumference, abdominal circumference, and femur length) to determine the GA of the fetus. These values were recorded and plotted on percentile charts according to gestational age and Hadlock’s sonographic weight standard. M-mode scanning was used to measure the fetal heart rate and assess for fetal cardiac rhythm. 39 Normal fetal heart rate was set between 120 and 180 beats per minute. Also in B-mode sonography, a free-floating loop of umbilical cord was identified and color Doppler employed in identifying the cord and composite vessels of two arteries and a vein. Continuous-wave Doppler was then employed with the sample box placed over the umbilical artery (Figure 1). The sample size was collimated to reduce margin of error from interference. Machine-automated measurements of Doppler indices were obtained, repeated three times, and recorded.
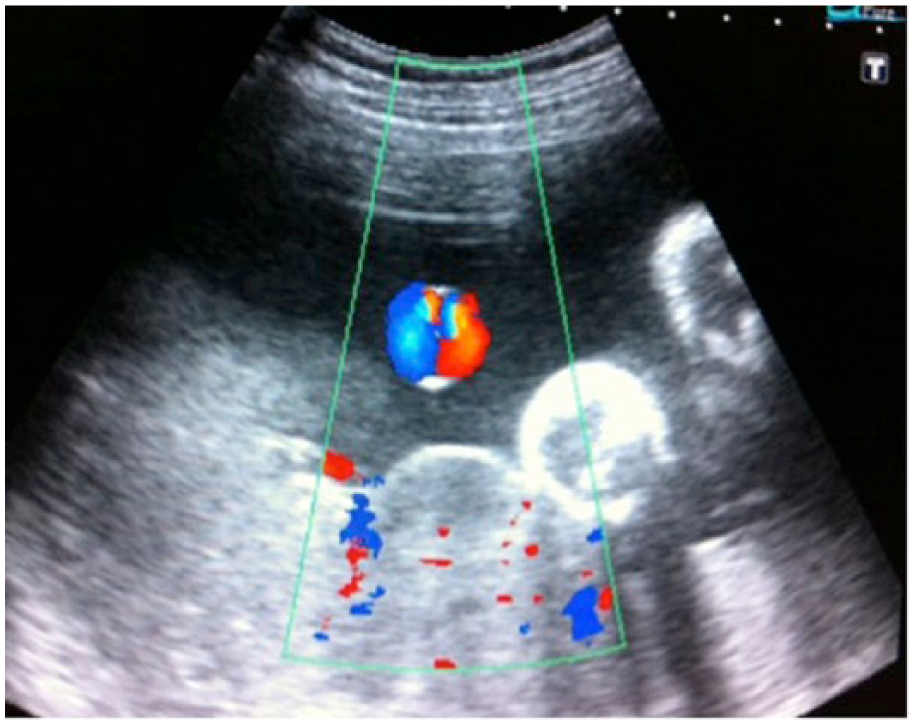
Color doppler of the umbilical artery.
Through observation of the fetal thorax, the umbilical artery velocimetry was carried out during periods of fetal apnea. 39 When four to five waves of equal heights were seen, the image was frozen and measurements were taken using the caliper feature and tracing through a peak and a trough, which represented a cardiac cycle. The computer-generated indices were obtained directly from the ultrasound equipment monitor and recorded. This was repeated three times at the same point and the average value taken, so as to reduce operator-dependent error. Parameters studied included the S/D ratio and RI of the umbilical artery, as well as the presence of absent and reversed diastolic flow. The flow velocities were considered abnormal if the S/D ratio and RI exceeded the 95th percentile 40 and if there was absent or reversed end-diastolic flow velocity in the umbilical artery.
The patients were prospectively followed up throughout the pregnancy until delivery and the details of pregnancy events, labor, delivery, and neonatal outcomes were recorded. Other maternal prepregnancy medical conditions (e.g., history of renal impairment) were noted. Abnormal fetal outcomes considered were intrauterine demise, intrauterine growth restriction, 5-minute Apgar score less than 6, and abnormal birth weight. IUGR was defined in this study as estimated fetal weight below the 10th percentile for gestational age and abdominal circumference below the 10th percentile for gestational age. The prevalence of IUGR was calculated using the following formula:
Statistical Analysis
The data collected were analyzed using sensitivity and specificity. Predictive value (P value) was set at .05 a priori. Data analysis was done using Statistical Package for Social Science (SPSS) for Windows version 20.0.1 (SPSS, Inc., an IBM Company, Chicago, IL) and Microsoft Excel for Windows (Microsoft, Redmond, CA). The location and spread of continuous variables such as means were done using the independent (Student) t test. Hypothesis testing for comparison between groups of categorical data or proportions was done using the χ2 or Fisher exact test where the assumptions of the χ2 were not met. Associations between continuous variables were done using Pearson’s correlation. Receiver operator characteristic (ROC) curve was plotted for the sensitivity and specificity noted for the detection of intrauterine growth restriction using RI and S/D. Umbilical artery Doppler findings were grouped into categories, including absent diastolic flow, reversed diastolic flow, RI >95th percentile, and S/D greater than 95th percentile. The results were also presented in a tabular format. The frequency of pathologies seen was calculated and compared with those from other studies. From this analysis, conclusions were deduced from the patterns of umbilical arterial Doppler findings, pregnancy outcomes, and hemodynamic status of the patients.
Results
In total, 120 pregnant women (60 HbSS and 60 HbAA), aged between 23 and 34 years with gestational ages between 26 weeks, 0 days and 26 weeks, 6 days, were examined during the duration of this comparative prospective study.
The sociodemographic distribution of the study and control populations is presented in Table 1. The mean maternal age was 27.70 ± 3.38 years in the control group and 28.50 ± 2.89 years in the study group. The largest number of subjects for both populations was in the 26- to 30-year age bracket, making 46.7% of the total study population. In the study population, 76.7% of sickle cell anemia patients had received some tertiary education, compared with 80% of the control group.
Sociodemographic Characteristics of the Population.
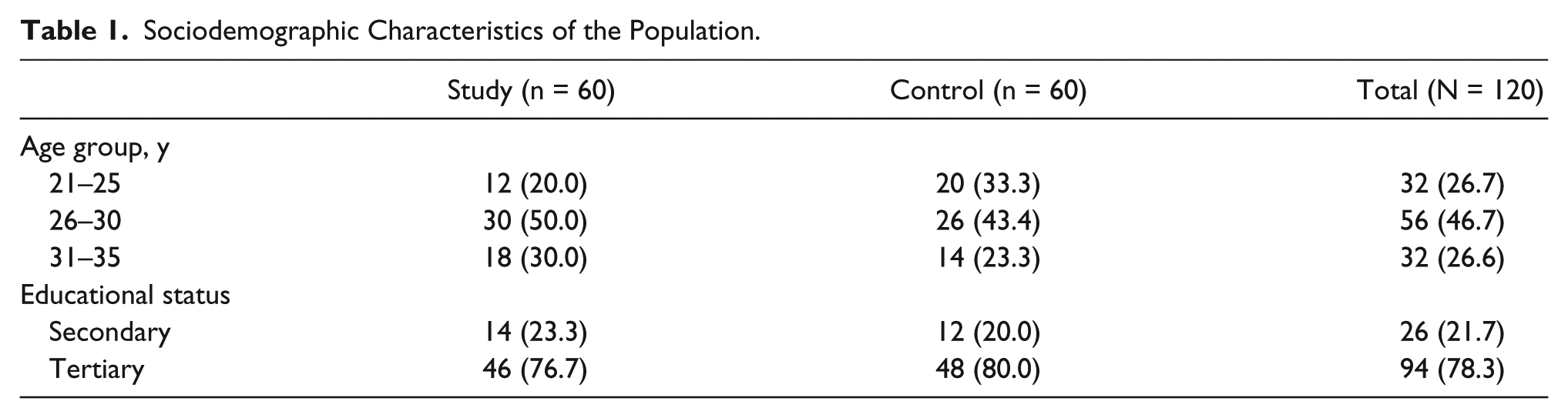
Table 2 demonstrates the mean maternal characteristics (parity and packed cell volume [PCV] of the study and control patients) and 26-week umbilical artery indices in both populations. Parity was significantly lower in the 21- to 25-year and 26- to 30-year age groups (P = .014 and .002, respectively) of the sickle cell anemia patients. There was a statistically significant difference in hematocrit levels between the study and control groups. The mean umbilical artery index distribution (RI and S/D) of the HbSS patients at 26 weeks GA was not significantly different compared with the HbAA patients in the same age group (P > .05).
Maternal Characteristics With Umbilical Artery Velocimetry in Each Age Group.
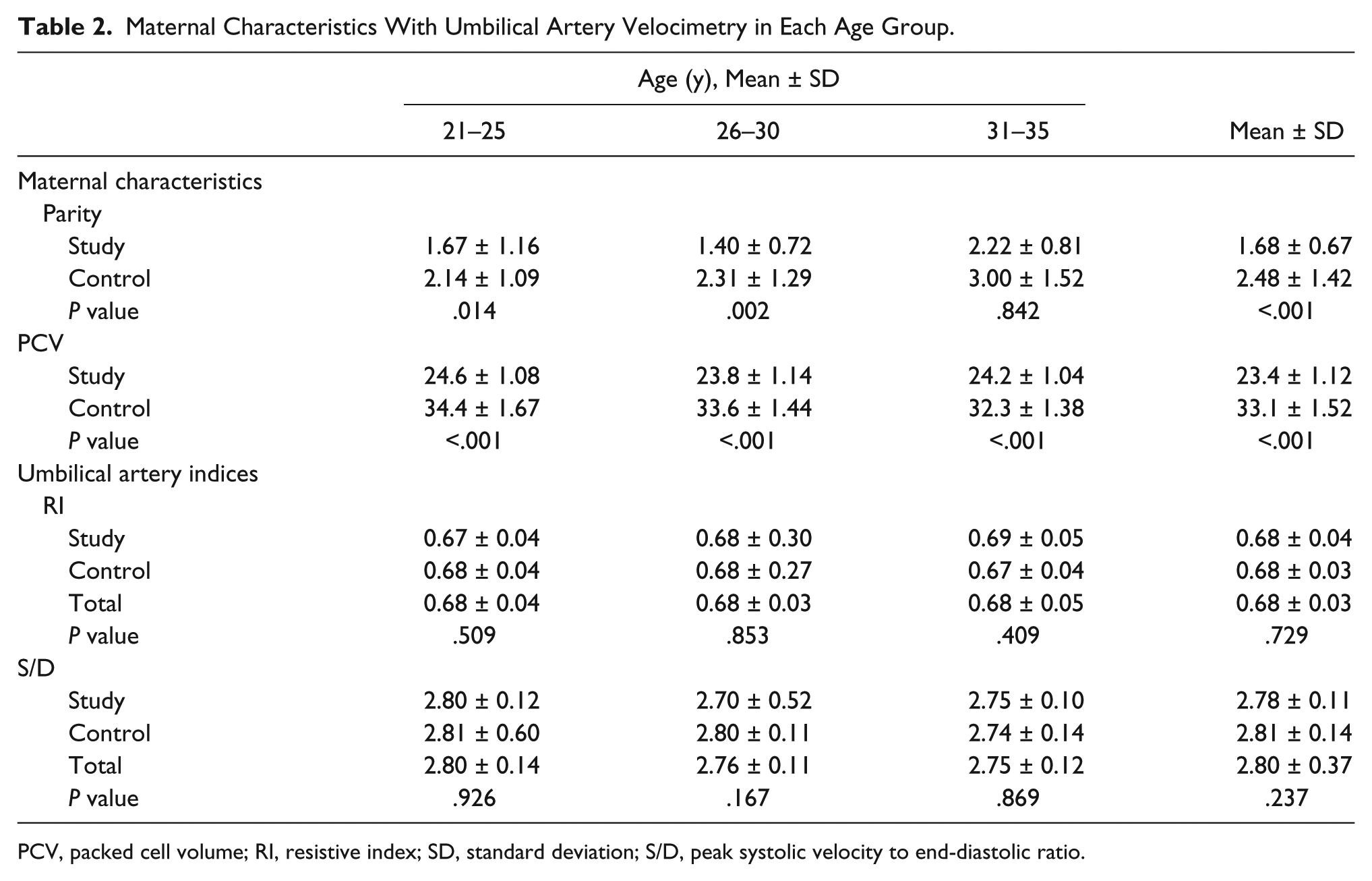
PCV, packed cell volume; RI, resistive index; SD, standard deviation; S/D, peak systolic velocity to end-diastolic ratio.
Correlation studies are shown in Table 3. There was a negligible correlation between umbilical artery indices and parity in both study and control groups. A strong negative relationship was seen between maternal hematocrit and RI (r = −0.449, P = .013) in the 26- to 30-year age group of HbSS patients. Negligible or weak correlation was noted in the 21- to 25-year and 31- to 35-year age groups. Correlations with S/D and hematocrit showed a weak to strongly positive relationship. However, these correlations did prove to be statistically significant.
Correlation Studies of RI, PI With Parity, and PCV.
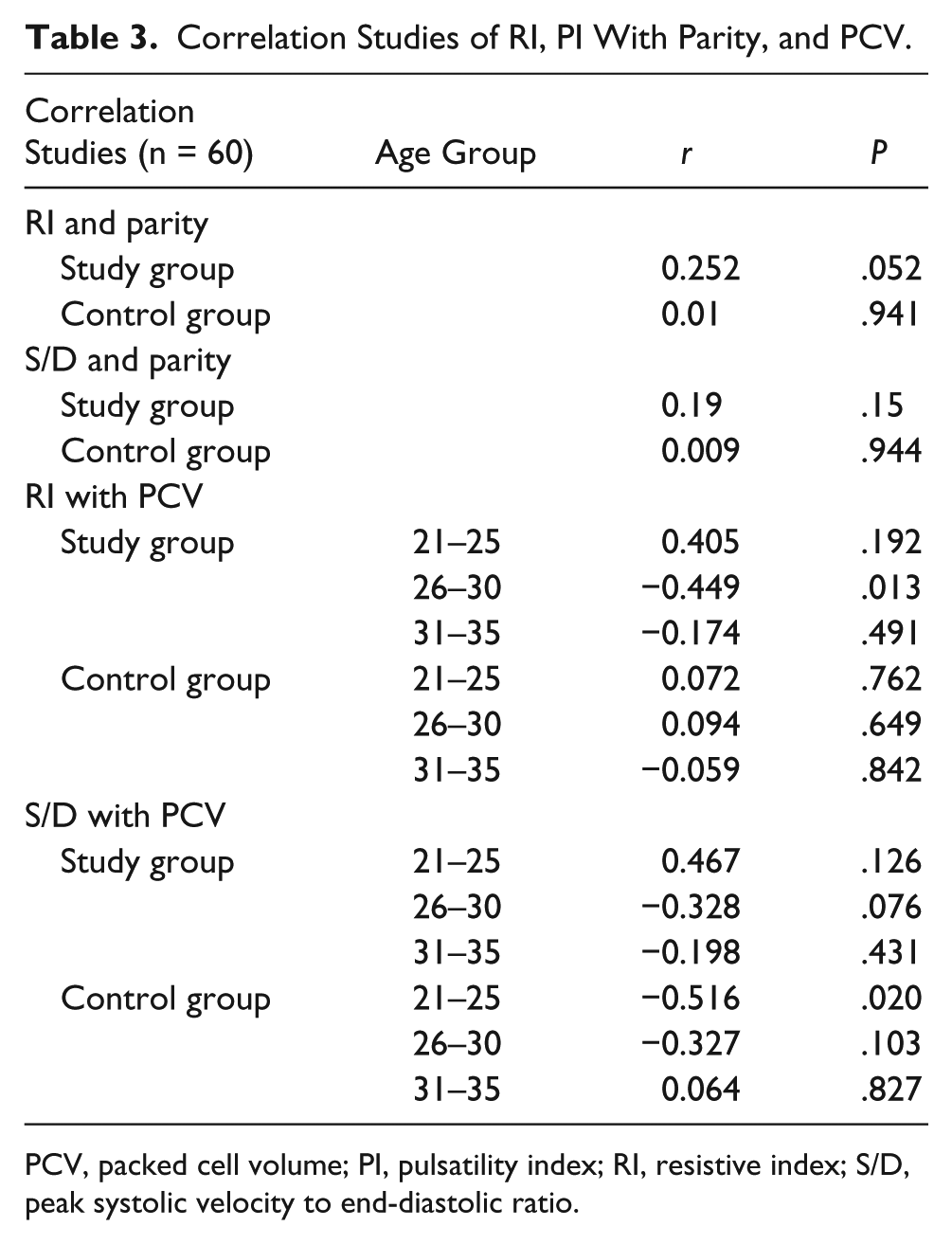
PCV, packed cell volume; PI, pulsatility index; RI, resistive index; S/D, peak systolic velocity to end-diastolic ratio.
In Figure 2, estimated fetal weight is shown graphically in both the study (HbSS) and control (HbAA) populations. Estimated fetal weights were comparable in both groups, and there was no fetus with an IUGR at 26 weeks’ gestation, using the diagnostic criteria.
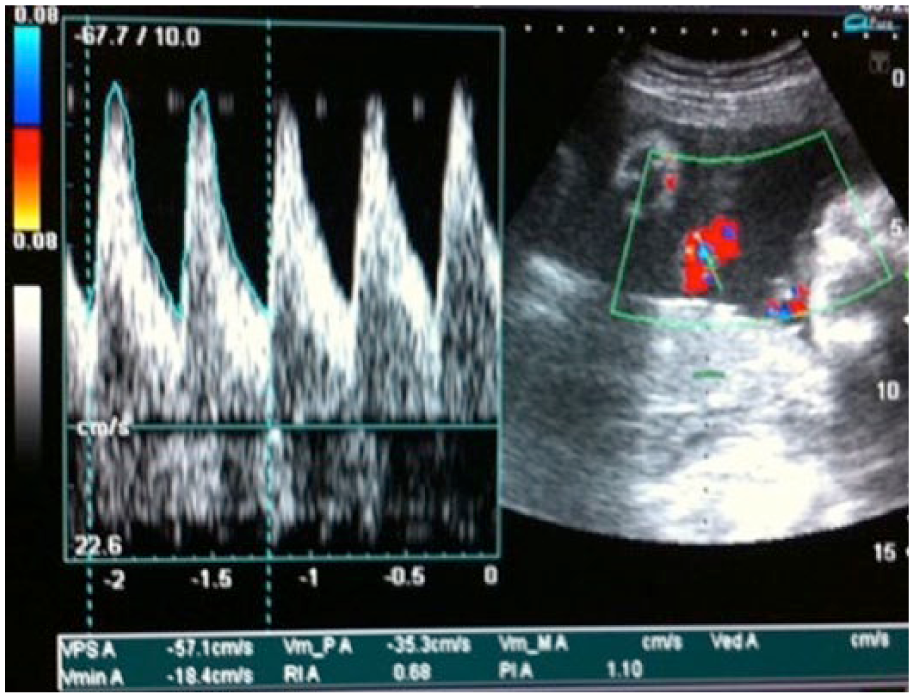
Triplex Doppler velocitometry of a free-floating umbilical cord.
Perinatal outcomes were poorer in HbSS pregnancies, with intrauterine fetal demise noted in 3% (P = .042), IUGR seen in 16.7% (P = .011), and low birth weight in 63% (P = .021) of the patients (see Table 4).
Perinatal Outcome in Study Population.
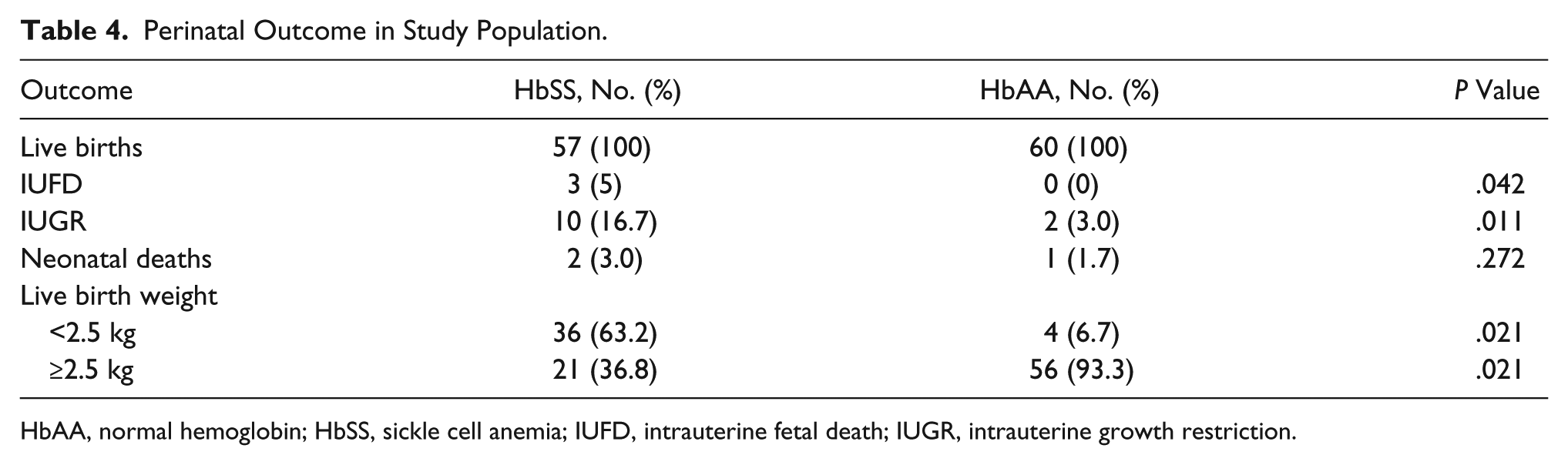
HbAA, normal hemoglobin; HbSS, sickle cell anemia; IUFD, intrauterine fetal death; IUGR, intrauterine growth restriction.
Table 5 shows that the mean birth weight was significantly higher in HbAA pregnancies in all age groups (P < .001). Apgar scores at 5 minutes were, however, marginally lower in the HbSS group compared with the HbAA group in the three age brackets. These were, however, not significant (P > .05).
Mean Fetal Birth Weight and Apgar 5 in Study.
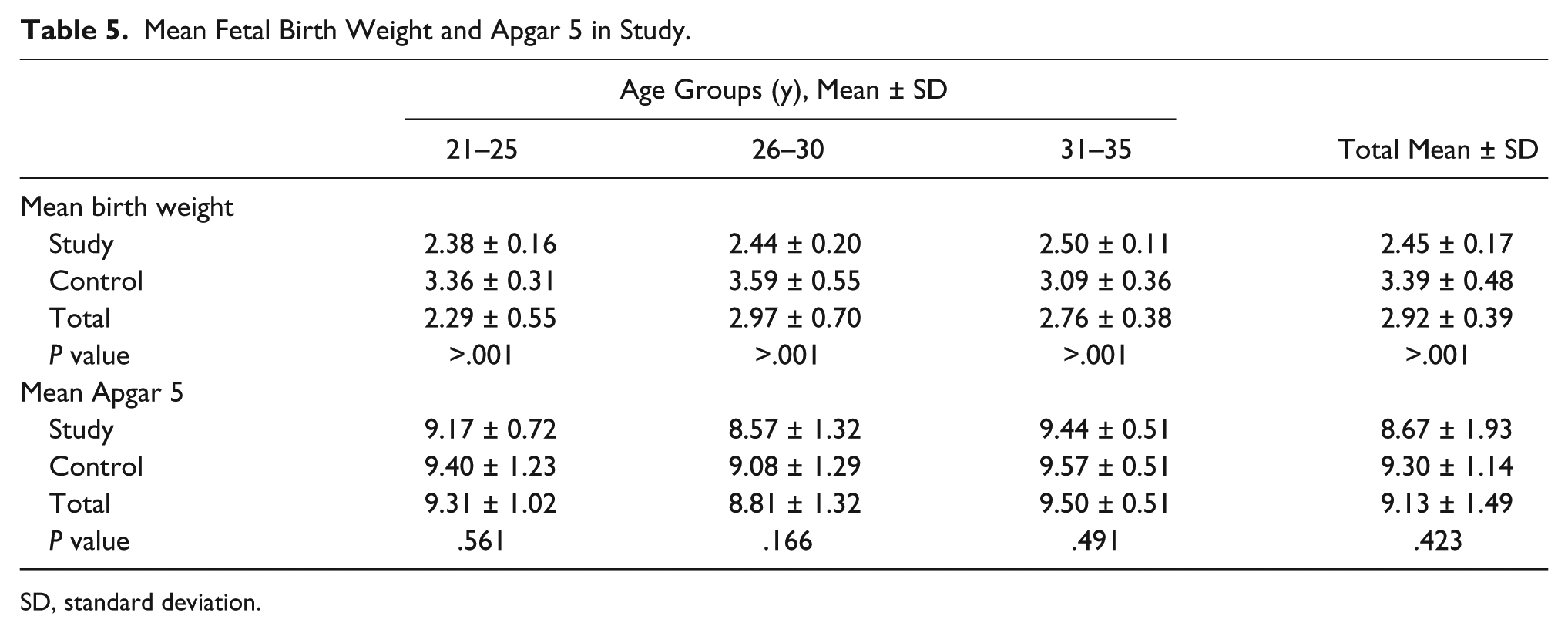
SD, standard deviation.
There was high incidence of operative delivery in HbSS pregnancies, with 73.3% of these patients undergoing caesarean section (elective and emergency), compared with 30% of HBAA pregnancies (see Figure 3).
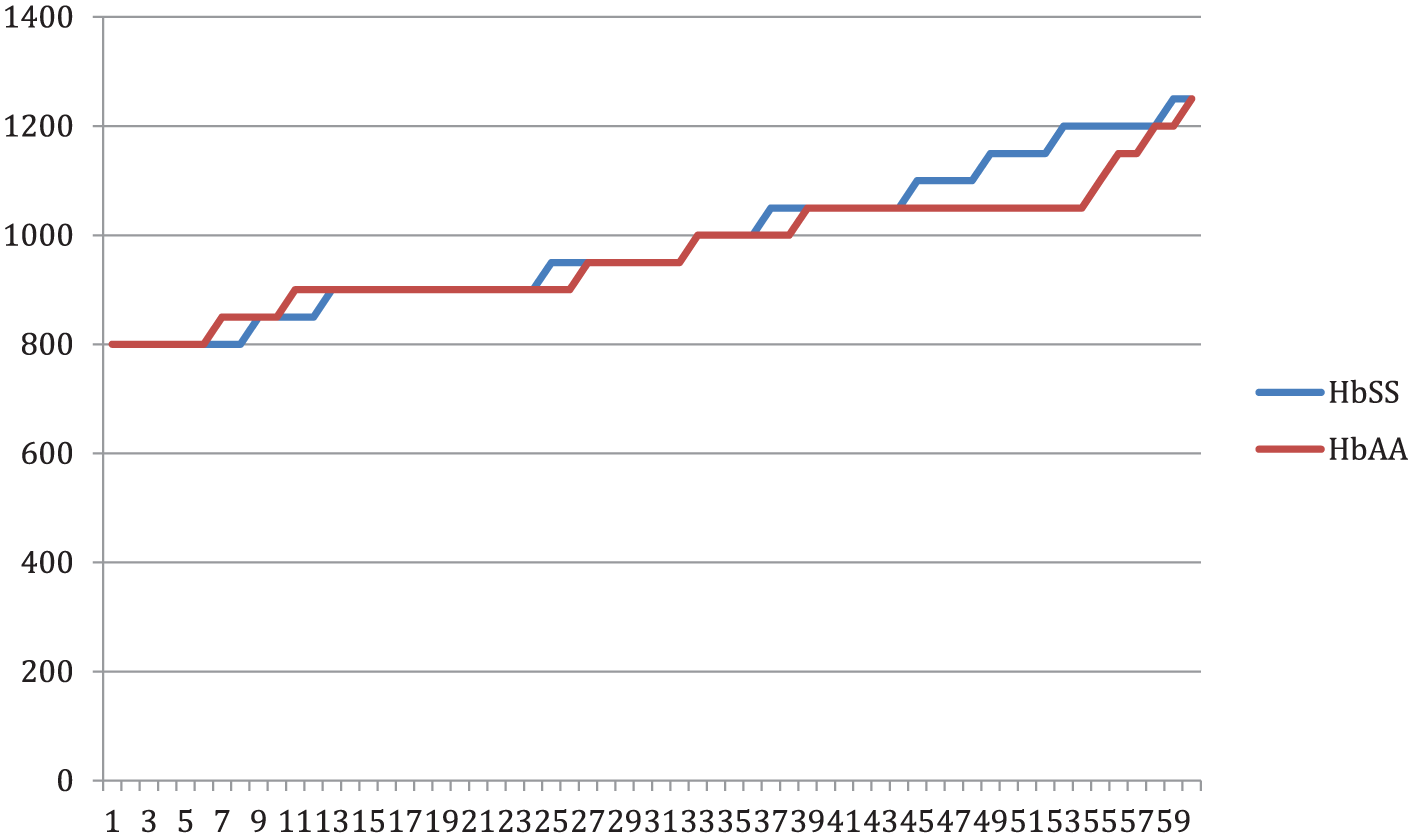
Estimated fetal weight at 26 weeks gestational age in the study population. HbAA, normal hemoglobin; HbSS, sickle cell anemia.
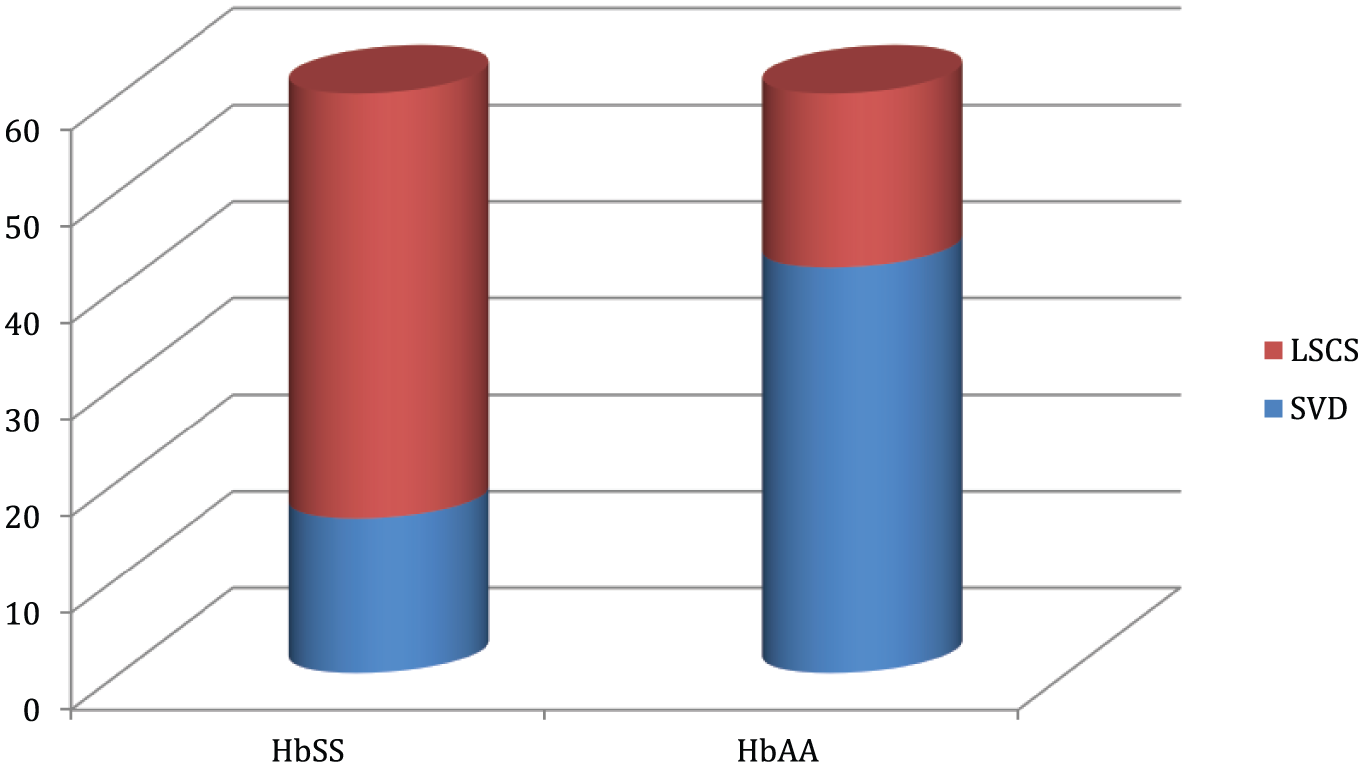
Frequency of operative delivery in study population. LSCS, lower segment cesarean section; SVD, spontaneous vaginal delivery.
In a multivariate correlation between birth weight, umbilical artery Doppler indices, and maternal hematocrit, birth weight showed a strong positive relationship with RI in the 21- to 25-year age group of HbSS patients (r = 0.638; P = .026) and a nonsignificant inverse relationship in the 26-to 30-year and 31- to 35-year age bracket (see Table 6). There was a weak inverse relationship between birth weight and S/D ratio in the 26- to 30-year and 31- to 35-year age bracket and a moderate positive correlation in the 21- to 25-year age bracket. These were, however, not statistically significant (P > .05).
Correlation of Birth Weight with Umbilical Artery Indices and Maternal Hematocrit.
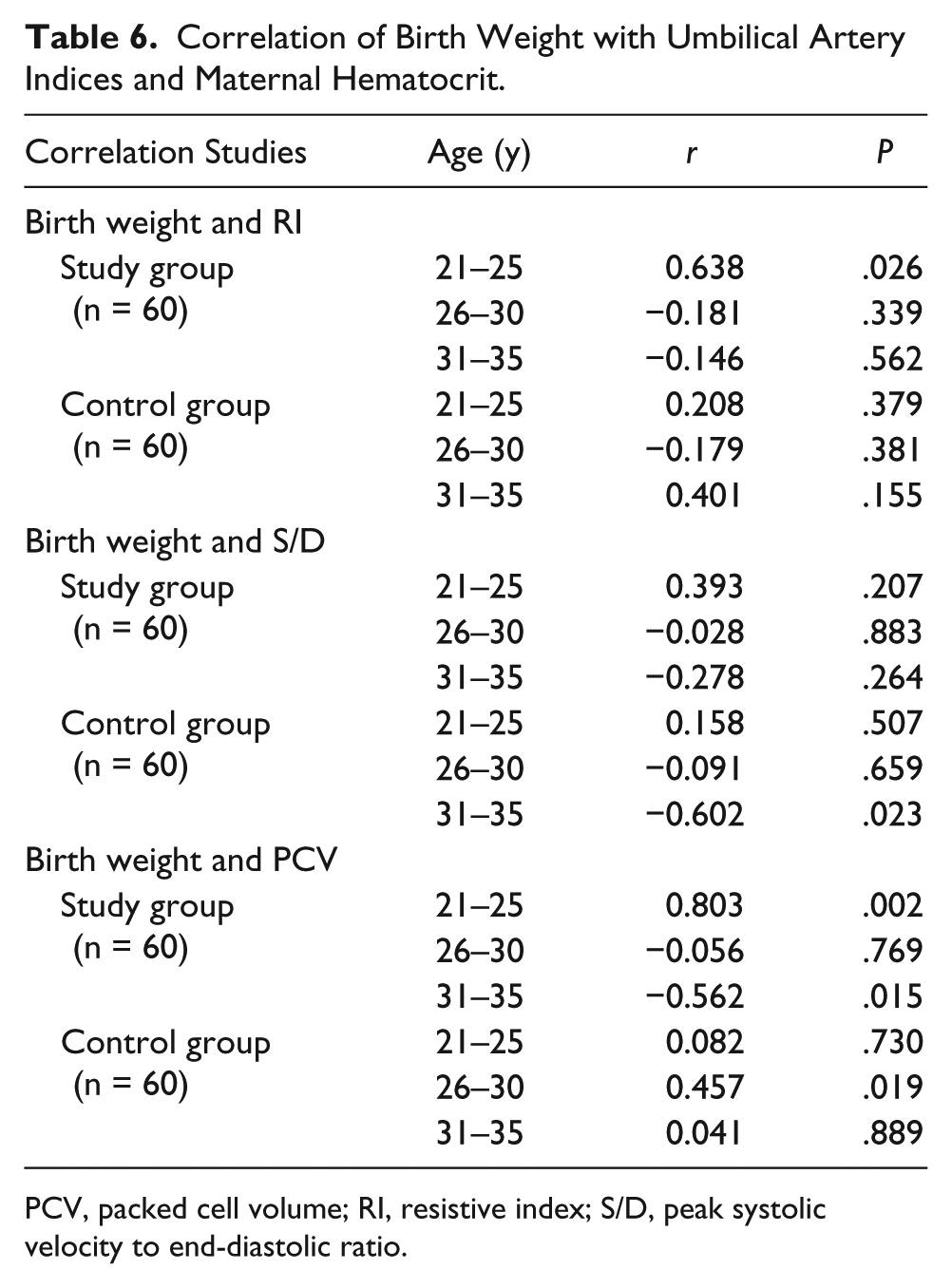
PCV, packed cell volume; RI, resistive index; S/D, peak systolic velocity to end-diastolic ratio.
Table 7 depicts a correlation of Apgar 5 scores and umbilical artery Doppler indices. There was a moderate positive correlation in the 26- to 30-year age bracket (P = .047) and a significant inverse relationship between S/D and Apgar 5 score in the 31- to 35-year age bracket (P = .002).
Correlation of Apgar 5 With Umbilical Artery Indices.
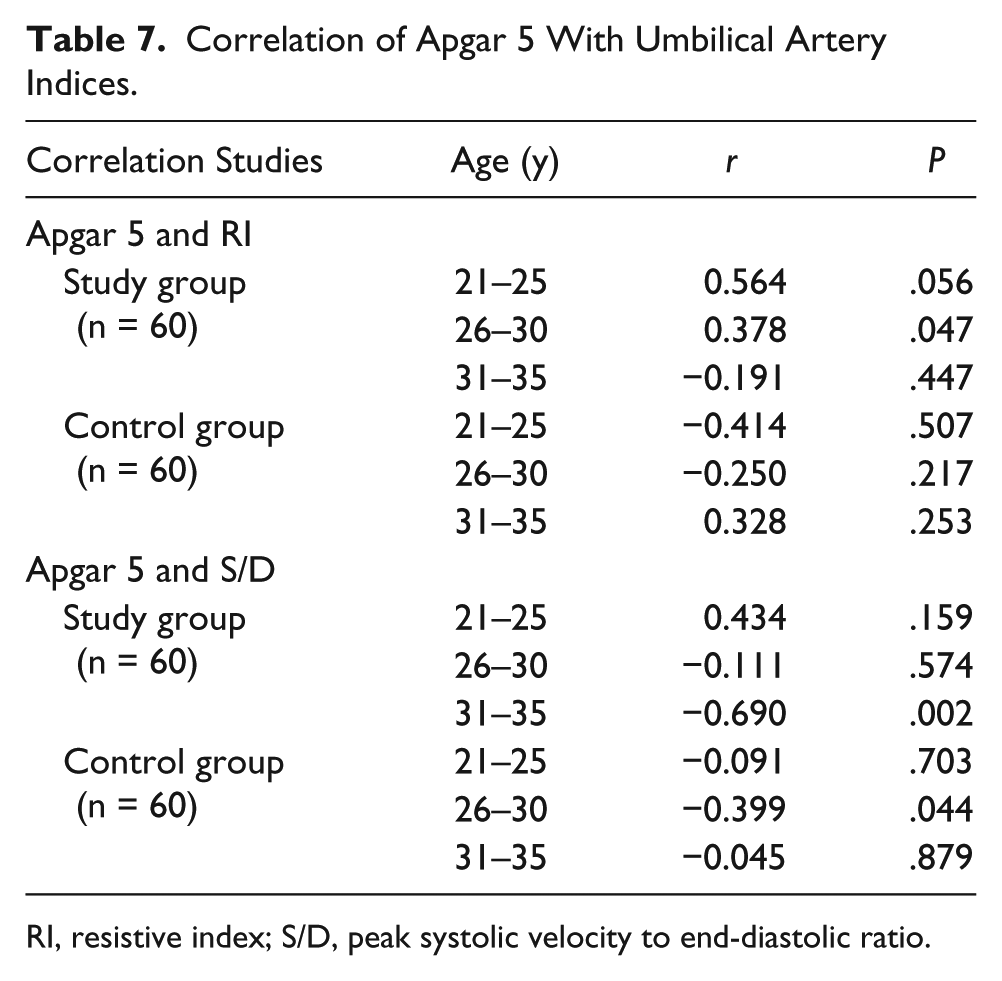
RI, resistive index; S/D, peak systolic velocity to end-diastolic ratio.
The ROC curve at 26 weeks GA is shown in Figure 5. The S/D ratio was more accurate than RI in detecting IUGR, with a larger area under the curve (AUC), but these were not significant (P = .129 and .473, respectively). The AUC was 63.2%, however, suggesting an overall poor test of accuracy. Sensitivity and specificity were 67% and 53% for the S/D ratio and 53% and 62% for RI at a cutoff of >3.40 and >0.70, respectively.
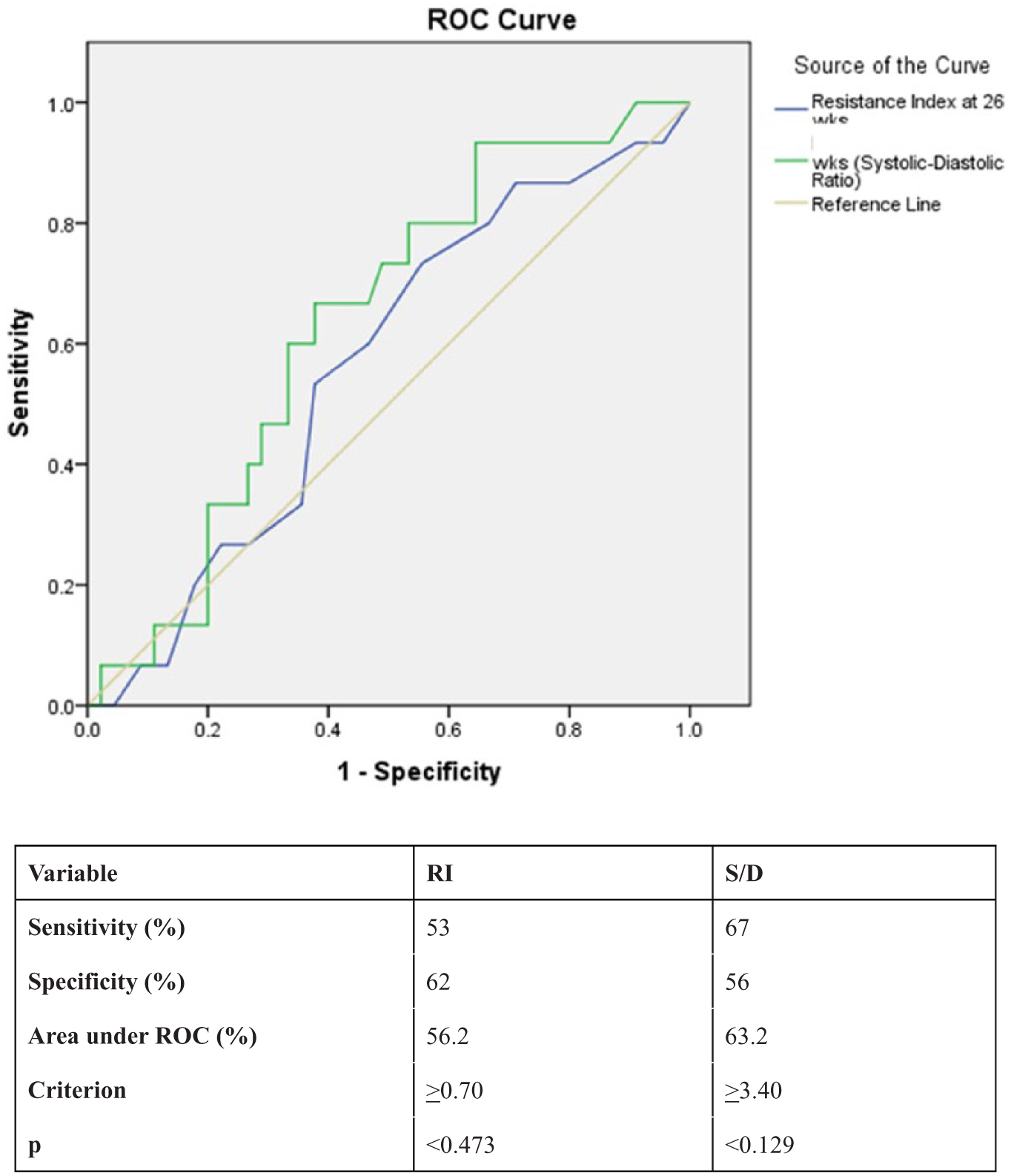
Receiver operating characteristic (ROC) curves for umbilical artery Doppler indices regarding prediction of intrauterine growth restriction at 26 weeks gestational age. RI, resistive index; S/D, peak systolic velocity to end-diastolic ratio.
Discussion
The burden of sickle cell anemia continues to be an important public health issue in sub-Saharan Africa, where the majority of patients reside. Although basic health care and education are improved, more individuals continue to be affected by this disease. Improved life expectancy and quality-adjusted life years (QALYs) with reproductive abilities are comparable to the general population. 42 Sonography and Doppler studies are able to detect at-risk fetuses and guide the clinician in timely management of mother and baby, thus contributing to improved overall outcomes.
The baseline physiological state of HbSS patients is anemia. This has an adverse effect on multiple organ systems, including the fetoplacental circulation. Similar findings were seen in this study, with a significant difference in hematocrit levels noted between the study (HbSS) and control groups (HbAA). This was also seen in a study by Bowers et al., 43 which showed an optimal hematocrit level to be 26% in sickle cell disease patients, as opposed to 33% in healthy subjects. Mean hematocrit levels in this study (23.4%) were also in consonance with that observed in the study by Wilson et al. 44 The lower limit of the hematocrit level in pregnant sickle cell disease patients is uncertain. 44 The low hematocrit levels observed in sickle cell anemia patients are due to an attempt to improve blood flow. Blood flow is determined by blood viscosity, which is governed by PCV or hematocrit levels, total serum protein concentration, and deformability of red blood cells. HbSS patients have a higher level of circulating deformed red blood cells (tending toward increased viscosity). This may be counteracted by a reduction in PCV, resulting in increased flow. Odum et al. 45 reported an increase in perinatal mortality in HbSS pregnancies from low hematocrit levels with a negligible change in maternal hematocrit levels throughout the pregnancy. Similar research findings were noted in this study with the mean hematocrit found to be relatively constant in the course of pregnancy in HbSS patients.
Kidanto et al. 38 also noted that the risk of preterm delivery increased significantly with the severity of maternal anemia, which in turn increases the risk of very low birth weight babies. Bora et al. 46 independently noted that at hemoglobin levels of <8 g/dL, there was an increased risk of small for GA babies as well as low birth weight babies.
Lower birth weight of babies born to HbSS mothers have also been noted in several studies.47–49 Low birth weight in HbSS pregnancies has been attributed to the increase in maternal morbidity, with resultant chronic affectation of the fetoplacental circulation. 44 This was also noted in this study, where the mean birth weight was lower and statistically significant compared with that of the control group in the three age groups. The highest birth weights were seen in the 31-to 35-year age group in HbSS patients. The parity in this age group was highest, suggesting a progression to larger babies with subsequent pregnancies. Babies born to nulliparous women (which were a significant proportion of HbSS patients) had lower birth weights compared with their multiparous HbSS and HbAA counterparts.
It should be noted that IUGR is a multifactorial condition and does not necessarily mean reduced fetoplacental circulation. Its definition and diagnosis vary between centers and geographical regions. The number of growth restricted fetuses (abdominal circumference [AC] below the 2.5th percentile and fetal weight less than the 10th percentile) at 26 weeks GA was zero. Low numbers of growth-restricted fetuses were seen in the studies conducted by Wilson et al. 44 and Chakravarty et al., 50 which could be due to the inclusion of sickle cell hemoglobin C (HbSC) patients in their study. The latter was also a retrospective study with limited data on timing of IUGR.
The Apgar score reflects the status of the newborn infant immediately after birth 51 and is a useful index of the response to resuscitation. Perinatal mortality relates inversely with this score, but low 5-minute scores alone are not conclusive markers of an intrapartum hypoxic event. 52 Mean Apgar 5 scores in this study were consistently >8 in each of the three age groups. The highest score was seen in the 31- to 35-year age bracket in both study (HbSS) and control (HbAA). Similar to this study, however, Al Suleiman et al. recorded high 5-minute Apgar scores; this was attributed to the less indolent course of sickle cell disease in their environment. 53 Lower scores were, however, noted in studies by Afolabi et al. 47 and Ogedengbe and Akinyanju. 54 This is at variance with the current study and may be due to the improvement in antenatal care and health care delivery services in Nigeria. 55
There is an exponential increase in maternal morbidity from the start of the third trimester, with previously stable patients developing crises and requiring transfusions with attendant adverse outcomes. 56 This may account in part for the finding of poor outcomes in previously uncomplicated HbSS pregnancies.
Mean RI and S/D ratio at 26 weeks were marginally higher and lower, respectively, in the HbSS group. These differences were, however, not significant (P = .729, P = .237). This could be due to physiological placental bed microvascular changes that are yet to be fully functional early in the third trimester. There is also the possibility that the microvascular placental abnormalities in sickle cell disease have yet to become overt. These findings are also in consonance with that obtained in studies by Acharya et al. 57 and Arora et al. 34 in low-risk groups at the same gestational age. Bahado-Singh et al., 58 however, recorded higher systolic to diastolic (S/D) ratios in uncomplicated pregnancies. This variance may be due to the timing of the Doppler study, as Anyaegbulam et al. 33 noted a time lag of an average of 3 weeks between the detection of abnormal umbilical artery Doppler indices and abnormal fetal nonstress test. The current study also demonstrated that although poorly sensitive at 26 weeks GA, the S/D ratio is a more accurate predictor of intrauterine growth restriction compared with the RI. This is similar to work done by Anyaegbulam et al. 33 and Beattie and Dornan. 59
Correlation studies of parity with umbilical artery indices demonstrated a weak direct relationship with the RI and a negligible relationship with the S/D ratio. There was no relationship between parity and the S/D ratio in the control group. This is similar to findings in the study by Arora et al., 34 in investigating the significance of umbilical artery velocimetry in the perinatal outcome of growth-restricted fetuses. Mendelson et al. 60 also reported no relationship between parity and RI in a study on normally progressing pregnancies.
Correlation of packed cell volume with Doppler velocimetry revealed a strong positive relationship in the 21- to 25-year HbSS group and a strong inverse relationship in the 26- to 30-year group. The latter was noted to be statistically significant. This may be explained by the finding of Brun et al., 61 who also noted a strong positive relationship between hematocrit and RI. This was ascribed to an increase in blood viscosity, thus increasing impedance. Their study, however, included patients with gestational ages ranging from 25 to 30 weeks, and there was no reference to maternal age. Anyaegbulam et al. 33 reported significant abnormal velocimetric measurements in HbSS patients, but velocimetry was done on four consecutive fortnightly occasions starting from 28 weeks. 33 Correlations between Doppler indices and maternal PCV were otherwise weakly inverse or with negligible correlation and not significant. Of note is the strongly inverse relationship obtained in the 21- to 25-year control group, which may be due to other factors not evaluated in this study.
This study found that at 26 weeks’ gestation, composite fetal weights of the HbSS pregnancies were comparable to those of the control group. Subsequent birth weights were, however, significantly lower compared to the control group, suggesting that adverse events in HbSS pregnancies may likely occur late in the third trimester, thus preventing these fetuses from reaching their full growth potential.
Almstrom et al. 62 noted that normal antenatal Doppler cannot be taken as an indicator of low risk in pregnancies where the fetus is small for gestational age. It is assumed that Doppler studies are able to distinguish between constitutionally small and growth-restricted fetuses 62 ; in practice, however, small fetuses with eventual IUGR may have normal umbilical artery Doppler indices, 56 as found in this study.
The correlation between birth weight and Doppler velocimetry revealed a statistically significant positive correlation between birth weight and RI and birth weight with PCV within the 21- to 25-year age group in the study population. Perhaps this could result from relatively “untested” maternal hemodynamic capacity of pregnancy in this subdivision. Higher levels of fetal hemoglobin (HbF) in HbSS patients, which have been shown to be protective, may also play a role. 63 A weakly insignificant and negligible correlation was noted in the other age groups, suggesting that other factors not tested for in this study may be contributory. A study by Srinivasan et al. 64 showed increased villous vascularity in placentae from anemic mothers. This placental arrangement is complete by 28 weeks’ gestation. It is possible that other factors play a significant role in reversing the effect of this late in third-trimester patients, who have adverse outcomes.
There was a moderate positive relationship between Apgar 5 score and RI in the 26- to 30-year age group of HbSS patients. This is contrary to what is expected and could be due to the prevalence of concomitant illness not evaluated in this work. Other subject groups showed negligible to moderate inverse correlations that were statistically insignificant. This could be due to the numbers of subjects in each group. All the patients in this study were scheduled, and thus overall outcome was improved in HbSS mothers due to active management of the term fetus.
There was a higher frequency of operative delivery in HbSS patients in this study (see Figure 4). This finding is similar to work done by Wilson et al. 44 and is probably reflective of the increased frequency of obstetric complications in HbSS patients.
The ROC curve in this study was a poor discriminatory test, suggesting that umbilical artery Doppler interrogation is of limited value in fetal assessment at 26 weeks GA. S/D was noted to have a larger AUC and was also more sensitive in the prediction of IUGR compared with RI. Beattie and Dornan 59 also found that S/D was the more accurate predictor of growth restriction in the third trimester. Anyaegbulam et al. 33 found an S/D cutoff of >3 in the prediction of growth restriction. This is at variance with this study, in which the cutoff was >3.4. This finding may be due to the fact that velocimetry was carried out between 28 and 34 weeks in the former study.
Limitations
The results of this study are applicable only to regular attendees at the antenatal clinic and uncomplicated HbSS pregnant women at the 26-week GA period. While umbilical artery Doppler indices were shown to be useful in predicting obstetric outcome, this study did not include those patients with extraneous complications that commonly occur in patients with sickle cell anemia.
A small convenience sample was also used, and the results may differ from those in a study done in a larger cohort.
Conclusions
This study showed that umbilical artery velocimetry in uncomplicated HbSS pregnant women at 26 weeks was comparable to HbAA women at the same GA. There was a relationship between umbilical artery Doppler and maternal PCV in the 26- to 30-year age group, birth weight, and Apgar score of HbSS patients. There was, however, no relationship between Doppler indices at 26 weeks and fetal weight in both HbSS and HbAA.
S/D ratio, in determining IUGR when compared with RI, was poorly sensitive and poorly specific, given the ROC curve. S/D ratio, however, had a larger AUC compared with RI, indicating better accuracy in the prediction of IUGR.
The number of growth-restricted fetuses at 26 weeks was zero. Perinatal outcome revealed an increase in the number of low birth weight babies from HbSS mothers, but Apgar scores were remarkably improved, probably due to active management of the term fetuses.
Recommendations
Umbilical artery Doppler indices in 26- to 30-year and 31- to 35-year age groups were equivocal in this study population. Further work later in the third trimester is advised as other studies showed a significant relationship between perinatal outcome and velocimetry. The good perinatal outcomes in this study may be attributable to other hemoglobin subtypes not tested for in this study. This may be overcome by detailed serum electrophoresis by the researcher in subsequent studies. In addition, patients with complications and irregular or nonantenatal clinic attendees should be included in follow-up studies. Finally, further classification based on drug history of HbSS patients should be included in follow-up studies, so as to evaluate the presence of possible confounders and perinatal outcome.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.