
Abstract
For the fetus at risk for intrauterine growth restriction (IUGR), umbilical cord Doppler provides the clinician valuable information about fetal circulation. When the cord Doppler is abnormal, spectral analysis of the middle cerebral artery (MCA) gives additional information about perfusion to the fetal brain. This case report describes a 31-week gestational age fetus referred for a biophysical profile and umbilical cord Doppler because of an abnormal nonstress test.
Keywords
For the developing fetus, the interface between the maternal and fetal circulations at the level of the placenta is critical for proper fetal growth and development. When this circulation is compromised, the fetus is at risk for intrauterine growth restriction (IUGR). Although IUGR has a number of causes such as fetal infection, underlying maternal pathology, or genetic disorders, abnormal vascular placental perfusion is the most common.
Spectral Doppler of the umbilical cord is used to assess the perfusion of the placenta. When the spectral analysis of the umbilical cord is abnormal, the fetal middle cerebral artery (MCA) and/or ductus venosus (DV) should be sampled. This hemodynamic information gives the clinician the tools to make the management decisions that will affect fetal outcome.
The following case report describes the importance of incorporating umbilical cord Doppler as a routine practice when performing a biophysical profile (BPP). When the cord Doppler demonstrated an abnormal waveform, by department protocol, an MCA Doppler was obtained to provide additional information regarding fetal cerebral perfusion. In this case, MCA Doppler was diagnostic of the brain-sparing effect.
Case Report
Clinical Details
A woman in her 30s, gravida 3, para 2, presented for a BPP following a nonreactive stress test. Her past obstetrical history was significant for a stillbirth at 38 weeks. On the basis of the last menstrual period, the fetus had a gestational age of 31 weeks, 2 days, which correlated with a prior gestational age of 19 weeks, 2 days based on a previous sonogram. The nonreactive stress test demonstrated decreased fetal movement. The patient was referred for a BPP with umbilical cord Doppler, which was performed using a Siemens Sequoia (Siemens USA, Washington, DC) using a 4C1-S transducer (bandwidth 4-1 MHz).
The biophysical profile was performed following the American College of Obstetrics and Gynecology guidelines. The BPP assessment included evaluation of fetal tone, fetal movement, fetal breathing, and amniotic fluid volume.
The fetus scored eight out of a possible eight points. Fetal heart rate was 138 beats per minute, with normal sinus rhythm. Total amniotic fluid index (AFI) was 8 centimeters. Fetal biometry demonstrated a fetus of 29 weeks, 5 days gestational age and in the 23rd percentile for growth.
Umbilical cord Doppler was performed without angle correction and sampled mid-cord. Umbilical cord Doppler samples were also obtained at the fetal and placental ends of the cord. The data obtained from the spectral analysis included standardized measurement of the systolic to diastolic ratio (S/D ratio), pulsatility index (PI), and resistive index (RI). By department protocol, if the umbilical cord Doppler is abnormal, the fetal MCA is sampled and an S/D ratio for the MCA is also calculated.
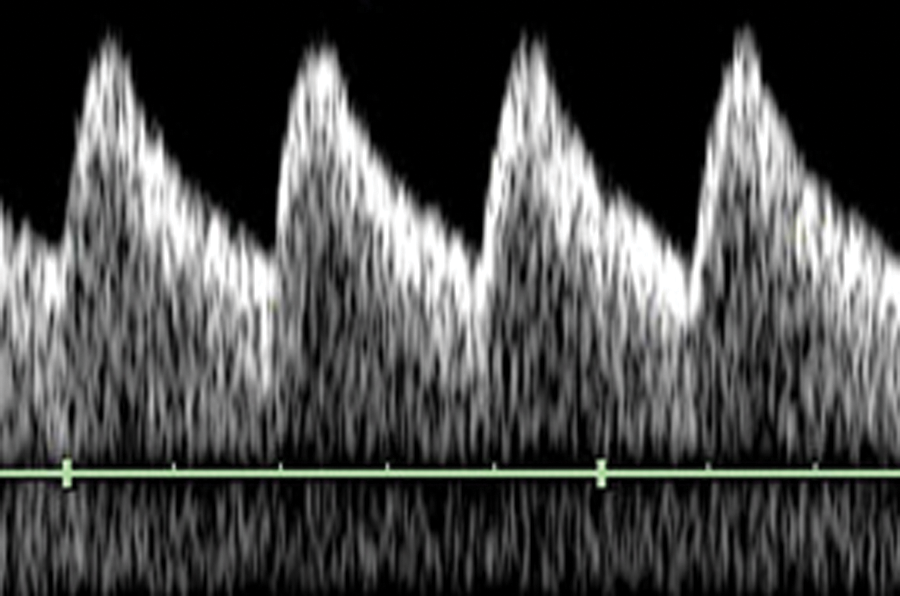
The spectral analysis of the umbilical cord demonstrated swift upstroke to a systolic peak with loss of diastolic flow (Figure 1). The S/D ratio was calculated at 23, the PI was 1.82, and the RI was 0.96. The umbilical cord was then sampled at the fetal end (Figure 2) and the placental end (Figure 3). Both areas demonstrated the same abnormal Doppler S/D ratio, PI, and RI as mid-cord (see Figure 4 for comparison to normal).
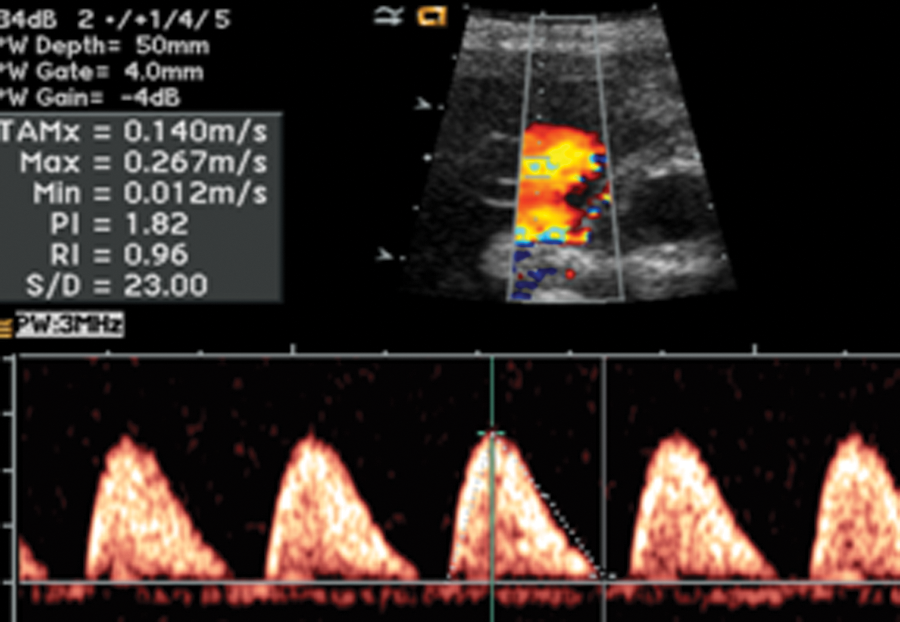
Umbilical cord Doppler with elevated systolic to diastolic ratio of 23.
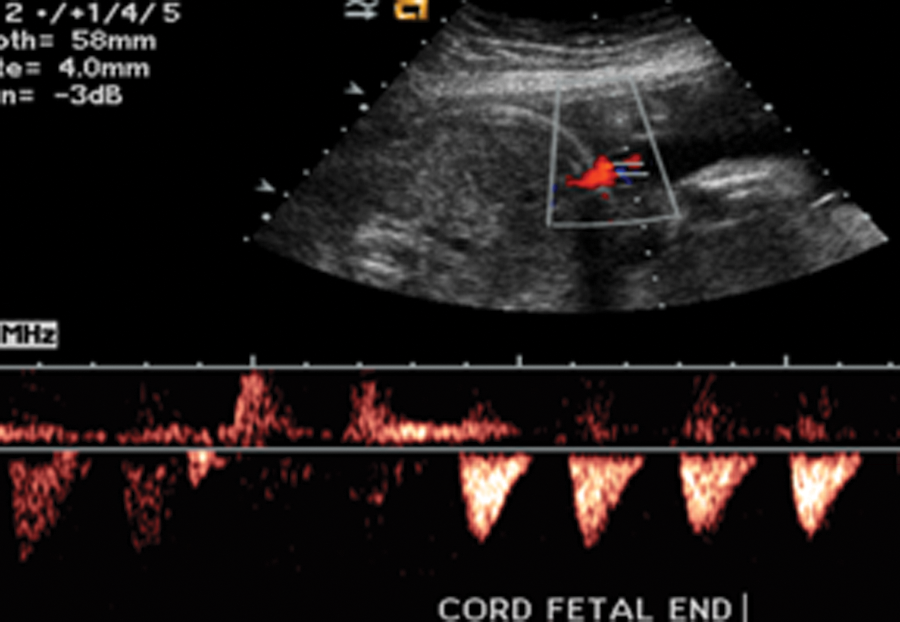
Umbilical cord Doppler at the fetal end showing loss of diastolic flow.
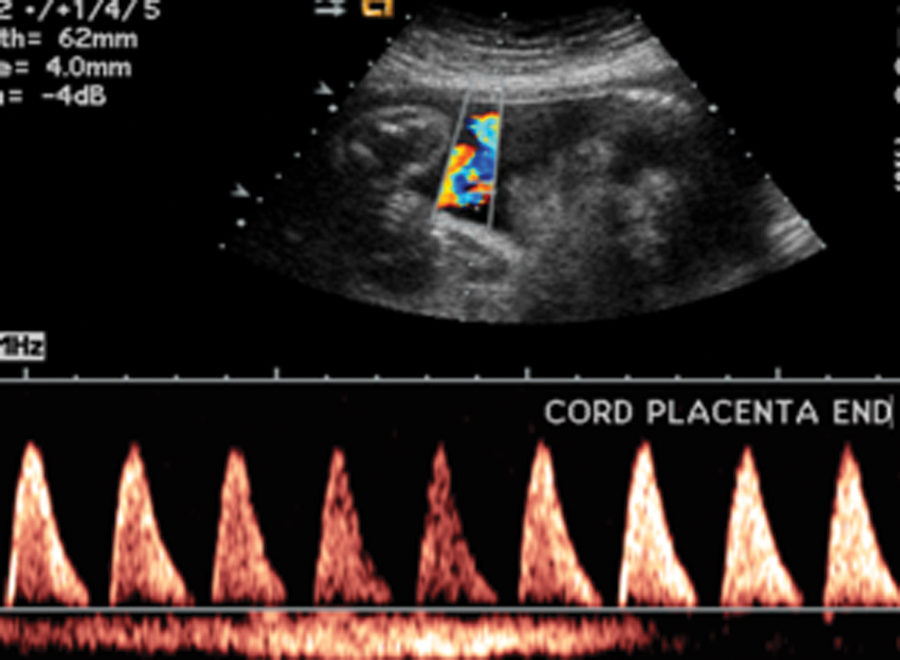
Umbilical cord Doppler at the placental end showing a similar loss of diastolic flow.
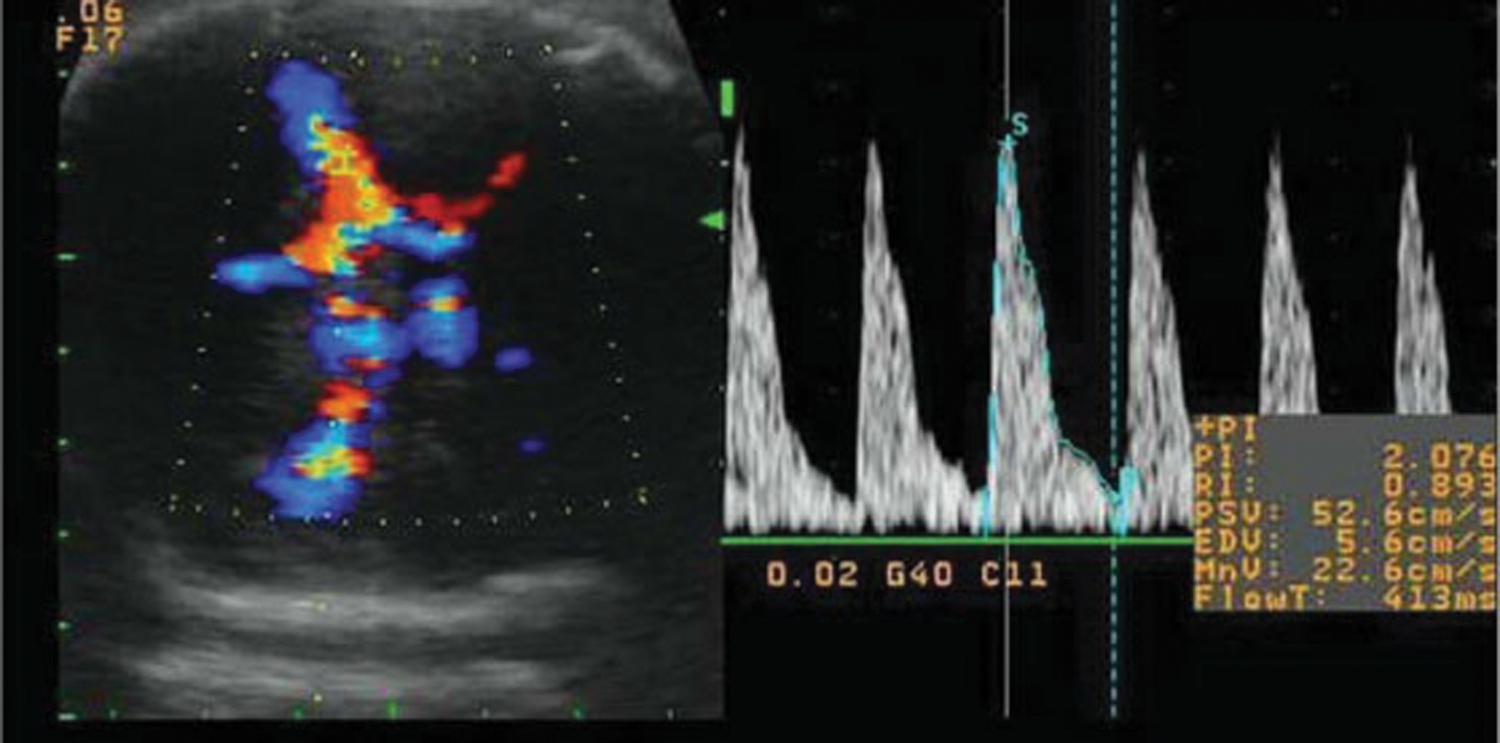
Because of the abnormal results of the cord Doppler, the fetal MCA was then sampled at the junction with the internal carotid artery (Figure 5). The MCA Doppler demonstrated significantly increased velocity through end diastole (see Figure 6 for comparison to normal). The MCA S/D ratio, when compared with the umbilical cord S/D ratio, was markedly reduced at 3.4; the MCA RI was 0.71. This fetus was then referred to the care of a perinatologist.
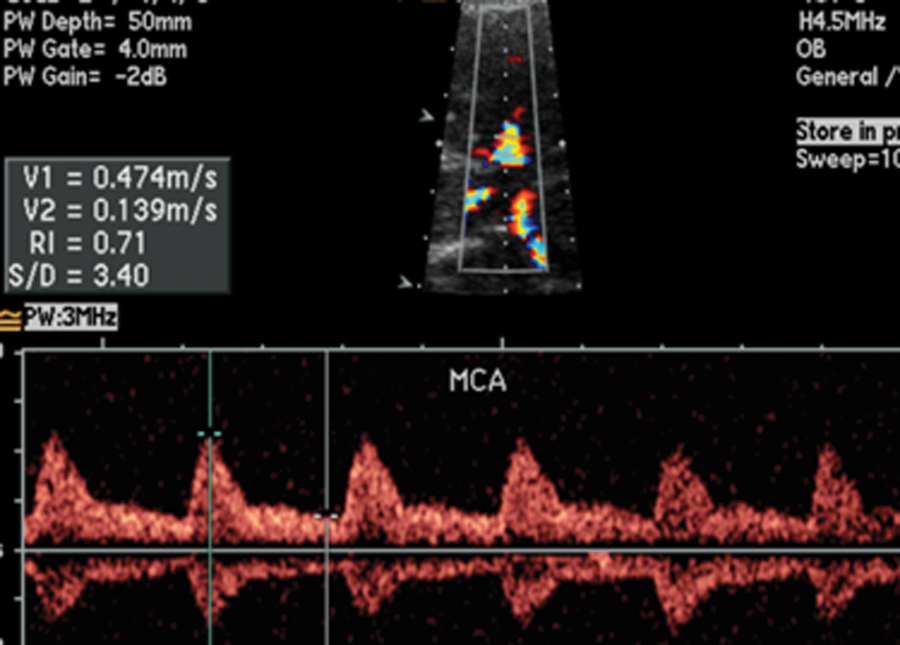
Middle cerebral artery Doppler showing increased velocity through end diastole.
Normal middle cerebral artery Doppler with diminished antegrade end-diastolic flow. Note the difference compared with Figure 5.
Discussion
The placenta’s function can be compared with the function of the lungs. The fetus receives oxygen-rich blood and nutrients from the mother via the placenta and umbilical vein.1–3 The maternal side of the placenta is analogous to a venous lake. On the fetal side of the placenta, villi arise from small branches of the umbilical arteries and vein and project into the placental venous lake. It is at the level of the villi that oxygen (O2) and carbon dioxide (CO2) are exchanged by the fetal blood. 2
In the uncompromised fetus, umbilical vein blood is about 80% saturated with oxygen compared with an approximate 98% arterial oxygen saturation in normal adults. Approximately 50% of umbilical vein blood will pass through the fetal liver. The remainder bypasses the liver and enters the inferior vena cava (IVC) via the ductus venosus.1,2 Blood from the ductus venosus joins deoxygenated blood returning from the trunk and lower extremities and, along with blood from the liver via the hepatic veins, merges to form streams in the IVC. 1 Within the IVC, the streams of blood will maintain their identity. 1 They are divided into two separate, although unequal, streams by the edge of the interatrial septum (crista dividens). 1 The larger of these two streams is blood mainly from the umbilical vein. This blood is diverted to the left atrium via the patent foramen ovale. 1 The smaller of the two streams of blood enters the right atrium and is joined by blood from the superior vena cava. 1 The superior vena cava is composed of blood returning from the upper parts of the body and from the myocardium. 1 Blood shunted through the foramen ovale to the left atrium is joined by blood returning from the lungs. 1 Blood moves from the left atrium to the left ventricle into the aorta. In the ascending aorta, the majority of the blood goes to the head, upper thorax, and arms. 1 The remainder of the blood joins blood from the ductus arteriosus and supplies the rest of the body and placenta. 1 The majority of the blood in the descending aorta comes from the right ventricle and ductus arteriosus; it will enter the two umbilical arteries and supply the placenta.1,3 It is this blood flow from the umbilical arteries that is measured when performing umbilical cord Doppler.
After 30 weeks’ gestational age, the normal umbilical artery flow should have low-resistance characteristics, and the S/D ratio should be 3 or less with perfusion demonstrated throughout systole and diastole (Figure 4). 4 The PI and RI values should be in the 50th percentile for gestational age; accordingly, a 31-week gestational age fetus would be expected to have a PI of 0.997 and RI of 0.600. 3
The normal fetal MCA will demonstrate a higher resistance waveform than the umbilical cord, although antegrade flow is maintained through the cardiac cycle (Figure 6). The normal MCA S/D ratio will always be greater than the S/D ratio of the umbilical cord for all gestational ages. 4 The PI will have a predicted value for a specific gestational age, and the RI will be in the 50th percentile for gestational age.3,4
Intrauterine growth restriction is compromised fetal growth. According to Callen, 3 “In 1967, Battaglia and Lubchenco defined SGA (small for gestational age) as birthweight being below the 10th percentile for gestational age.” Intrauterine growth restriction is now viewed as a fetus that is failing to achieve its growth potential. 3
The intrauterine growth–restricted fetus tends to have a poor prognosis, with increased fetal morbidity and mortality.
The IUGR fetus is hypoxic, and in this hypoxic state, the fetal brain circulation vasodilates to allow more oxygenated blood to flow to the head. In doing so, more blood is shunted away from the liver to the head. 5 This shunt, the ductus venosus, will dilate and capture as much as 70% of the umbilical vein blood, therefore increasing the size of the stream of blood passing through the IVC to the left atrium via the foramen ovale. 6 It is this mechanism that affects the size of the fetal liver, altering the abdominal circumference, and making this measurement a sensitive indicator in the diagnosis of IUGR.
Theoretically, the brain-sparing effect is the result of cerebral vasodilatation as a response to the hypoxia. Doppler of the MCA will demonstrate a less resistant waveform than the umbilical artery Doppler with an increase in the diastolic flow. This will be reflected in a decrease in the S/D ratio, PI, and RI, which serve as markers of the brain-sparing effect. 7
This case demonstrates the merits of performing at a minimum umbilical cord Doppler when performing a BPP. 8 For this fetus, the umbilical cord Doppler demonstrated loss of end-diastolic flow at samples obtained from the middle of the cord, the placental end, and the fetal end. The cord Doppler velocities showed an elevated S/D ratio of 23, a PI of 1.82, and an RI of 0.96.
The MCA demonstrated the brain-sparing effect. The MCA Doppler showed a lower resistance waveform than the umbilical artery, with increased flow through end diastole. The S/D ratio of the MCA was considerably less than the S/D ratio of the umbilical cord: 3.4 versus 23. The MCA RI was 0.71 versus the expected value of 0.798 in an uncompromised 31-week gestational age fetus.
Conclusion
This case demonstrated the complementary use of umbilical cord Doppler when performing a BPP examination. The BPP failed to demonstrate any fetal compromise. Addition of the umbilical cord Doppler demonstrated possible fetal distress, notably by loss of end-diastolic flow resulting in an elevated S/D ratio. Addition of MCA Doppler measurements showed increased end-diastolic flow and an S/D ratio less than the umbilical cord S/D ratio, evidence of the brain-sparing effect. These findings were instrumental in referring this patient to a perinatologist. The fetus was eventually delivered by caesarean section due to decreased BPP scores, continued abnormal umbilical cord Doppler, MCA Doppler, and fetal growth in the 10th percentile for age.
When performing routine BPPs, incorporating umbilical cord Doppler will give valuable information about the hemodynamic state of the fetus. When the umbilical cord S/D ratio, PI, or RI is abnormal, addition of MCA Doppler and its values for the S/D ratio, PI, or RI can give added information to the clinician for the management of the pregnancy.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The author received no financial support for the research and/or authorship of this article.