
Abstract
Objectives:
The intervertebral disk has traditionally been imaged by magnetic resonance imaging (MRI); however, advances in sonography mean it can now be visualized with this modality. The objectives of this human cadaveric study were to visualize the internal structure of the lumbar intervertebral disks and map any defects. Shear wave sonography was explored as a method for assessing the disks.
Materials and Methods:
In a human cadaver, L4-L5 and L5-S1 disks were imaged with sonography through the anterior abdominal wall and directly through the anterior longitudinal ligament. Gray-scale images and shear wave elastography velocities were obtained. An MRI was performed for image comparison.
Results:
Defects in the disks were clearly seen with sonography, imaging through the anterior abdominal wall and also directly through the anterior longitudinal ligament. The defects identified on sonography were less well visualized on MRI. Shear wave velocities could only be obtained from the anterior aspect of the disk and were unreliable, primarily owing to the stiffness of the tissues.
Conclusion:
Sonography can provide an accurate map of defects within the disk, corresponding with MRI. Shear wave elastography should be used with caution in the human cadaveric intervertebral disk, acknowledging the many confounding factors influencing the measurements.
The intervertebral disk has traditionally been imaged with magnetic resonance imaging (MRI) rather than sonography, being a deep structure covered by the bony skeleton and musculature. Recent advances in sonography have made this imaging assessment a more realistic prospect, with a few studies demonstrating the possibility to assess the lumbar and cervical disks from an anterior approach in slim subjects.1–3 Sonography is a noninvasive test and is readily available in most hospital settings. It is less expensive compared with MRI and has very few contraindications. If the intervertebral disk could be accurately assessed in vivo with sonography, then this could potentially broaden its clinical applications. This could be realized in the bedside assessment to follow-up of discitis or a final check of disk health, immediately before surgery. The effect of flexion and extension of the spine on the disc could potentially be elucidated. Intraoperative sonography could potentially be used to characterize a tear in the disk annulus and thus aid surgical repair. It could also be used to assess the health of an intervertebral disk, with the patient on the operating table. This could guide the surgical decision making of decompression versus decompression with fusion.
In vivo, intervertebral disks are more readily accessible for sonographic assessment from an anterior approach, as the posterior bony arch of the spine reflects the acoustic waves and casts an acoustic shadow where the disk is situated. There is a potential “acoustic window” from a posterior interlaminar approach; however, this is limited and difficult to achieve in vivo. 4 From an anterior approach, acoustic windows of the lumbar disk are also hindered by interposed structures, such as with gas in the intestines. Despite the obstructions, the ultrasound transducer can be oriented to obtain “windows” on certain disks. Gray-scale sonographic imaging demonstrates the most superficial structure of the disk, relative to the transducer, namely, the anterior annulus fibrosus and a limited assessment of the nucleus pulposus. Shear wave elastography has been used to assess superficial (anterior) annulus fibrosus; however, nucleus pulposus and deep (posterior) annulus fibrosus of the disk are currently too deep to be interrogated, from an anterior approach. The structure of the disk has been analyzed in vitro in dog cadavers, with an elegant sonographic depiction of healthy disks. 4 Based on a review of the literature, there are no studies assessing the disks in human cadavers.
This study was designed to determine whether sonography could be used in a human cadaver to accurately map defects in the intervertebral disk and also measure the associated shear wave velocities.
Materials and Methods
The study was approved by the Institutional Research Board of the host institution. A 67-year male cadaver was procured by the anatomy department, and the cause of death was metastatic lung cancer. The cadaver was frozen immediately following death and then fully defrosted for 24 hours prior to the study. The cadaver was imaged when fully defrosted (at 24 hours) and in a room with an ambient temperature of 18°C. The cadaver was used in accordance with the Human Tissue Authority regulations.
MRI of the lumbar spine was performed 3 hours prior to the sonogram, using a 3-Tesla MRI unit (Siemens Skyra model; Siemens Healthcare Ltd, Erlangen, Germany). The sequences obtained were sagittal T2 (time to repetition [TR] = 607 ms, time to echo [TE] =10 ms, 4 mm slice thickness) and axial T2 images (TR = 713 ms, TE = 18 ms, 4 mm slice thickness). The MRI images were initially viewed for adequacy and used as an anatomic “roadmap” for sonographic imaging. The disks were not individually assessed to avoid any potential bias with the subsequent image analysis.
Sonography was performed by the principal investigator, a consultant musculoskeletal radiologist with 7 years of post-Fellowship experience. The sonograms were completed using a Siemens Acuson 2000 ultrasound unit (Siemens Healthcare Ltd). The initial sonographic assessment was performed from an anterior transabdominal approach to the lumbar intervertebral disks. A linear 9-4 MHz transducer (upshifted to 9 MHz for imaging) was placed on the anterior abdominal wall, with gel coupling. Gray-scale (brightness mode) sonographic images were obtained in the mid-transverse section of the disk, recording the level at which the disk was situated. The level of the disk was identified with reference to the sacrum and then counted cranially. Static gray-scale sonographic images and a “cine-clip” sweep through the disk were obtained (Figure 1). Trapezoidal imaging was used, where necessary, to extend the lateral field of view of the disk. The depth from the skin to the most anterior aspect of the disk in the transverse plane was measured. Shear wave elastography maps were obtained in the mid-transverse section of the disk. The shear wave velocity overlay box was sized to cover as much of the disk as possible within the depth of the image, a minimum of 3 × 3 cm. The overlay box was then positioned at the most superficial aspect of the disk, and this depth was recorded. The shear wave velocity color map was generated while holding the transducer still and with a light pressure. The shear wave quality map was visually assessed, and if inadequate, the readings were repeated. The region of interest (ROI) boxes were then placed within the color map of velocities. These were chosen to cover as much of the color map as possible, including all areas that gave rise to measurements. A minimum of five ROIs were placed on the disk. The maps were repeated five times. The transducer was then rotated through 90° to give a midline longitudinal plane. These above gray-scale sonographic assessments and elastography measurements were repeated to account for any effects of anisotropy in the tissues. 5 The equipment was able to measure shear waves with velocities from 0 to 10 m/s. Any readings greater than 10 m/s were labeled as “high,” by the software. These few readings (of which there were three) were rounded down to 10 m/s. The disks amenable to sonographic assessment were L4-L5 and L5-S1. The more proximal disks were obscured by acoustic shadowing from bowel gas. The above measurements with the transducer placed on the anterior abdominal wall were termed “indirect.”
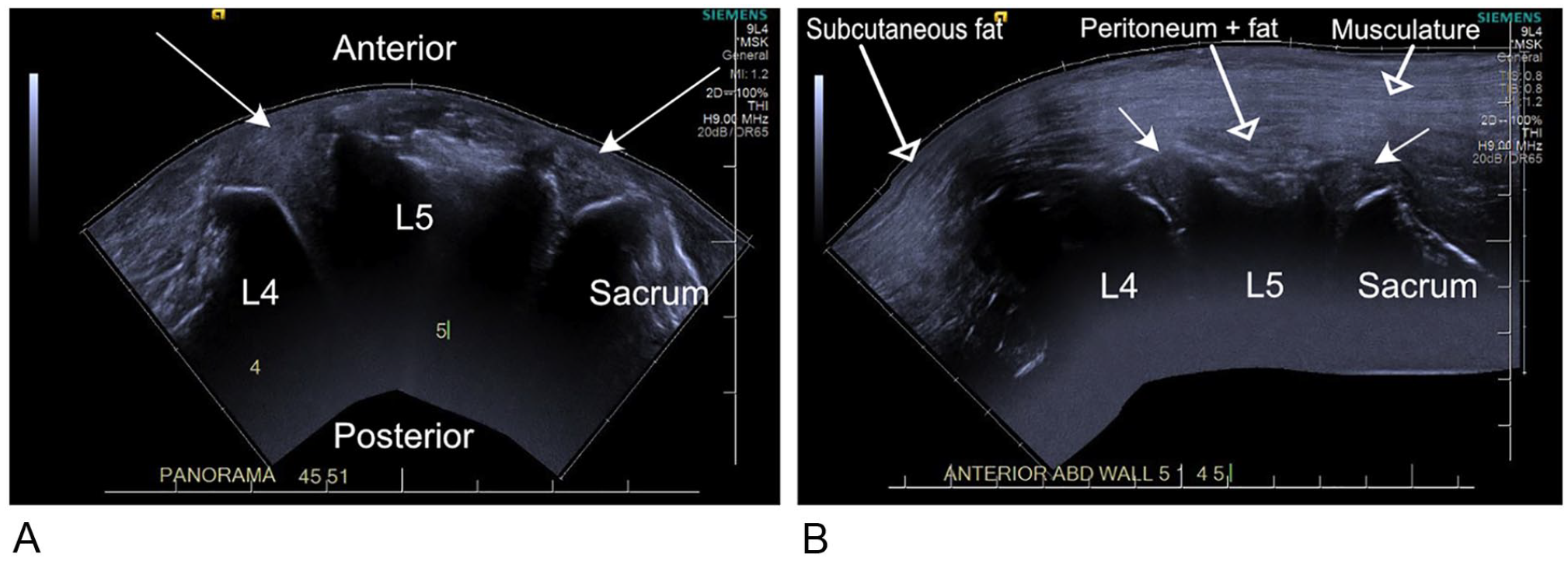
(A) A panoramic sonogram from the direct approach, with the transducer placed on the anterior longitudinal ligament. The vertebral bodies and sacrum cast an acoustic shadow and can be identified from their characteristic shape, in particular the sacrum. The disks are visualized as echogenic objects between the vertebral bodies (arrows). The vertebral endplates are seen at their most anterior aspect, and acoustic shadowing obscures detail from the posterior aspect. (B) A panoramic sonogram from the indirect approach through the anterior abdominal wall, showing from L4 to the sacrum, as in image (A). Note the longitudinally oriented fibers of the abdominal wall musculature (labeled open arrow) lying immediately deep to the subcutaneous fat (labeled open arrow) and anterior to the disks (closed arrow). A thin layer of peritoneum and intra-abdominal fat (labeled open arrow) is also seen, with the bowel displaced out of the imaging field by the probe pressure.
Following the initial MRI and sonographic assessment, the cadaver was dissected by a senior consultant orthopedic spinal surgeon through the left retroperitoneal plane, as per the surgical access for an anterior lumbar interbody fusion. The dissection time was 30 minutes, undertaken at a constant ambient room temperature of 18°C. The dissection created a plane along the anterior aspect of the spinal column, with only the anterior longitudinal ligament remaining covering the discovertebral unit.
The sonographic analysis was repeated with the 9-4 MHz transducer placed on the anterior margin of the disk (directly on the anterior longitudinal ligament) with gel coupling. This created a second matched data set of readings. These measurements were termed “direct” (Figures 2 and 3). Figure 4 is a diagrammatic representation of how the sonographic images of the disks were obtained.
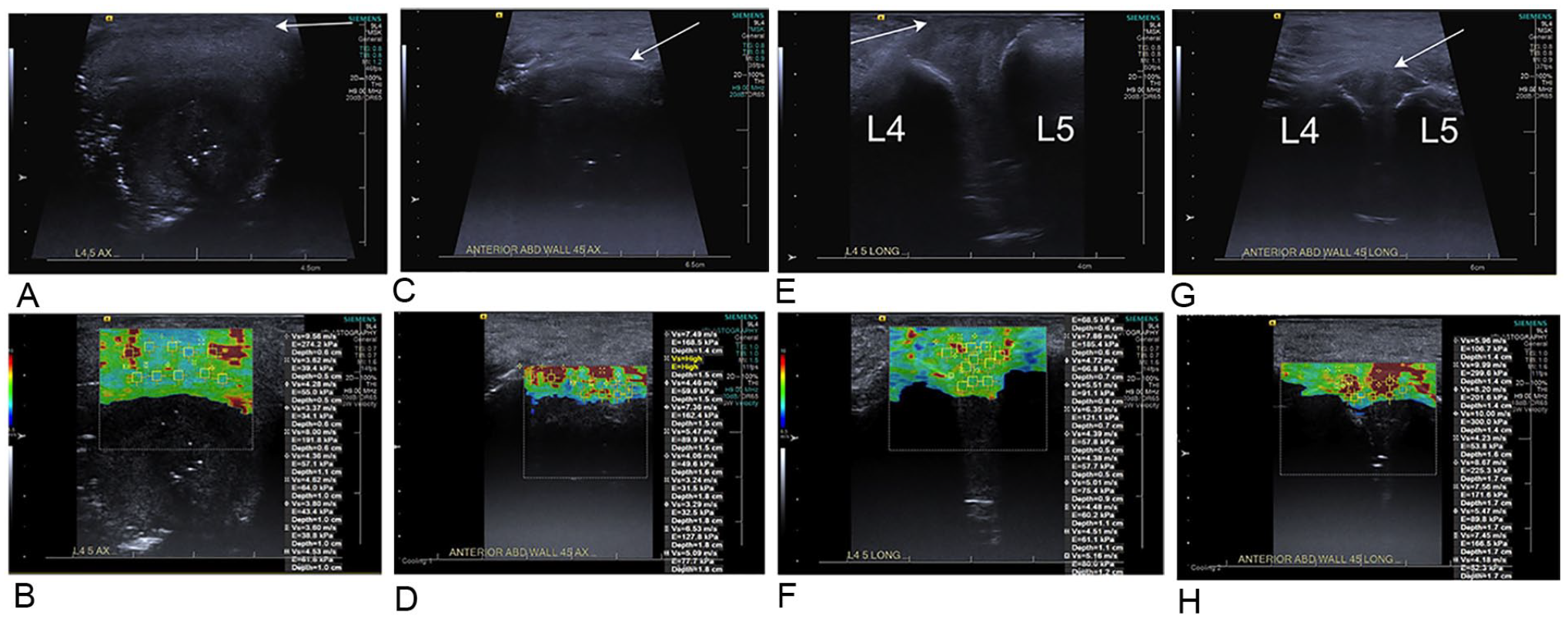
L4-L5 disk with shear wave elastography color maps (B, D, F, H) and B-mode images for correlation (A, C, E, G). The arrow denotes the anterior margin of the disk in this image and subsequent images. (A, B) Transverse direct approach and (C, D) indirect approach. (E, F) Longitudinal direct approach and (G, H) indirect approach. There is a greater proportion of red color in the disks via the indirect approach compared with the direct approach, corresponding to a faster velocity. Note also how most of the disk from the indirect approach has no color map, that is, no shear wave velocities propagated within it.

L5-S1 disk with shear wave elastography color maps and gray-scale sonographic images for correlation. Transverse view images (A, B, C, D) and longitudinal view images (E, F, G, H). Direct approach (A, B, E, F) and indirect approach (C, D, G, H). As in the L4-L5 disk (Figure 2), there is a slightly greater proportion of red color map (faster velocities) via the indirect approach compared with the direct approach. Note also how most of the disk does not propagate any shear waves.
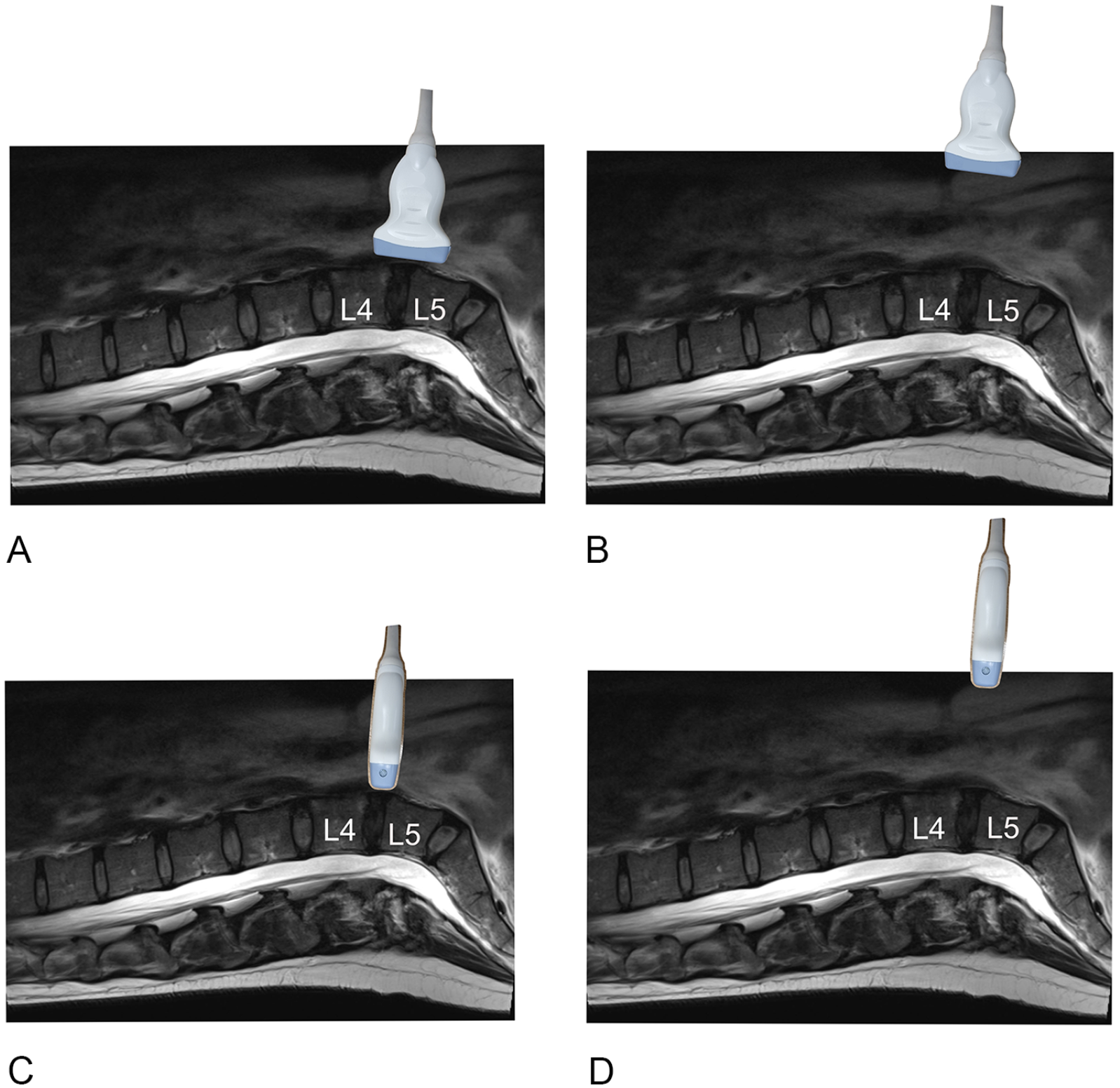
Diagrammatic representation of the image acquisition. A sagittal T2 magnetic resonance image of the lumbar spine in an adult female, presented in the same orientation as the cadaveric sonograms. The sacrum is seen to the right of the image and the thoracic spine to the left. The L4 and L5 vertebral bodies are labeled. The ultrasound probe is placed on the L4-L5 disk, demonstrating the different positions of the probe. (A) Direct longitudinal approach, (B) indirect longitudinal, (C) direct transverse, and (D) indirect transverse.
Image Analysis
The intervertebral disks were assessed by the principal investigator, a consultant musculoskeletal radiologist, who also had performed the sonograms. The image analysis was performed 4 weeks following the image acquisition, using an industry standard DICOM (digital images and communication in medicine) viewer (Fujifilm UK Ltd, Bedford, UK). The sonograms were viewed in longitudinal and transverse planes at L4-L5 and L5-S1, and a score was assigned, according to the method previously described by Naish (see the appendix). 6 The midline sagittal T2 MRI images were viewed on a DICOM viewer and a grading assigned, according to the Pfirrmann grading system (see the appendix). 7 The disk height was measured on the midline sagittal T2 image at the narrowest point of the disk. The images were assessed to see whether the defects visible on the sonogram were also visible on MRI, with a qualitative score assigned of poor, moderate, good, and substantial.
Statistics
The shear wave elastography velocities were pooled for the L4-L5 and L5-S1 disks in longitudinal and, separately, transverse planes. The data were checked for normality by the Shapiro-Wilk test. The data did not follow a normal distribution; hence, the Wilcoxon nonparametric test was used to assess for any difference between the groups.
Pearson’s correlation coefficient was used to assess for any correlation between the pooled longitudinal and transverse measurements. The average shear wave velocity was calculated for each disk. The standard deviation, mean, median, 25th and 75th percentiles, and interquartile range/median were calculated for the shear wave velocities separately for both disks and direct versus indirect measurements. The data available from the visual grading were deemed to be too few to allow any meaningful statistical analysis.
Results
Image Analysis
Sonography was able to interrogate the internal structure of the intervertebral disks. It was possible to visualize the annulus fibrosus and nucleus pulposus of the L4-L5 (Figures 5 and 6) and L5-S1 (Figures 7 and 8) disks as distinct structures using both the direct and indirect methods. The annulus fibrosus was visualized as longitudinal fibers at the periphery of the disk, with a demarcation with the nucleus. Small defects in the disk were visualized as hyperechoic foci within the nucleus of the disk. The internal detail of the disks was better visualized through the direct approach (transducer on the anterior longitudinal ligament) compared with an indirect approach (transabdominal imaging). The anterior aspect of the disk was better visualized compared with the posterior aspect of the disk for both the direct and indirect approaches. The small defects in the disk were better seen on transverse sonographic views compared with longitudinal sonographic views. Conversely, on MRI, the defects were better visualized with sagittal (longitudinal) imaging compared with axial (transverse) imaging. The use of trapezoidal sonographic imaging of the disk did not degrade image quality, as compared with linear imaging.
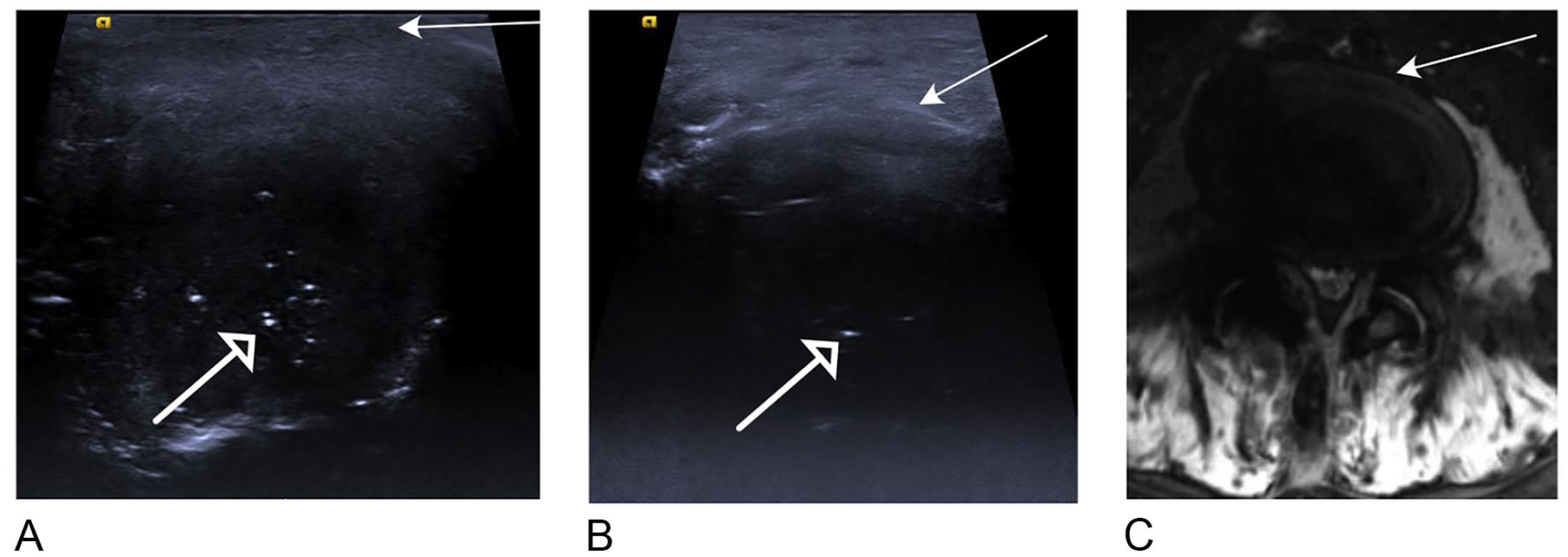
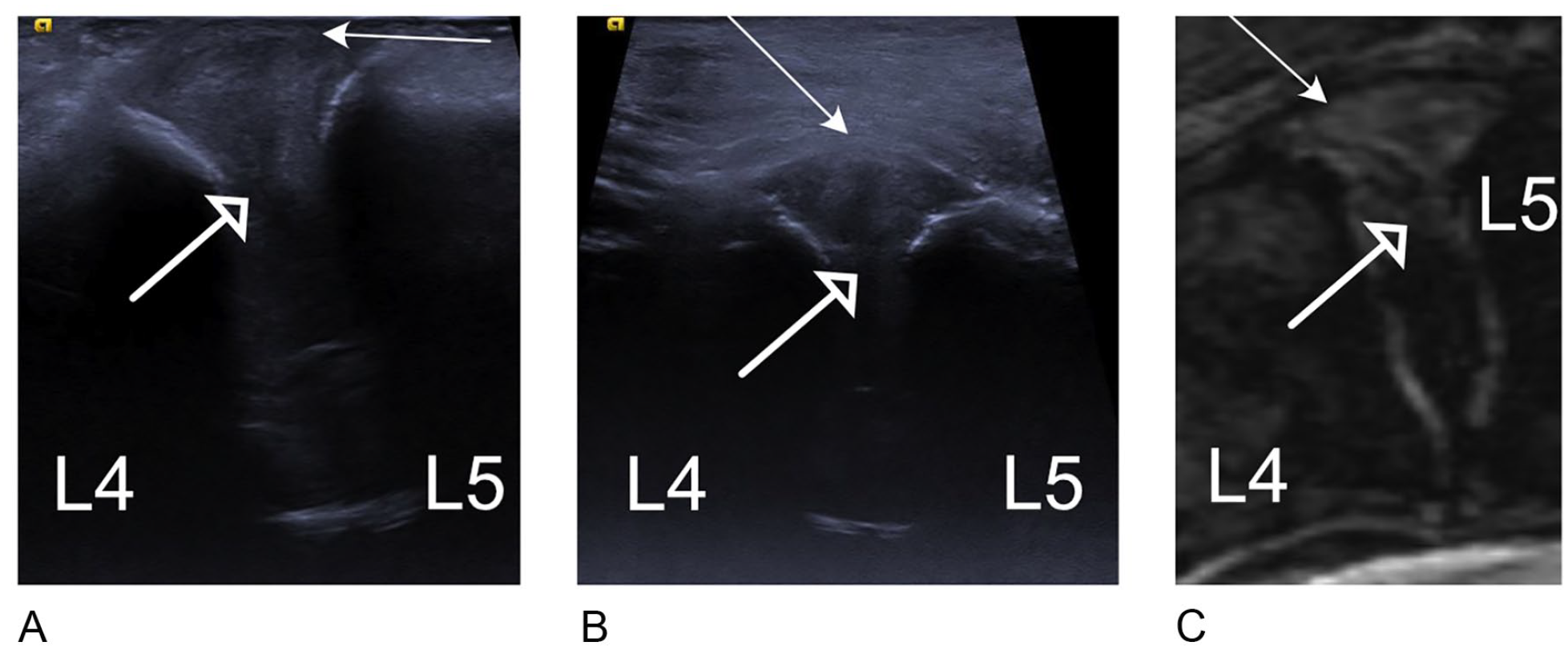
L4-L5 disk, transverse images of (A) direct and (B) indirect B-mode sonogram. The small defects in the disk are visualized as hyperechoic foci (open arrow). Detail is greater for the anterior aspect of the disk, where the radial fibers of the annulus fibrosus can be identified. The nucleus pulposus is seen as a separate structure; however, the demarcation with the annulus fibrosus is indistinct. The posterior fibers of the annulus fibrosus are not separately identified. The indirect image (A) gives less detail of the disk compared with the direct image (B). (C) A transverse T2 MRI mid-disk image. The internal detail of the disk is not well appreciated on this MRI image, with relatively poor spatial resolution compared with the direct ultrasound image.
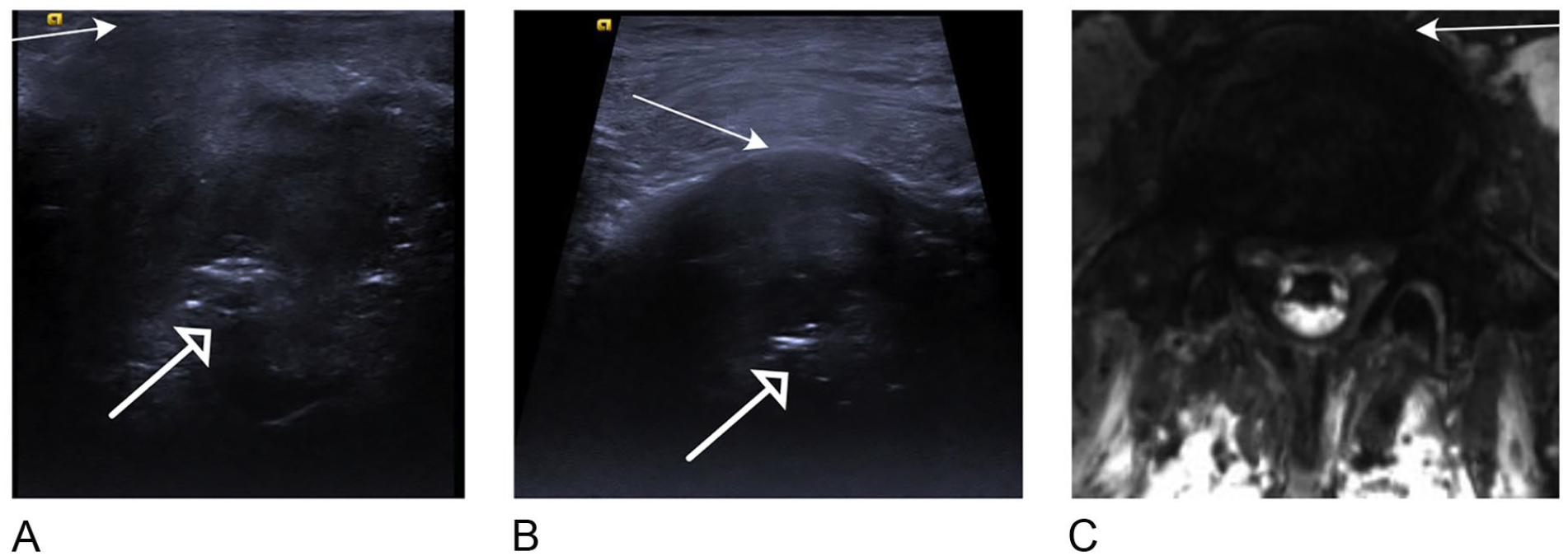
L4-L5 disk, longitudinal images of (A) direct sonogram, (B) indirect sonogram, and (C) T2 MRI. The fibers of the annulus fibrosus are seen at the most superficial aspect of the disk (closed arrow), with a clearer view of the hypoechoic nucleus pulposus (open arrow) compared with the transverse images. The endplates are seen on the sonograms as hyperechoic lines at the cranial and caudal margins of the disk. As in the transverse images, the superficial aspect of the disk is better seen compared with the deep aspect, and the direct sonogram gives a clearer depiction of the disk compared with the indirect sonogram. On T2 MRI (C), the irregular nucleus pulposus (open arrow) appears similar to the ultrasound images, but with less detail.
L5-S1 disk, transverse images of (A) direct sonogram, (B) indirect sonogram, and (C) transverse T2 MRI. As in the L4-L5 disk, the direct approach gives better detail of the small defects (open arrow) compared with the indirect approach and the transverse MRI image.
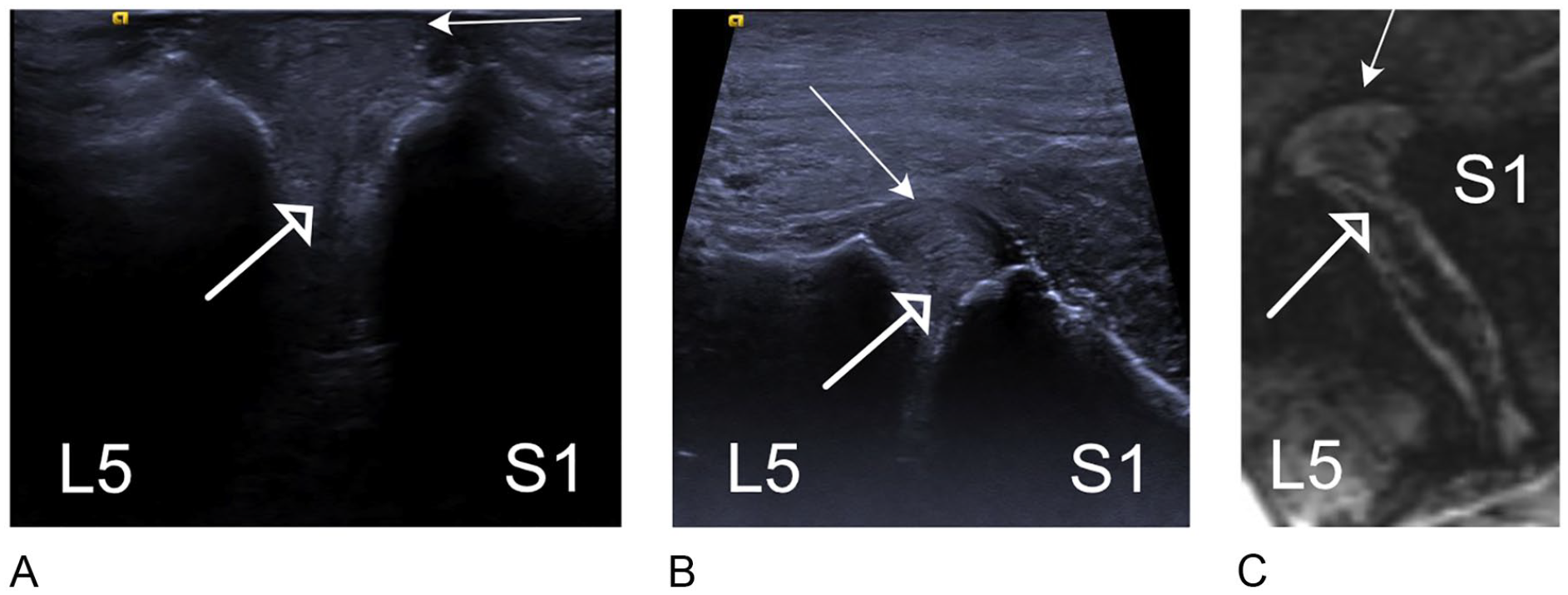
L5-S1 disk, longitudinal images of (A) direct sonogram, (B) indirect sonogram, and (c) longitudinal T2 MRI. The nucleus pulposus is seen as a hypoechoic focus in the middle of the disk (open arrow), which is imaged between the slope of the sacrum and L5.
The L4-L5 disk was graded as 3 by the Naish score for both the direct and indirect methods. The L5-S1 disk was graded as 4 by both methods. This indicates that the disks were very degenerate, with a corresponding Pfirrmann grade, as assessed on sagittal T2 MRI (Table 1).
The Grading Scores That Were Used in the Study for the Intervertebral Disks.
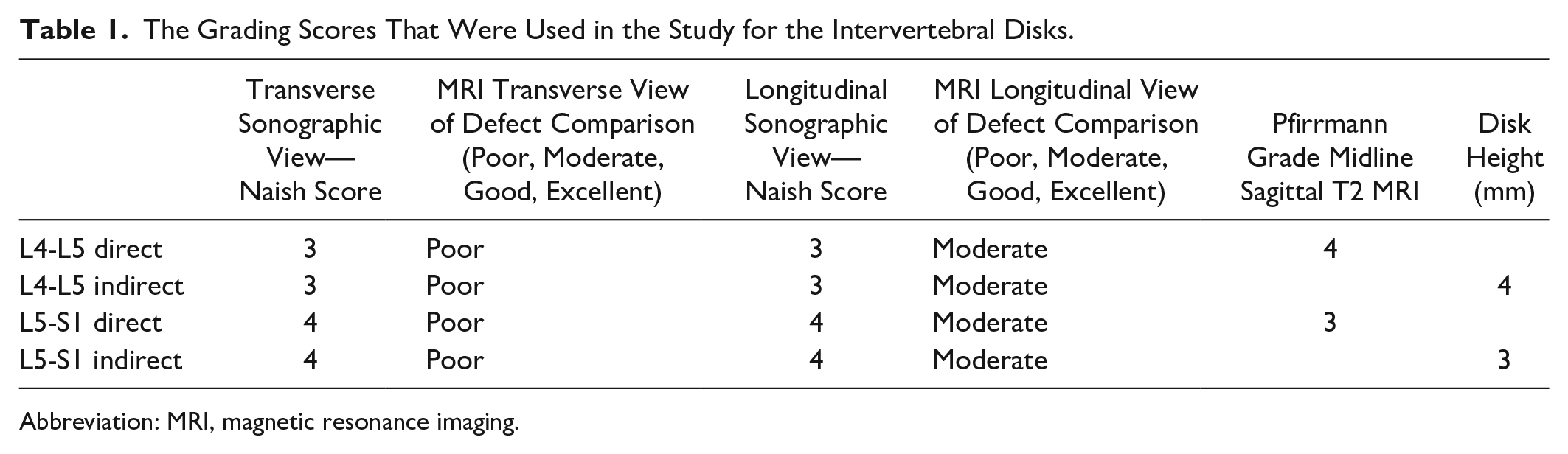
Abbreviation: MRI, magnetic resonance imaging.
Shear wave elastography measurements
It was only possible to obtain consistent shear wave elastograms from the most anterior aspect of the disk, at the annulus fibrosus. The shear wave elastogram was degraded from around 1 cm depth into the disk, equating to around 1 cm depth from the probe using the direct method and 3 cm using the indirect method. This meant that there were no measurements available from most of the nucleus pulposus and posterior anulus fibrosus. The occasional measurement from the nucleus pulposus was disregarded. Tables 2 and 3 summarize the results.
Shear Wave Elastographic Data (Measurements Made in the Transverse View) That Were Obtained for the Intervertebral Disks.

Shear Wave Elastographic Data (Measurements Made in the Longitudinal View) That Were Obtained for the Intervertebral Disks.

A statistical difference was found between direct and indirect pooled shear wave velocities for the L4-L5 disk and L5-S1 disk in both longitudinal and transverse planes (P values are shown in Tables 2 and 3). The mean velocities were greater via the indirect method compared with the direct method, apart from the longitudinal velocity at L5-S1.
The standard deviation from the mean was greater for the indirect velocities compared with the direct velocities at both disks and in both longitudinal and transverse planes. The ratio of the interquartile range/median was also greater for all the indirect measurements compared with direct measurements.
There was no correlation between longitudinal and transverse measurements at either disk, for the direct and indirect measurements.
Discussion
Image Analysis
The L4-L5 and L5-S1 disks were amenable to assessment through the abdominal wall, in this thin cadaver, in addition to directly through the anterior longitudinal ligament. The defects in the disks were well depicted on the sonogram, and the Naish grading was matched between the longitudinal and transverse planes. While the grading by Naish was devised with reference to canine cadaveric intervertebral disks, it was also noted to be applicable for human cadaveric intervertebral disks.
The visual assessment of the disks was subjectively better through the direct method compared with the indirect method. Although the Naish grading was the same for both methods, the small inclusions in the disk were depicted with better clarity through the direct method. This was especially noticeable in the transverse plane, as the disk fills the imaging field of view. The detail of the posterior annulus, of the disk, was better appreciated with the direct method versus the indirect method. This would be expected, as there is attenuation of the ultrasound beam by the abdominal wall musculature and less acoustic energy available to provide detail of deeper structures when imaged transcutaneously.
The transverse MRI images, of the disks, were of limited value and had poor correlation with the transverse sonography images. This was accounted for by the limits of spatial resolution of the acquired MRI images (4 mm slice thickness in a disk that is around 10 mm thick) versus the spatial resolution of sonography which is often submillimeter and dependent on the technical specifications of the transducer and settings. 8 The use of MRI to assess human cadaveric disks has been previously reported in the literature, with MRI being shown to provide a good assessment of degenerate disks. 9 The sagittal, or longitudinal, plane has been reported to be better than the axial plane for assessing the disks with MRI, also shown in our study. There was better agreement between the defects seen in the longitudinal (sagittal) MRI plane and longitudinal sonographic images compared with the transverse/axial planes. The greater spatial resolution of sonography compared with MRI allows the disks to be assessed well in both the longitudinal and transverse planes.
The disks in this 67-year male cadaver were degenerate, as shown by Pfirrmann grades 3 and 4 as assessed by sagittal plane T2 MRI and the Naish score. This is not unexpected, given the age of the patient. Potentially, if the disks were better hydrated with greater height, sonography may show even more detail of the internal structure.
The trapezoidal technique was frequently used in the gray-scale sonographic images to optimize the visualization of the disk. As found in other convex structures, such as the infant hip, this study did not find any degradation of image quality as compared with linear imaging. 10
The main clinical application of sonography of the disks is intraoperative assessment. This study demonstrated that disks can be accurately assessed via the direct method, and this was achieved through a surgical access approach for an anterior lumbar interbody fusion. This anterior approach is well established for lumbar spinal interbody fusion surgery or lumbar disk replacement, with indications including degenerative disk disease, spondylolisthesis, and correction of scoliosis.11–13 The anterior approach has advantages over posterior lumbar surgery as there is no breach of the paraspinal musculature, no resection of the posterior bony neural arch, and no manipulation of the cauda equina nerve roots and thecal sac. The risk of iatrogenic injury to these structures is thus greatly reduced. Intraoperative assessment of the disks can provide real-time sonography prior to any surgical intervention, which may be relevant if there has been a significant time delay between any preoperative MRI and the date of surgery. This could help guide the decision of which disks to surgically intervene with or, potentially, help the surgeon assess how much of the disk to resect in the case of a discectomy. Intraoperative MRI is established as a surgical guide in neurosurgery; however, it is expensive, is a scarce resource, and requires compatible anesthetic equipment. 14 This limits its use, especially in an orthopedic spinal center rather than a neurosurgical spinal center where intraoperative MRI is unlikely to be available. Intraoperative sonography has very few limitations compared with MRI. It is less expensive and more widely available; thus, it is well suited for intraoperative assessment of the intervertebral disks.
A further surgical approach that would allow direct placement of an ultrasound transducer on the intervertebral disk is the direct lateral, transpsoas approach, such as for an extreme lateral interbody fusion. 15 Although this approach was not explored in this cadaver study, it could potentially provide a similar acoustic window directly onto the intervertebral disk. This would broaden the clinical application of intraoperative sonography of the intervertebral disk.
Shear Wave Elastography Data
It was only possible to obtain consistent shear wave velocities from the anterior annulus fibrosus. The waves were attenuated in the deeper tissues and no shear waves were propagated. This is in agreement with previous studies.1–3
A statistical difference was found between the direct and indirect shear wave velocities at both the L4-L5 and L5-S1 disks. The indirect shear wave velocities were faster than the direct velocities, apart from the longitudinal velocity at the L5-LS1 disk. A recently published paper by this group assessing shear wave velocities in soft tissue tumors has shown the opposite trend, with the deeper lesions (equivalent to indirect) showing slower velocities compared with more superficial lesions (equivalent to direct), regardless of the histological type. 16 The same trend of slower velocities at greater depths has also been shown in other in vivo and phantom studies.17–20 The difference between the values according to the depth obtained in this cadaveric study and those previously reported could be explained by the stiffer nature of the cadaveric tissues compared with living subjects. The measurements taken at greater depth (indirect) also showed a greater variability compared with superficial measurements (direct), as shown by the greater standard deviation and interquartile range/median ratio for the indirect velocities compared with the direct velocities. The interposed tissues between the transducer and the disks are inferred to be exerting a nonuniform effect on the shear wave velocities, thus creating a greater spread of velocities and rendering them less consistent and potentially less reliable. The increased variability of measurements at depth can also be attributed to a lesser shear wave signal to noise ratio the greater the measurement depth.
Phantom studies have shown a significant effect on the measured velocities dependent on the stiffness of the tissue, with stiffer tissues showing greater variation in measurements. The diameter and volume of the tissues have also been shown to have an effect on the measured shear wave velocity, with spherical inclusions of the same known stiffness showing a variation in velocity dependent on diameter and volume.21,22 The disks in this cadaver were very degenerate, with reduced height, loss of the normal fibrillar pattern, and irregular inclusions, all of which are likely to influence the shear wave velocities and render them unreliable.
An in vivo study of cervical intervertebral disks in adult humans has shown that it is possible to obtain shear wave velocity measurements from the anterior annulus fibrosus from a transverse, transcutaneous approach at C6-C7 and C7-T1. 3 The average shear velocity in this group was 3.0 m/s, correlating with the subject’s age and body mass index. A study looking at the lumbar intervertebral disks in adolescent females has shown it to be possible to obtain shear wave velocities from the L4-L5 and L5-S1 disks, 1 with average velocities of 2.9 m/s. A study comparing lumbar intervertebral disks in scoliotic and nonscoliotic females has shown a velocity of 3.5 m/s in the scoliotic lumbar disks and 3.0 m/s in the healthy control group. 2 The equivalent values in the study cadaver (indirect/transabdominal measurements) are 4.6 m/s at L4-L5 and 5.3 m/s at L5-S1. Thus, the velocities in living human disks are generally less than those in cadaveric human intervertebral disks, most likely explained by the difference in stiffness of cadaveric tissues versus living tissues. A similar, relatively fast velocity (5.3 m/s) has been shown in cadaveric oxtail disks, 23 further suggesting that cadaveric disks are stiffer and give rise to faster velocities than living disks.
There was no correlation between longitudinal and transverse shear wave velocities at either disk in the study cadaver, for both direct and indirect measurements. This is in contrast to the data within soft tissue tumors, recently published by this group, which show a strong correlation between the transverse and longitudinal measurements. 16 The intervertebral disks have anisotropic properties, with different propagation of the shear waves according to the insonation angle. The disks in this cadaver were degenerate, with reduced height, loss of the normal fibrillar pattern, and irregular inclusions. These factors are likely to influence the expected effects from tissue anisotropy and negate any uniform effect, thus destroying any potential correlation, such as one may expect to see in young, healthy living disks.
The adjacent anatomic structures could also potentially be influencing the velocities according to the imaging plane. In the longitudinal plane, the disk is imaged as a small structure between two vertebral bodies. The intact cortex of the bone is a strong reflector of sound, which may give rise to in-plane wave reflection and altered velocities of the shear waves. 24 This effect is likely to be less in the transverse plane, where the disk fills more of the imaging field of view and the in-plane wave reflection is expected to be less.
The shear wave velocities obtained from the intervertebral disks in this cadaver are best regarded as preliminary results and baseline measurements for future studies. The variability in the data and the lack of consistency with in vivo studies mean that further research is required before shear wave sonography of the intervertebral disks is clinically useful. The main future direction that is posed is for sonography of the lumbar disks in living subjects and to ascertain whether shear wave velocities are correlated with disk degeneration. If this were implemented, it could provide a quantitative sonographic measurement of disk degeneration. This would be useful for clinical follow-up of patients and potentially replacing MRI in longitudinal research studies. This cadaveric study has shown that it is technically feasible to obtain the intervertebral disk shear wave velocity measurements for future research.
Limitations
The main limitation of this study was that the data were derived from a single, slim cadaver with metastatic disease. This potentially restricts how applicable the results are to cadavers with a higher body mass index and to living subjects, many with greater body mass index and free from metastatic disease. The tissue properties of a cadaver are also likely to be different from a living subject, thus limiting how generalizable the results are to a patient population.
There are many imitations of using sonography to assess the lumbar disks. The greatest obstacle is obtaining an adequate acoustic widow. In live subjects, the anterior acoustic window is difficult owing to overlying bowel gas and adipose tissues. Previous studies have shown that it is possible to obtain an acoustic window scanning anteriorly at the level of aortic bifurcation in adolescent female patients with a normal body mass index. 2 Many patients have an elevated body mass index, limiting the usefulness of sonography. Given the high prevalence of obesity in many countries throughout the world, this potentially restricts the generalized use of sonography to assess the lumbar intervertebral disks. In patients with gas-filled intestines, it may not be possible to obtain any acoustic window scanning anteriorly. In this cadaver, it was only possible to obtain an anterior acoustic window at L4-L5 and L5-S1, with the more proximal disks being obscured by gas in the bowel. It was further complicated by interposed anatomic structures which attenuated the beam.
The bony cage of the spinal canal, to protect the spinal cord, means that a posterior acoustic window to the disks is difficult to obtain. A preliminary study showed that it was possible to assess the disks using a 3.5-MHz transducer, from a posterolateral approach. 4 A high-frequency transducer is unlikely to penetrate through the paraspinal musculature and show the required detail of the internal structure of the disk. In the study cadaver, the disks could not be visualized from a posterior approach with either a 9-4 MHz or a 3.5-MHz transducer. This is likely to be because the bony spinal canal was degenerate, with osteophytes and other regions of bony hypertrophy obscuring any potential window through the interlaminar space.
Using both direct and indirect methods, the fibrous nature of the disks attenuated the acoustic beams and gave rise to acoustic shadowing at the posterior margin of the disk and limited assessment of the deep nucleus pulposus, as well as the posterior annulus fibrosus. No shear wave measurements were obtainable from most of the nucleus pulposus and the posterior annulus fibrosus. Thus, a large proportion of the disk could not be assessed with shear wave elastography, thereby reducing its utility.
The depth measurements for the shear wave velocities within the disk were recorded from the anterior margin of the disk, on an assumption of a uniform spread of ROIs. The difference in placement of the ROI between each disk may potentially have introduced error into the measurements through nonuniform ROI distribution. There is also a small area (up to 5 mm) at the most superficial aspect of the disk where it was not technically possible to obtain any measurements, thus potentially introducing error. This was apparent in the direct measurements, where the transducer was around 3 mm away from the disk (the thickness of the anterior longitudinal ligament), but not the indirect measurements.
Adjacent strong acoustic reflectors, namely the cortex of the vertebral bodies, can introduce error in the shear wave velocities. This effect is particularly apparent when scanning in the longitudinal plane of the disk where there are likely to be more reflected shear waves. This would be compared with imaging in the transverse plane where the in-plane reflected shear waves are likely to be fewer.
Accurate assessment of the levels can be challenging with sonography of the disks. In this study, the level was ascertained with reference to the sacrum. The anterior bony cortex of the sacrum can be seen on sonography as a continuous echogenic line from which the vertebral bodies and disks can be counted. Other methods used are to identify the bifurcation of the aorta and assume this is at the L4 level; however, this may be less reliable owing to variations in anatomy. Transitional lumbosacral anatomy can hinder accurate level assessment with sonography, unless there is a “roadmap” of the anatomy, such as a radiograph or MRI. The study cadaver had an MRI “roadmap” to aid in the localization of the levels, thereby reducing a potential source of error.
A variation has been shown in recorded measurements dependent on the transducer pressure applied by the operator. This is shown to be less in shear wave elastography compared with strain elastography; however, it may still introduce variation and potential error in measurements.18,25,26 To minimize this, a consistent light transducer pressure was used by the operator.
Differences in shear wave velocities can be found within the same ultrasound equipment and different transducers. 27 Error can also be introduced by variations in repeatability of measurements made by the same interpreting physician and between interpreting physicians. 20 To limit this, the same operator, ultrasound equipment, and transducer were used for all measurements. The consequence of this in this study was that there are no data to measure interobserver variation. The authors have not included any statistical measurements or interobserver data for the visual grading of the disks and comparison with MRI. This was a proof-of-concept study, and the data set is too small to allow any meaningful numerical statistical tests. Please review Figures 5–8 to determine possible conclusions.
Conclusion
Sonography can show the internal structure of the intervertebral disk with better detail than MRI. This was especially true when the transducer was placed directly on the anterior longitudinal ligament and in the transverse plane. Defects within the disk are clearly visualized on sonograms, as compared with MRI. These conclusions have the potential for enabling intraoperative sonography of the disks as a real-time surgical diagnostic tool.
Shear wave elastography is to be used with caution in cadaveric intervertebral disks, acknowledging the many confounding factors influencing the measurements. Further research is needed in living subjects to assess the feasibility and utility of in vitro sonography of the intervertebral disk.
Footnotes
Appendix
Acknowledgements
Thanks to Ceri Worthington and Dawn Collins, Senior Radiographers, for their assistance in obtaining the MRI images of the cadaver. I would like to thank Mr David Jaffray, Consultant Orthopedic Spinal Surgeon, for his expertise in dissecting the cadaver. I would also like to thank Mr David Adams, Head of the Anatomy Lab, for his practical assistance.
Ethics Approval
The study was approved by the Institutional Research Board of the host institution.
Informed Consent
Not applicable in this cadaveric study. The cadaver was used in accordance with the Human Tissue Authority rules for the UK.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were involved in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Trial Registration
Not applicable.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.