
Abstract
Objective:
A placenta accreta spectrum (PAS) refers to a condition in which there is an abnormal penetration of the placenta, within the walls of the uterus. This study was designed to assess the overall diagnostic accuracy of sonography in detecting myometrium invasion of the placenta, in pregnant women with placenta previa (PP).
Materials and Methods:
In this study, 70 participants were placed into groups with either an anterior placenta (APL) or a posterior placenta (PPL). An experienced radiologist examined the participants. At least two well-known diagnostic sonographic signs were considered, as the diagnostic criteria of PAS.
Results:
Sonography diagnosed 30 cases of PAS out of 43 confirmed cases, with a sensitivity of 70%, specificity of 77%, positive predictive value (PPV) of 83% and negative predictive value (NPV) of 61%, accuracy of 72.8%, precision of 69.1%, diagnostic odd ratio (DOR) of 21.06, and an F measure of 0.71. Detection rates were higher in cases of the APL (sensitivity: 78%, specificity: 91%, PPV: 94%, NPV: 68%, accuracy: 82.8%, precision: 78.2%, DOR: 39.12, and an F measure: 0.78). The review of sonograms allowed for the detection of seven cases (10%) of PAS appropriately.
Conclusion:
The sonographic results seem to be more accurate among individuals with APL than PPL. A replication of this study, with multicenter participation is recommended, especially in cases of PPL.
Keywords
A complete placenta previa (PP) is defined as placenta that covers the internal orifice of the uterus (IOU). When the placenta is a distance of less than 20 mm, it is considered a low-lying placenta while a placental distance equal to or greater than 20 mm is considered normal.1,2 Conversely, the placenta accreta spectrum (PAS) may be associated with a PP, as a pathology. This occurs when the placenta penetrates within the uterine wall. 3 PAS divides into three subtypes based on the intensity of penetration, known as acerta, increta, and percreta, respectively. 4 The placenta attached to the myometrium is characteristic of a grade 1, while, in the second and third grades, it is considered invasive. The increta invasion is limited to the myometrium; however, in percreta, the depth of penetration goes beyond and involves the surrounding organs.4 –6 There are several risk factors for PAS, which are patient history of Cesarean section (C/S), dilation and curettage, myomectomy, ectopic pregnancy, endometrial ablation, pelvic radiotherapy, age over 35, multiparity, manual placental deletion in previous pregnancies, and infertility-related procedures.6 –9
Hemorrhagia and disseminated intravascular coagulation, respiratory distress syndrome, renal failure, and death are all considered major complications of PAS.6,10 A study involving 7001 pregnant women, diagnosed with PAS, determined that there was an association with hysterectomy in 52.2% of participants, of whom 46.9% required packed red blood cells, due to severe hemorrhagia. 11 Damage to the adjacent viscera was among the adverse effects of PAS that could cause hematuria and was observed in 31% of a study of PAS cases. 12
The prevalence of PAS has increased in recent decades. 13 In the 1950s, with the United States, the prevalence of PAS was reported at 30 per 10 000 pregnancies, which increased to 170 per 10 000 pregnancies in 2019.11,14,15 In a regional study, between 2012 and 2016, the prevalence of the PAS in candidates for non-emergency C/S, PAS was reported at 1774 per 10 000. 16 The combination of PP along with the history of C/S has been considered the most important PAS risk factor. In the case of a primary C/S, the risk is 3%; however, a third C/S increases the risk of PAS by 40%. 13 The use of C/S has increased rapidly in the last decades. The prevalence of C/S, within Iran, has been reported as 48% and a prevalence of 90% in some private centers, compared with the ideal rate of 10% to 15% based on the World Health Organization recommendations.17,18
A transabdominal sonogram is the first diagnostic choice for clinical follow-up during a pregnancy. Sonography is also the first diagnostic alternative for detecting both PP and PA. The use of transvaginal sonography has improved the near-field resolution, which has been promising among individuals with PP or posterior placenta (PPL). 19 An interpreting physician relies on the loss of the retro-placental (clear zone), decreased myometrial thickness < 1 mm, interruption of the interface between bladder and the uterine surface, presence of abnormal placental lacunae, and placental outgrowing or bulges distorting adjacent organs to detect PAS with grayscale sonography. The use of color Doppler is helpful in detecting abnormal utero-placental blood flow that bridges vessels crossing placenta and uterine margin and turbulent flow in placental lacunar (feeder vessels). 20 Magnetic resonance imaging (MRI) also identifies PAS with high accuracy, especially in the case of sonographic limitations.21,22
This study was designed to assess the diagnostic accuracy of sonography in detecting PAS, among participants with PP. An investigation across different published studies, based on the diagnosis of PAS, resulted in many only considering anterior placenta (APL) with a noticeable lack of attention to the PPL.1,23 –26 Consequently, this study was prospectively designed with two group participants that were at risk for APL and PPL.
Materials and Methods
Study Design and Participation
Prospectively, 70 participants were enrolled in the study which followed pre-established inclusion criteria. A previous history of C/S along with the presence of documented PP after 28 weeks’ gestation was considered a main inclusion criterion. Conversely, participants were excluded if there was a history of any chronic diseases, pelvic surgery, and any complications during a recent pregnancy. In addition, those with an equal IOU distance from the anterior and posterior edges of the placenta were excluded. Ethical approval was received from the host hospital’s internal review committee. An oral and written informed consent was obtained from each of the participants. The participants were divided into 35 cases with APL and 35 cases with PPL. Placental location was characterized regarding the location of placental bulk and maximum distance of placental edges to IOU. It was important to note that a radiologist diagnosed either a PP or low-lying placenta, prior to the study. The sonographic findings were compared with the histopathologic results after surgery and surgeon’s description, which was based on the International Federation of Gynecology and Obstetrics (FIGO) classification for the clinical diagnosis of PAS disorders.
Diagnostic Imaging
The sonographic examinations were performed on an Aloka Prosound SSD 3500 ultrasound equipment system (Hitachi Healthcare Manufacturing, Ltd). A 2 to 6 MHz curvilinear transducer and a 3 to 7.5 MHz transvaginal transducer were used to examine the patients. An experienced and qualified radiologist performed the grayscale sonogram, the transvaginal ultrasound (TVUS), as well as the color and power Doppler examinations. The radiologist had over 10 years of experience in women’s imaging. The data collection began with a grayscale sonographic examination to survey the adjacent organs, then duplex scanning that included color Doppler helped to detect signs of PAS. Note that the transabdominal sonograms were acquired while the participant had a full urinary bladder, and for the TVUS, the participants were asked to empty their bladder. The ultrasound equipment’s electronic cursors were used to determine the distance between the IOU and the placenta for PP detection and the overlying myometrial thickness, to make a PAS diagnosis. The loss of the retro-placental (clear zone), decreased myometrial thickness < 1 mm, interruption of the interface between bladder and the uterine surface, presence of abnormal placental lacunae, and placental outgrowing or bulges distorting adjacent organs were used as diagnostic signs (see Figure 1). Likewise, color Doppler abnormalities such as abnormal utero-placental blood flow, bridging vessels crossing placenta and uterine margin, and turbulent flow in placental lacunar (feeder vessels) were used as additional diagnostic sonographic signs (see Figures 2 and 3). These signs have been suggested by the European Working Group on Abnormally Invasive Placenta (EW-AIP) and the AIP international expert group.20,27 As soon as one diagnostic finding was detected, additional diagnostic features were collected to strengthen the final diagnosis. As part of the diagnostic grading system, it was determined that two or more findings would be suggestive or conclusive for PAS, as well as sufficient to enroll the participant. When observing exophytic, bulging zones, or direct invasion of adjacent organs (i.e., bladder, vagina), the participant’s case was classified as a placenta percreta.

A grayscale sonogram, sagittal view, is provided and demonstrates a loss of bladder-uterine interface and bulging (see white arrow) of the placenta.
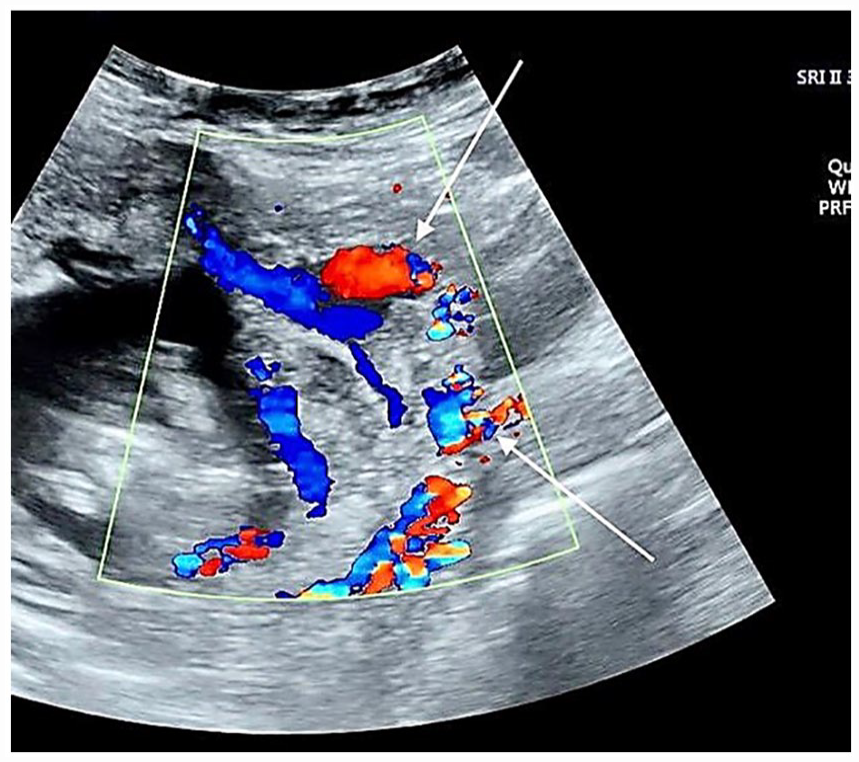
A color Doppler sonogram, sagittal view, is provided that demonstrates the turbulent flow (upper white arrow) in lacunar “feeder vessels” and presence of bridging vessels (lower arrow).
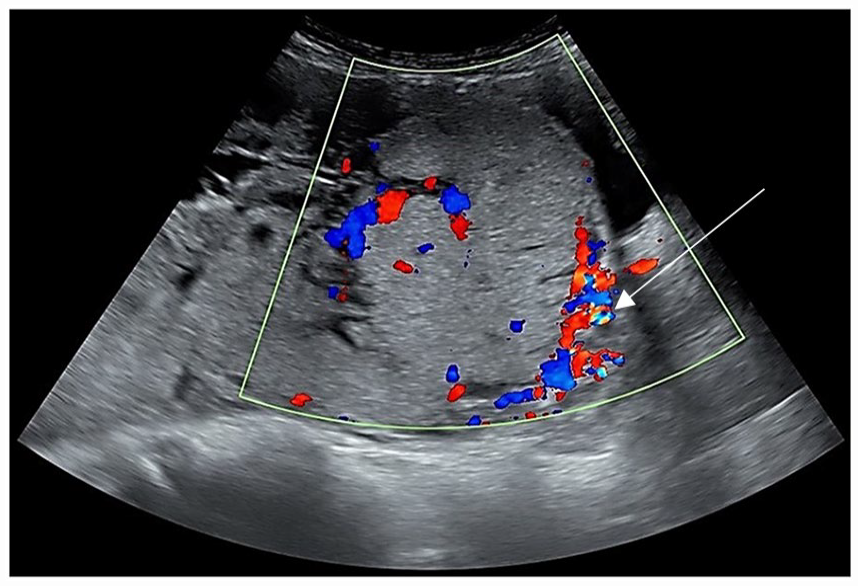
A sagittal transabdominal sonogram is provided and shows a posterior placenta accreta. Color Doppler is applied and demonstrates the increased vascularity at the lower uterine segment and uterus-bladder interface (see white arrow) in this case of posterior placenta previa. Loss of retro-placental “clear zone” and myometrial thinning are also noted in this region.
Statistical Analysis
The overall sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), accuracy, precision, positive likelihood ratio (LR+), negative likelihood ratio (LR–), and F measure were calculated. The same values were also calculated for cases of APL and PPL separately. The study variables were expressed as means with positive or negative standard deviations (± SD), and frequencies were measured as a percentage (%). The associations among the quantitative variables were calculated using t test. Pearson χ2 test was used for qualitative variables. The Statistical Package for the Social Sciences (SPSS) software (IBM, SPSS Inc.), version 22.0, was used. The statistical significance was set at P < .05 a priori.
Results
Seventy pregnant women were enrolled in the study who had a documented history of a previous C/S. The mean age of participants was 31.4 ± 4.86 years (20–42). The mean of gravidity was 2.93 ± 1.01 in a range of 2 to 6. The mean parity was 1.63 ± 0.73 in a range from 1 to 4. All participants had been diagnosed with PP, prior to enrolling in this study. The data collection continued until the number of participants reached 35 equally in both APL and PPL cohorts. Complete PP was present in 28 (40%) and low-lying placenta in 42 (60%) participants.
The study variables included the participant’s past medical history, sonographic findings, and pathologic outcomes after surgery. The results of these variables were compared with each other after dividing participants into two groups of the APL and PPL. There were 34 participants (48.6%) who had no positive sonographic signs of PAS, However, following surgery, the number of participants without PAS decreased to 27 (38.5%). There were 25 individuals (35.7%) who showed two or more diagnostic positive sonographic signs of PAS. Eleven individuals (15.7%) were diagnosed as placenta percreta, due to bulges or exophytic zones or invasion to other organs. Of these participants, five were anterior and six were posterior, in location. There were no statistically differences for any of the variables in the two groups, APL and PPL; an exception was noted for placental locations in proportion to IOU. A low-lying placenta was more frequently noted in the APL group (P = .03). Twenty-seven individuals (38.6%) had no histopathologic evidence of PAS after surgery. Grade 1 and 2 FIGO classifications, for PAS (accreta and increta), were present in 21 cases (30%), and a FIGO grade 3 classification was assigned for PAS (percreta) in 22 cases (31.4%). There was a need to perform a total or subtotal hysterectomy in 23 cases (32.9%), due to severe hemorrhage or placental invasion. A FIGO classification grade 3b (penetration into the bladder) and 3c (placental penetration to the vagina) was also present in 11 (15.7%) and 3 (4.3%) cases, respectively (see Table 1).
The Clinical Characteristics, Medical History, and Sonographic and Surgical Findings of 70 Participants.
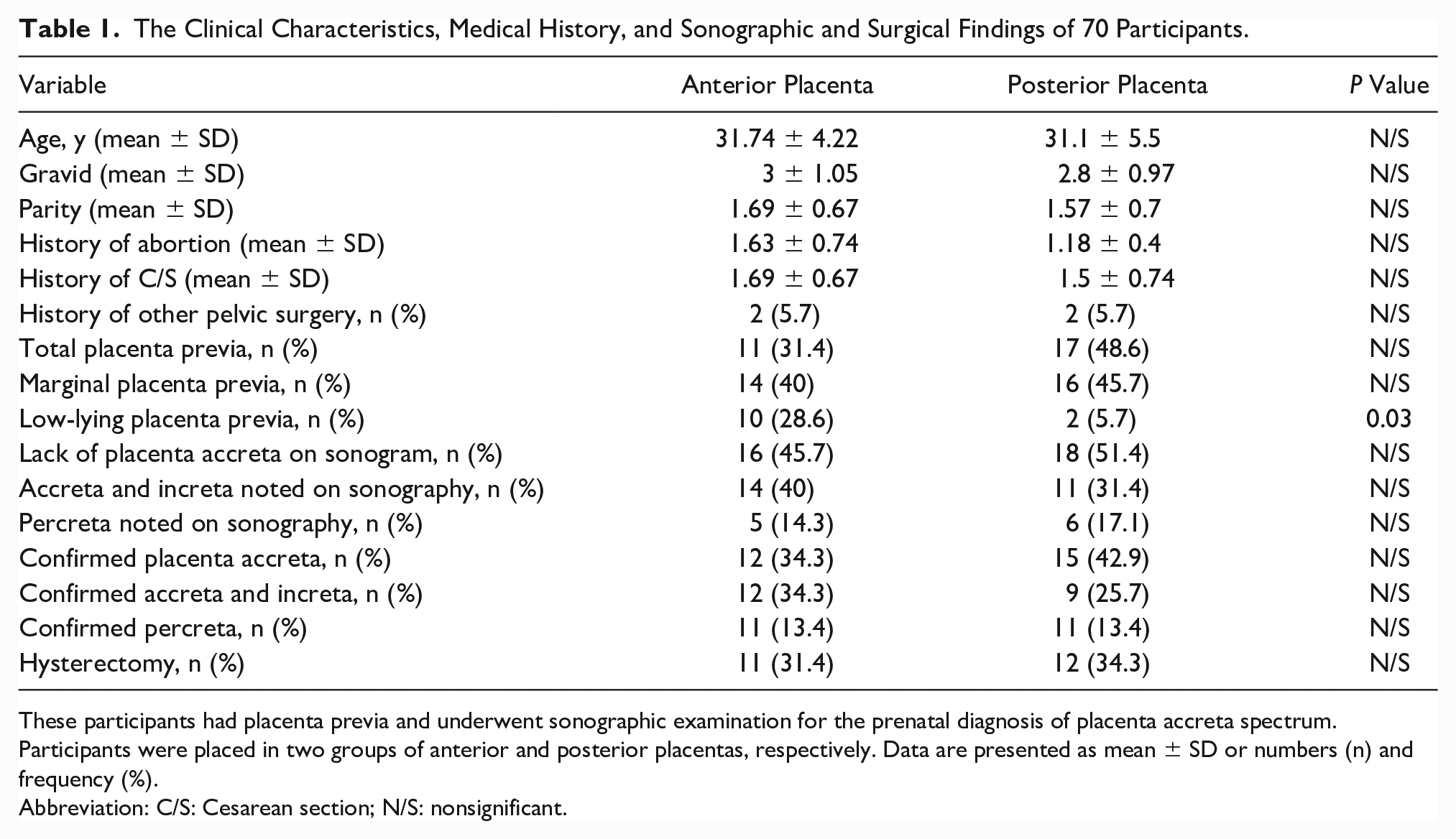
These participants had placenta previa and underwent sonographic examination for the prenatal diagnosis of placenta accreta spectrum. Participants were placed in two groups of anterior and posterior placentas, respectively. Data are presented as mean ± SD or numbers (n) and frequency (%).
Abbreviation: C/S: Cesarean section; N/S: nonsignificant.
The sonographic examination was successful in diagnosing 30 of 43 PAS cases, which were confirmed postsurgically. These results demonstrated a sensitivity of 70%, specificity of 77%, accuracy of 72.8%, precision of 69.1%, PPV of 83% and NPV of 61%, diagnostic odd ratio (DOR) of 21.06, and F measure of 0.71 for sonography. Notably, considering the placental location, these were better observed in cases of APL compared with PPL (see Table 2).
The Accuracy of Sonographic Examinations Based on the Prenatal Diagnosis of Placenta Accreta Spectrum, in Patients With Placenta Previa.
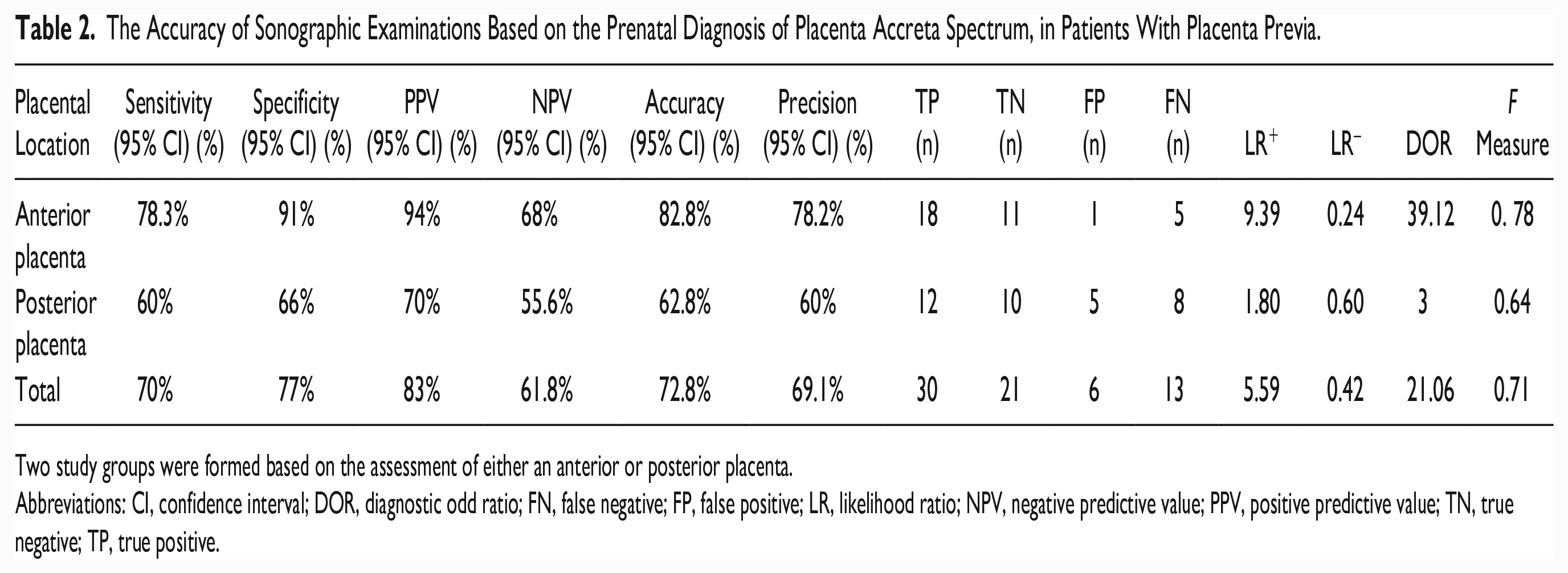
Two study groups were formed based on the assessment of either an anterior or posterior placenta.
Abbreviations: CI, confidence interval; DOR, diagnostic odd ratio; FN, false negative; FP, false positive; LR, likelihood ratio; NPV, negative predictive value; PPV, positive predictive value; TN, true negative; TP, true positive.
The sonographic examination failed to detect seven cases (10%) of PAS, most of which showed one or no detectable criteria, thus lowering the diagnostic suspicion. Twenty-two of 43 surgically positive cases were diagnosed as FIGO classification grade 3 for PAS (percreta) and 21 cases as grade 1 and 2 FIGO classification for PAS (accreta and incerta). All the confirmed percreta cases were diagnosed as increta or percreta, by sonography before surgery. However, only half of the percreta cases had been diagnosed correctly as percreta, prior to surgery.
Discussion
A diagnosed PAS, at the proper time, allows for planning a suitable delivery management and may prevent serious complications. This prospective study followed 35 participants with APL and 35 participants with PPL to delivery and postpartum. Afterward, the sonographic results were compared with the histopathologic results, postsurgically and the surgeon’s report. It was important to note that participants who had two or more PAS sonographic diagnostic signs were consented for study. Other published studies have used the presence of at least two sonographic signs as diagnostic for PAS.28,29 Pilloni et al. 29 used the “two diagnostic criteria system” to confirm the presence of PAS and reported a sensitivity of 81.1%, specificity of 98.9%, PPV of 90.9%, and NPV of 97.5%. They were able to reach an acceptable compromise between sensitivity and specificity using this diagnostic system. 29 Similarly, the current study used the same diagnostic criteria to classify and group the participants.
The diagnostic value of sonographic findings was variable. Shih et al. 30 reported the “numerous coherent vessels sign” as having the strongest diagnostic value, which was made possible by using 3D power Doppler. Shi et al. 31 reported the “multiple lakes” and “interphase hypervascularity” detected by grayscale sonography and color Doppler as the best diagnostic signs. Conversely, the presence of a large lacunae and thinning of the retro-placental myometrium was reported by Amirabi et al. 32 as the strongest signs for a PAS diagnosis. Bowman et al. 33 considered placental lacunae abnormalities, retro-placental space, and color Doppler as representative of truly positive diagnostic cases. However, in the current study, the cumulative variables and the sonographic results were suggestive or conclusive for PAS, rather than evaluating the diagnostic accuracy of each single sonographic study finding.
The sonographic sensitivity and specificity, for the diagnosis of PAS, vary widely based on previously published studies. It has been reported, between 1992 and 2020, that sonographic diagnoses varied between 33% and 100%, and 50% and 98.8%, respectively.34 –39 A meta-analysis of 23 published studies found an overall sensitivity of 90.72%, specificity of 96.94%, and DOR of 98.59, based on the prenatal diagnosis of PAS with sonography. They also reported on the abnormality of the interface between the bladder and uterus, had the highest specificity for detection of PAS. 25 In addition, they found that color Doppler had a sensitivity of 90.74 %, specificity of 87.68%, and DOR of 69.02, which introduced an added technique with high diagnostic accuracy. 25 Garofalo et al. 39 completed a retrospective investigation of 198 pregnant women with PPL and reported a sensitivity of 60% and a specificity of 98.8%, based on the diagnostic value of sonography, for those diagnosed with PPL. The results of the current study showed an overall sensitivity of 70% and a specificity of 77%, for the diagnosis of PAS. Meanwhile, when specific attention was paid to the cases with APL, the current results displayed a higher accuracy rate with a sensitivity and specificity of 78% and 91%, respectively, for APL. This is in comparison with the current study data that showed a sensitivity of 66% and specificity of 66%, for PPL. These results exhibit the efficiency of sonography, as the diagnostic choice for APL. The pooled LR+ of 9.39 and LR– of 0.24 for APL cases would indicate that identifying PAS-positive individuals with sonography is 9.39 times more likely than not identifying them. Similarly, the pooled LR+ of 1.80 and LR– of 0.60 reported for PPL cases in the present study displayed the lower efficiency of sonography for PPL. Regarding the comparison of LR– in APL (LR–: 0.24) and PPL (LR–: 0.60) cases, it indicates a higher probability of finding true negative cases in APL than the PPL cases. Pagani et al. 40 reported a pooled LR+ and LR– of 38.4 and 0.147, respectively, as the diagnostic value for using sonography to detect APL. In the current study, sonography displayed its best performance in detecting placenta percreta. It is also important to point out that DOR also represented a higher diagnostic value for sonography in detecting APL (DOR = 39.12), compared with the PPL (DOR = 3). Furthermore, to create greater accuracy, the current study included the F measure. The F measure was an important indicator based on accuracy and precision. The F measure for APL and PPL cases was calculated as 0.78 and 0.64, respectively, which support the idea that despite a lower F measure in PPL, it was plausible to include in these cases as well. In the current study, 22 of 43 confirmed positive cases were identified as a FIGO grade 3, which represents a high prevalence. This may be due to the current study being performed in a referral center, which could have introduced a study bias.
Limitations
The major limitation to this study was the research design, which was based on a convenient sample of participants. Threats to internal and external validity, based on the design, precludes generalization of these results. However, these results are foundational for further studies in this regard. However, it may be important to design similar studies based on both MRI and sonography, especially in the cases of PPL (see Figure 4). A single-centered study that only included pregnant women in their third trimester was the other limitation of this study. By designing multicenter studies with a larger number of participants, as well as including participants in their first and second trimester with shortened follow-up intervals, it is possible to better determine the diagnostic accuracy of sonography, in the diagnosis of PAS.
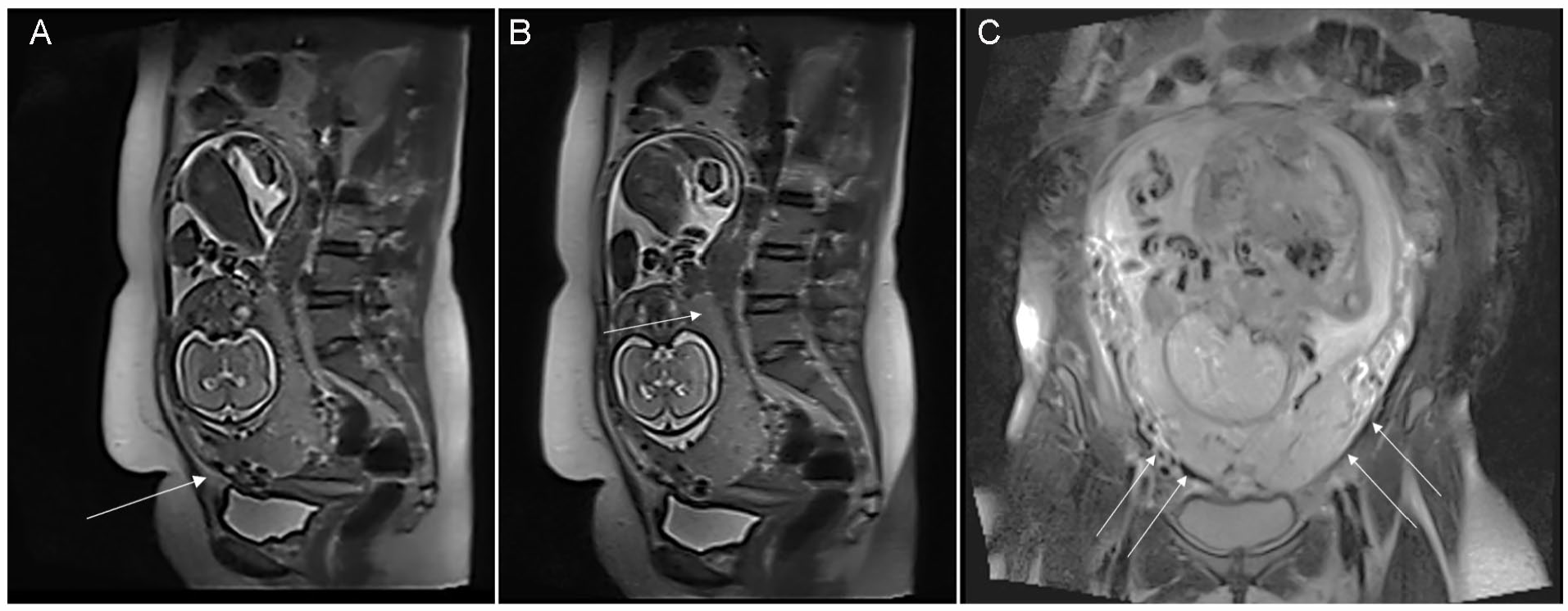
A magnetic resonance imaging (MRI) set of images demonstrates a posterior placenta accreta. (A) and (B) are a sagittal T2 Haste and (c) is a coronal T2 Fast spin echo sample image that demonstrates a 28-week gestation that shows multiple T2-hypointense (arrow) bands and placental heterogeneity (arrowhead) at the lower uterine segment. In cases where a thorough, sonographic evaluation is not possible, due to the posterior location of the placenta or patient obesity, MRI may be a better diagnostic choice.
Sonography is a very operator-dependent diagnostic modality which can be a limitation, and applied to these examinations, participants with only one positive sonographic sign or an inability to perform the examination due to a posterior placenta or large body habitus are all inherent challenges. Thus, an experienced and qualified examiner is needed to minimize these sonographic limitations, as much as possible.
Conclusion
Sonography is an efficient diagnostic imaging choice for perinatal evaluation and the detection of complications during pregnancy. The sonographic results used in the detection and diagnosis of PAS, for patients with APL, may be more accurate than in individuals with PPL. The replication of this study as a multicenter clinical trial is recommended and utilizing MRI in conjunction with sonography may be important, especially in cases of PPL.
Footnotes
Acknowledgements
We would like to express our gratitude to Al-Zahra hospital because of their kind contribution during this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by Tabriz University of Medical Sciences.
Ethics Approval
This study was approved by the local ethics committee of Tabriz University of Medical Sciences.
Informed Consent
All patients signed written consent notes for inclusion in potential observational studies prior to hospitalization.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because this study is on humans.
Trial Registration
Not applicable.