
Abstract
Keloid is a benign fibroblastic tumor that is most often secondary to tissue injury. The clinical presentation is a hard red or purple tumor, mostly itchy or painful. The clinical objectives are to report an ulcerated keloid secondary to a central or inner complicated epidermal inclusion cyst histologically proven and to describe the sonographic findings that permitted the diagnosis. A 29-year-old man with multiple large keloids on the chest wall presented with a two-day pain history, increased volume, and ulceration on one side. Physical examination showed a keloid with edema, peripheral erythema, and a 1-cm central ulcer with purulent discharge. On the sonogram, multiple solid dermal hypodermal pseudotumors were visualized. The lesions were well-defined hypoechogenic heterogeneous solid masses that were hypovascular with color Doppler, concordant with keloids. Within the ulcerated enlarged mass, a complicated epidermal inclusion cyst was discovered with inflammatory changes. The significance of this case lies in the very low frequency of ulceration of a keloid and the high diagnostic value of sonography to demonstrate the presence of a coexisting epidermal inclusion cyst. In the differential diagnosis of an ulcerated keloid, sonography can assist in achieving a better presurgical approach.
Keloid is a benign fibroblastic tumor that is most often secondary to tissue injury with abnormal skin healing1,2 and can occur spontaneously in individuals with black pigmented skin or a family history of keloid formation.1,3 The reported incidence of keloids in black and Hispanic populations has varied from 4.5% to 16%, with a mild predominance in women and a higher frequency in puberty and pregnancy. 4 Clinically, it is characterized as a hard red or purple tumor, which can be itchy or painful. It extends beyond the margins of the wound in the normal skin.1,3 It seldom resolves spontaneously, and the response to treatment is often poor or unsatisfactory.5,6 Currently, no publications of ulcerated keloids in the English literature have been reviewed. The ulceration of a keloid is a very rare condition.
Epidermal inclusion cysts, denominated epidermoid cysts or follicular infundibular cysts, are the most frequent type of cutaneous cysts.7,8 The cutaneous cyst has different classifications, but in general, the epidermal cyst is considered like a cutaneous adnexal cyst, depending on the infundibulum, 9 with an epithelial wall and granular layers and keratinization.8,9
High-resolution sonography (HRS) is an excellent imaging technique for examining the skin, soft tissue cysts, and tumors and generally is the first imaging study option for soft tissue masses.7,8
The objectives of this case report are to report an ulcerated keloid, secondary to an inner complicated epidermal inclusion cyst, and to describe the sonographic findings that suggested the diagnosis.
Case Report
A 29-year-old man with multiple large keloids on his chest wall secondary to acne came for consultation. This was due to a two-day history characterized by pain, increased volume, and ulceration in one of the keloids, accompanied by a fever of 38.5°C (101°F). Physical examination showed a keloid with edema, peripheral erythema, and an ulcer 1 cm in diameter with purulent discharge (Figure 1).

Thoracic wall keloid with edema, peripheral erythema, and an ulcer 1 cm in diameter.
A superficial structures sonogram was required by the dermatologist because of the ulceration. On HRS, multiple solid dermal hypodermal pseudotumors were visualized on the thoracic chest wall. The lesions presented on sonography as a regular elevated epidermis, with a well-defined hypoechogenic, heterogeneous, and solid dermal hypodermal mass (Figures 2 and 3). The lesions were hypovascular on color Doppler and concordant with keloids.
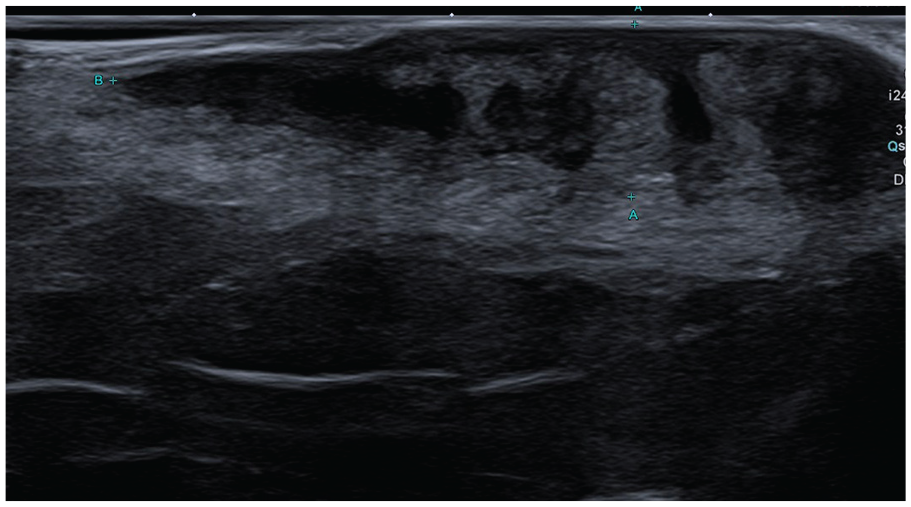
Thoracic wall ultrasonography. Well-defined hypoechogenic, heterogeneous, solid dermal hypodermal mass concordant with a keloid.
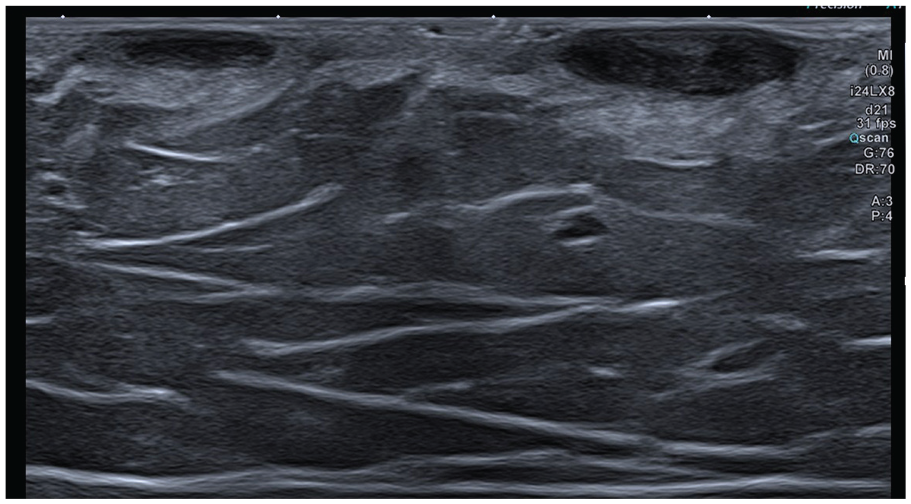
Two well-defined hypoechogenic, heterogeneous solid dermal keloids.
On the ulcerated enlarged keloid, a 20-mm cystic lesion was depicted. It was a bilobulated dermal hypodermal cyst (sandwich or shirt bottom shaped), heterogeneous, and partially anechoic, with hypoechogenic content. The contour was slightly irregular, with peripheral hyperemia. A prominent 5-mm punctum was observed in the middle of the lesion that crossed the dermis to the skin surface (Figure 4).
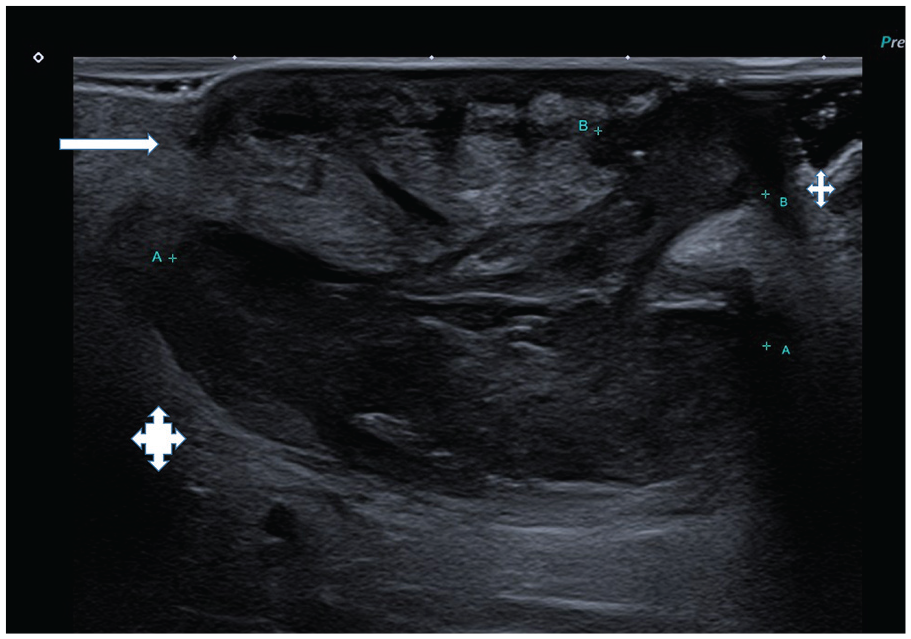
Ultrasonography of the ulcerated keloid with a predominant hypodermal cyst (A) in the keloid (white arrows). A prominent fistulized path in the middle of the lesion that crossed the dermis to the skin surface (B).
The subcutaneous tissue surrounding the lesion presented with an increased echogenicity and hyperemia, suggestive of inflammatory changes (Figure 5). The HRS diagnosis of a complicated epidermal inclusion cyst inside the keloid was determined.
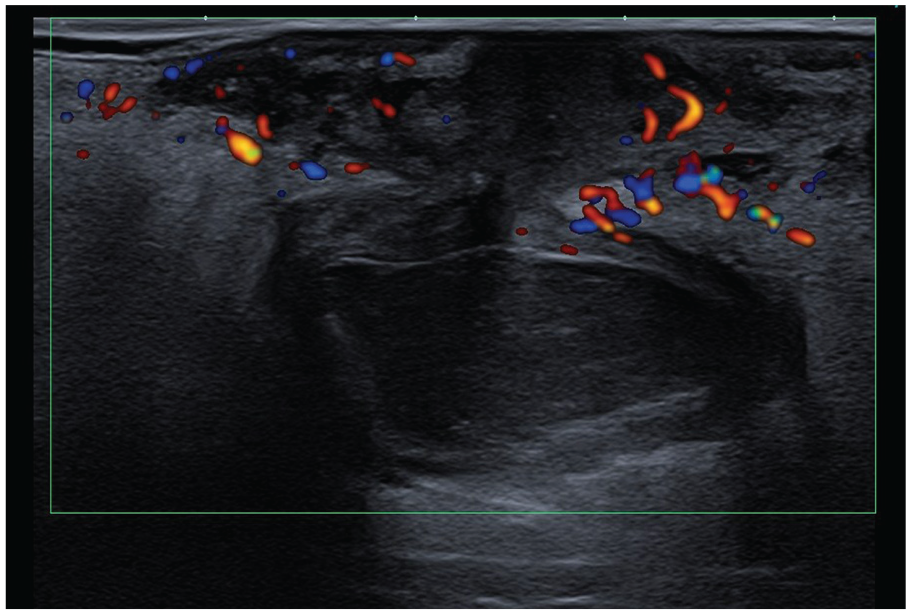
Increased echogenicity and hyperemia of the surrounding tissue suggesting inflammatory changes.
The culture of the ulcer showed the presence of multisensitive Proteus mirabilis. A 14-day regimen of cefadroxil 500 mg was indicated every 12 hours, and the patient was referred to plastic surgery specialists for complete keloid resection.
A skin surgical resection was made and the biopsy showed an epidermal inclusion cyst that was swollen and fistulized inside the keloid (Figure 6).
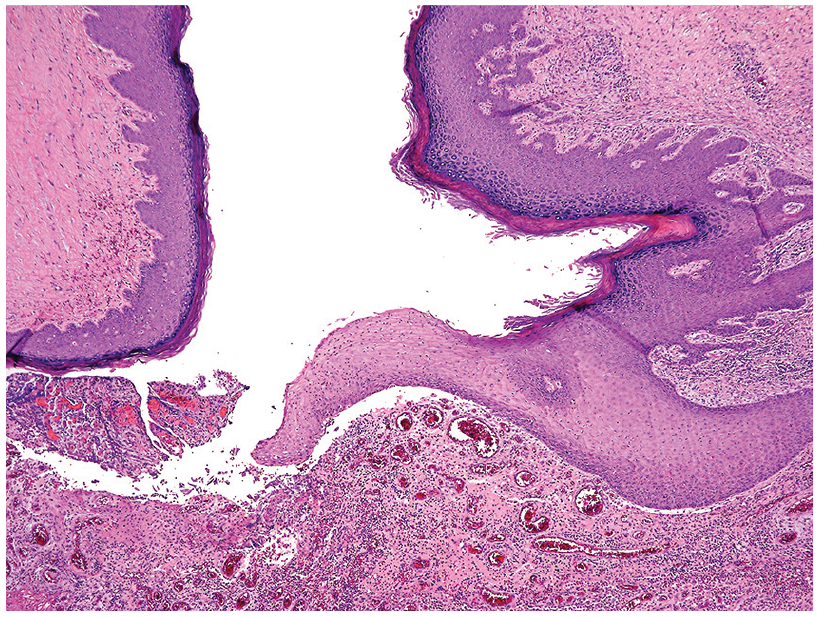
On histology, an infundibular cyst was confirmed.
Discussion
Keloidal tissue is a benign fibroblastic tumor most often secondary to a tissue injury and generally develops postsurgically beyond the margins of the scar.1,3 It apparently develops when the injury depth reaches the reticular dermis. 3 The clinical appearance is as a red or purple bulged dermal tumor, which can be painful or itchy. Also, cosmetic and functional problems can be present. 5 The ulceration of a keloid is rare.
The epidermoid cyst corresponds to a group of cutaneous adnexal cysts that originate in the follicle sebaceous unit. 9 The epidermoid cyst is the most frequent cutaneous cyst, 9 containing keratin and stratified epithelium. 8 The clinical presentation is variable, with slow-growth painless dermal or hypodermal cutaneous cysts with a central punctum (representing the plugged orifice of the pilosebaceous follicle), and typically appears in the head, neck, or anterior trunk.8,10
The existence of an epidermoid cyst inside a scar or keloid tissue is very rare, and only a few cases are reported in the literature. 11 Scars are a fibrous tissue with no skin appendages. This case of an epidermoid cyst probably had a posttraumatic origin. 11
The sonographic diagnosis of an epidermoid cyst included the presence of a cutaneous cyst located in the dermal, hypodermis, dermal, or hypodermal layers. The use of HRS helps the clinicians to study the cyst wall, internal content, and surrounding tissue. 12 Often it can appear as a heterogeneous cyst that had an anechoic peripheral rim, hypoechogenic content, and posterior enhancement. Some echogenic foci can also be present.8,12 It can be complicated with rupture or infection. Ruptured epidermal cysts have been reported in 21.3% to 38.0% of cases. 12 The presence of punctum is a characteristic finding. 8
In this case, the HRS revealed a complicated epidermal inclusion cyst on the ulcerated enlarged keloid, with important inflammatory changes. The radiologist observed a dermal hypodermal cyst, avascular in Doppler color, inside the lesion. A prominent punctum that crossed the dermis to the skin surface was also depicted.
An ulcerated keloid is a very unusual condition. In the differential diagnosis, dermatofibrosarcoma protuberans, squamous cell carcinoma, and basal cell carcinoma are mentioned, especially in cases that do not respond to treatment.13–16
Conclusion
The interest of this case lies in the very low frequency of ulceration of a keloid and a high diagnostic value of sonography to demonstrate the presence of a coexisting epidermal inclusion cyst. In the differential diagnosis of an ulcerated keloid, sonography can help us to achieve a better presurgical approach.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.