
Abstract
Work-related musculoskeletal disorders (WRMSDs) are a costly problem within the sonography profession, affecting health care organization bottom lines, sonographer satisfaction, and the patient experience. There is limited evidence regarding the limits of exposure to sonography examinations that would reduce on-the-job injury. This case study demonstrates the use of examination schedules that incorporate demand, length and difficulty level of examinations, staffing resources, and equipment availability, which may help to determine appropriate or maximum workloads for sonographers within their respective workplace. Developing a culture of prevention is a critical and cost-effective component of reducing WRMSDs.
Work-related musculoskeletal disorders (WRMSDs) are well known to affect sonographers primarily due to prolonged static postures, grip pressure on the transducer, and downward forces to complete certain scans.1–7 In Canada, WRMSDs are the largest single source of time-lost costs in many workers’ compensation systems. 8 In 2004, Muir et al. 9 reported that the direct cost to employers for an injured sonographer in Manitoba, Canada, was $120,038 CDN. In the United States, a sonographer injury could total in excess of $700,000 USD when factoring in direct costs for managing the injury along with indirect costs due to lost productivity or hiring of replacement staff. 10
Although there is an extensive and growing body of literature describing the prevalence of WRMSDs in sonographers, there is limited evidence regarding the limits of exposure to sonography examinations that would reduce injury. Specifically, more evidence is needed to establish a maximum transducer time, that is, the time a sonographer holds the transducer against a patient’s body. 4 Given that transducer time is directly related to the type and number examinations completed, sonographer scheduling is among the primary administration controls that may be targeted to moderate workload risk. 11 Despite limited empirical data, the National Institute for Occupational Safety and Health (NIOSH) provides general recommendations for scheduling ultrasound examinations to minimize injury risk. These include scheduling a variety of examination types to reduce the strain on specific sets of muscles, limiting the number of portable examinations, and establishing a maximum number of examinations per sonographer. 12
These recommendations are useful as a foundation, but implementation within the clinical context can be challenging. Unfortunately, exemplars are not readily available for administrators and sonographers on the specifics of reducing transducer time or the processes needed to establish examination schedules for sonographers. This article attempts to address this need by sharing a process for creating examination schedules that incorporate the demand for each examination type, the length and difficulty level associated with the examination type, staffing level, and number of ultrasound systems available. An industrial engineer was consulted for the project, who worked with the charge sonographer, a radiologist, and the bookings clerks. Together, the team gathered the necessary information, developed the scheduling process, and identified a means for monitoring and sustaining the new protocol. A description of each phase of the project follows.
Clinical Site Description
The ultrasound department in this exemplar exists in a tertiary care center that serves low-risk obstetric, gynecology, and pediatric patients in the region. In addition, there are neonatal and pediatric intensive care units on site. The sonography department has seven examination rooms and one portable ultrasound unit. The operating hours of the department are 7:30 to 17:00 Monday to Friday, with a total of 247.5 days of operation per year after subtracting weekends and statutory holidays. Sonographers are scheduled for 8 hours per day, including two paid 15-minute breaks and an unpaid 30-minute lunch break, resulting in 7 hours for scanning each day per full-time equivalent (FTE). During the year of the project, there was a total of 44.5 weeks (333.75 hours) of vacation owed to the sonographers.
At the time the scheduling project was carried out, there were 9.9 FTE sonographer positions. Of those 9.9 positions, one was the charge sonographer with a dedicated 0.5 FTEs to administrative work, and one sonographer was assigned to the position of “sorter” each day, bringing the total FTEs available for scanning to 8.4. The sorter position was designed to give each sonographer a full day away from scanning and thus incorporating the NIOSH recommendation of task rotation. Sorter duties included triaging and scheduling emergent and urgent patients, consulting with radiologists, answering the phone, and responding to patient questions. The sorter was also able to step in and assist with scans on unusually busy days or could be asked to scan all day in case of low staffing levels due to sick calls and vacations.
Gathering Information
Assess Demand
The Radiology Information System (RIS) was used to determine the total number of examinations that were performed during the previous year according to examination type. In addition to examination type, the team attempted to identify the frequency of emergent and urgent requests. Since sonographers are unable to carry a full outpatient workload as well as being expected to “squeeze in” emergent or urgent patients, it was important to ensure that the scheduling process allowed adequate room for these patients. Moreover, emergent cases are often the more difficult as patients are often limited in their ability to cooperate in positioning themselves and can be further complicated due to complex pathologies that can significantly extend transducer time.
Although the demand for emergent examinations could be captured as those sent from the emergency department, in actuality, emergent examinations were also requested from other sources within and outside the health center. To obtain a more accurate estimate of the daily number of emergent cases, the department kept track of all the emergent add-on cases using a handwritten ledger. The examinations logged in the ledger were compared to the examination totals found in RIS to identify the number of spots on the schedule that needed to be held open each day for emergent cases from within and outside of the center.
Urgent requests were more problematic to account for since these requests were targeted to be completed within three to seven days. It was difficult to determine which cases fell into the urgent category since they were generally booked as an outpatient with no distinguishing data to tell them apart from routine bookings. Subsequently, these types of examinations were left in the category of routine bookings, assuming that once the schedule was built proportional to the total number of each examination type required, there should be space left for scheduling urgent examinations within the three- to seven-day target.
In addition to gathering the total number of examination types and identifying the need for emergent care, the RIS data were used to determine the typical wait time for booking. To examine this need, lists of examination requests that had been received but not yet booked were identified within the “pending” area of the system. The health center uses the data from pending and tabulates wait time from the date an examination was pended until the examination was completed. These data are used to manage the wait time targets established by provincial and national authorities, ensuring that patients are seen in a timely manner and that no one is left waiting an unsafe length of time for their examination. To capture demand for all examination types, the data generated from pending were used to ensure that the scheduling process would meet the demand and target times across examination types.
Ascertain Average Examination Times
In addition to identifying the department demand, the approximate length of each examination type was assessed to ensure appointment times accurately reflected the turnaround time a sonographer required to complete the examination. This turnaround time included activities prior to engaging with the patient, such as a review of the requisition, review of pertinent prior examinations including information from other imaging modalities, and preparation of the examination room for the particular examination type. Time spent with direct patient engagement included patient assessment, patient positioning, and direct scanning. Additional time involved an initial image review, preparation of observation notes, image review with the reading physician, release of patient, and cleaning of the room after the patient departed.
Two methods were used to identify average examination lengths, including data from the Canadian Institute for Health Information (CIHI) and a time study. The CIHI is an independent, nonprofit organization that maintains databases and generates reports on Canada’s health systems. One of the many analyses that can be accessed through CIHI is the Medical Imaging Schedule of Unit Values. This schedule can be used to extrapolate appropriate length of time needed for each examination type. CIHI generates this information by accepting and analyzing data that had been gathered and submitted by numerous diagnostic imaging departments across Canada. These data were accessed and used to inform the project. 13
With the help of the industrial engineer, a time study was then carried out in the department to verify that the department was in line with examination times recommended by CIHI and to capture special protocols and unique examination types that may differ from the average CIHI data. All sonographers participated in the time study to account for differences in practice between sonographers. Forms initiated by the receptionist and completed by the sonographer were used to capture details of each patient visit (Figure 1). Descriptive information captured included the type of examination, room used, and the amount of time to complete the visit. Specific times were logged to characterize the flow of each patient through the visit, including when the patient arrived and exited, as well as the start and end times of preparation, sonographer examination, and radiologist review. The form also documented time associated with any add-on examinations or “other” time that was spent before the patient exited. Average appointment times were calculated for each examination type to identify appropriate sonographer turnaround time for the examination type. These times matched closely with the CIHI guidelines, and only a few examination types varied by ±5 to 10 minutes. 13
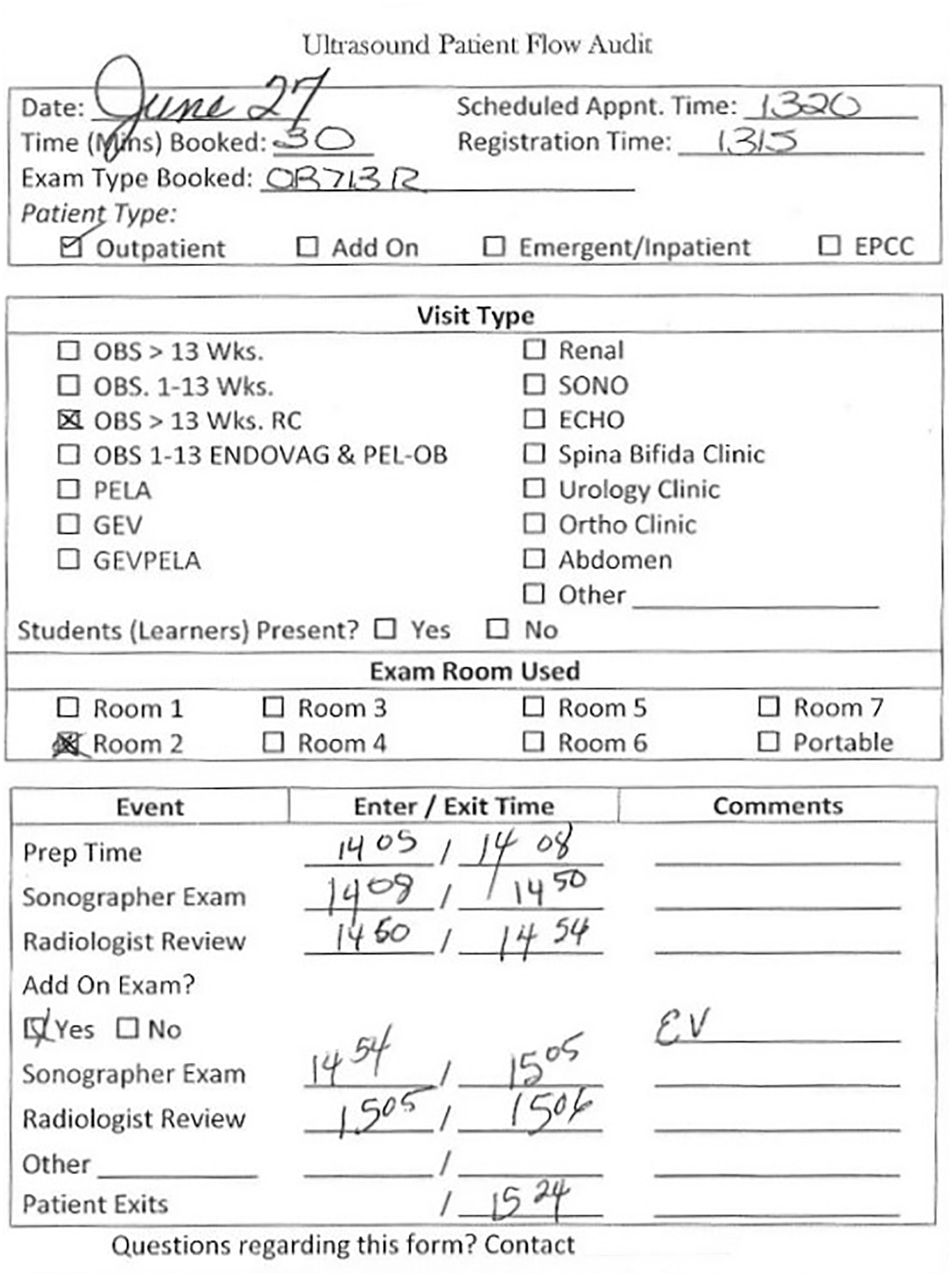
Example of a completed time study for a third-trimester obstetric examination that required an endovaginal examination to be added.
Develop a Weighted Examinations Rubric
In addition to identifying the department’s demand and average turnaround time per examination type, understanding strain and risk associated with individual examination types was a final component for consideration in developing a schedule for minimizing risk. Sonographers have experience and knowledge about the intricate aspects of each examination type and would be able to rank the “real-world” risk assessment for each examination. Thus, the sonographers in the department were asked to rank all the examination types completed within the department from high risk to low risk for WRMSDs.
Generally, those examinations with long total examination times carried the highest risk; however, there were exceptions. For instance, sonohysterograms required a one-hour appointment time, but the sonographer only scanned for the initial transvaginal portion while the radiologist performed the instrumentation required to insert the sonohysterogram catheter and scanned during the saline instillation. As a result, the sonographer had zero transducer time while assisting the radiologist during the majority of the examination, and the overall examination was deemed to be lower risk. Similarly, even though they were also one-hour appointments, pediatric abdomen examinations were assessed as low risk for WRMSDs due to the lower pressure needed on the transducer than with other examinations. Fetal echocardiograms were deemed to have the highest risk for WRMSDs, and pediatric hip examinations carried the lowest of all the examination types offered in the department.
Developing the Schedule
Outpatient Bookings Schedule
The outpatient bookings schedule was built using a spreadsheet for examination scheduling in six of the seven rooms. The seventh room, which was small with poor air quality and housed the oldest ultrasound system, was reserved for times when the workload was unusually high. Similarly, the portable machine was not on the outpatient bookings schedule; instead, this machine was only used for patients who were emergent add-ons or too sick to come to the department, as recommended by the Industry Standards for the Prevention of Work-Related Musculoskeletal Disorders in Sonography. 14
Using the time study, the rubric for risk of WRMSDs, and the demand assessment, a schedule was built for a two-week block. To begin, standing reserved appointment times for specific examination types were slotted to accommodate patients attending the various clinics that were carried out within the health center. For instance, urology, nephrology, and rehab clinics together reserved 128 renal appointments each month. The orthopedic clinic reserved 34 pediatric hip appointments each month. Each day of the week had a different ratio of examination types depending on which clinics were operating that day. The bookings schedule then ensured that appointment openings across examination types were varied, avoiding too many high-risk examinations in succession to minimize the chance any individual sonographer would end up with an exceedingly high-risk worklist.11,12
Numerous iterations were required before a final schedule was launched, a process that required time and patience. The most common failure in the process was running out of time within one day to fit in all the examinations required. It was important, then, to look at the week as a whole and find examination types that could be moved to other days in the week. Additional considerations in the scheduling process included examinations that required fasting, which were booked for the early morning hours. The initial schedule was developed by the most experienced booking clerk, followed by review by the lead sonographer. Multiple attempts were required to arrange the examinations so that the risk of WRMSDs was a low as possible considering all the constraints such as operating hours, staffing, emergent cases, and demand.
Sonographers’ Worklists
The outpatient bookings schedule did not reflect each sonographer’s personal workload for the day since there were more sonographers than examination rooms; therefore, it was difficult to analyze each sonographer’s workflow. It was important to balance the sonographers’ work/rest periods with patient flow. For example, patient flow would be compromised, and it would be inefficient to have a sonographer waiting to perform an examination while another sonographer performed a 60-minute examination. The work/rest ratio and patient flow would be most efficient if a sonographer went to break while another sonographer was performing a short examination. In this way, efficiencies were maximized between sonographers and examination room availability.
Individual worklists became necessary to capture the workflow of each sonographer and also to include the emergent cases, portables, and interventions that are not included into the booked patient schedule. It was clear that these lists would need to be created on a daily basis due to the variable number of add-ons and the varied booked patient schedules. Initially, the sonographers’ daily worklists were logged on paper. As each patient arrived, he or she would be assigned to a sonographer. This was cumbersome due to the shifting nature of emergent and urgent examinations. It was also difficult to get an overview of each sonographer’s daily workload or to see what they were doing at any given time. As well, sonographers were feeling that they had no control over their workload.
To overcome the problems associated with individual paper worklists, a large magnetic whiteboard was used (Figure 2). Each sonographer scheduled for the day was assigned a column. Magnets were made for each examination type. The sorter was assigned to create the sonographers’ worklists each morning using the list of booked patients and all orders for inpatients and portables. The sorter would also mark out any openings for emergent and urgent patients that could be added as the day unfolded. Scheduling the breaks and lunches was the best place to start when building the sonographers’ worklists. Every effort was made to schedule breaks mid-morning and mid-afternoon rather than at the beginning or end of a shift since it is better to allow appropriate muscle recovery time in the middle of a work period.
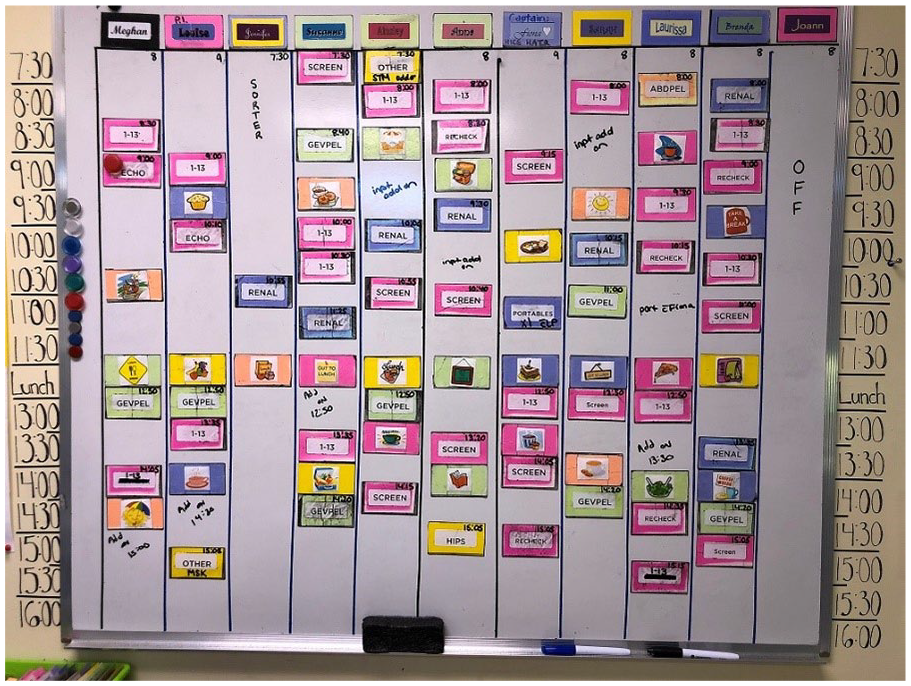
A magnetic whiteboard was used to create sonographer schedules daily. Magnets were created for each examination type, breaks, lunch, meetings, appointments, and sonographer names. These were added each day in the sonographers’ column to create a unique workload for each sonographer.
Another necessary aspect of developing the worklist to reduce the risk of WRMSDs was to ensure that the examination types are mixed so that no sonographer would be assigned two high-risk examinations back to back. While this was facilitated by the outpatient schedule that ensured that examinations were mixed, even with advance planning, there were days when creating the worklists was difficult due to sick calls and vacations. Nevertheless, every effort was made to avoid two high-risk examinations back to back, such as 20-week anatomic obstetric screens and gynecologic transvaginal examinations. These types of examinations that carried the highest risk for WRMSDs were intermixed with lower-risk examinations such pediatric hip, renal, or first-trimester obstetric for dating.
The use of the whiteboard made it possible to see what each sonographer was doing, to make sure the workload was balanced between sonographers, and to see where there were openings to schedule urgent/emergent cases, and the magnets made it possible to easily readjust as the day unfolded. This solution was enthusiastically accepted by the sonographers. Sonographers were able to see what their day would be like as they arrived for their shifts. They were able to see when their breaks were scheduled and where emergent/urgent patients may be added. This created a sense of control over their day and thus reduced stress. This method also has the benefit of everyone being able to see the workload of the other sonographers, which can prevent the possibility of “cherry-picking,” where a sonographer may choose scans that are shorter and easier and leave the difficult examinations for other sonographers. In this department, this ability to see what other sonographers were doing fostered a sense of looking out for each other. This was done to ensure that no one ended up with too many examinations that were high risk for WRMSDs. Sonographers would indicate with a marker on the whiteboard when they had a patient with an increased body mass index (BMI). They would then monitor each other and offer to take a high-risk examination from another sonographer who may have just completed an increased BMI examination, an exceptionally difficult examination due to abnormality, or fetal lie.
Maintaining and Improving the Process
Implementation of the new scheduling routine should not be the end of the process, and multiple ongoing activities are required to ensure that the process continues to support both the needs of the department and patients, as well as the health of the sonographers. Workload statistics must be monitored on a regular basis to ensure that the wait time targets are met without compromising the sonographers’ health. It is our practice to monitor the highest volume examination types monthly. The other examination types may be assessed at year end to ensure there are no significant changes in volume. The schedules can be tweaked periodically when trends become long-term changes rather than fluctuations.
New time studies may be needed to update scheduling when new ultrasound systems are purchased, which could significantly increase or decrease the times across examination types. For instance, new machines that automate annotation and measurements may significantly decrease examination times. Conversely, if the new ultrasound systems are capable of advanced imaging technologies such as 3D/4D imaging and protocols are changed to include these technologies, then the examination times may be longer to allow for postprocessing manipulation of the data sets. It would likely be beneficial to allow sonographers a period of time to become accustomed to new ultrasound systems to maximize their efficiencies prior to performing a time study.
Similar to new machines, updates to examination protocols can result in altered examination times, prompting a need for new time studies. Multiple small additions to protocols can happen over a long period of time, resulting in increased lengths in the time required to complete particular examinations. For instance, the protocol for the 20-week anatomy scan in obstetrics has been slowly but steadily growing over the past decade. It was once reasonable to book these examinations as 30-minute appointment times, but with the addition of assessing for soft markers, more extensive screening of the fetal heart and other structures, additional measurements, and color Doppler assessments, it is appropriate to make these 50- to 60-minute appointments.
There may also be times when new or more services may be offered by a sonography department. These additions should not be taken on without consideration for how it will affect the sonographers’ workloads. Sonographers and physicians may have the expertise and skills to offer new services, but there should be a thorough assessment for the demand of the service and staffing levels adjusted accordingly.
Implications for Practice and Research
Rationale for Implementing Risk-Minimizing Scheduling
Using a systematic approach that takes into consideration the demand for each examination type, length of examination, staffing and equipment, and hours of operation, a schedule can be created that allows muscle recovery time between examinations and a rotation between examinations that are high risk and low risk for WRMSDs. This is the first step toward establishing transducer time thresholds below which WRMSD risk is acceptable.
Sonographers play an important role in the diagnostic imaging department. Their skill sets are difficult to replace. An injured sonographer can have a great impact on the operations of a department from a number of perspectives. It can be difficult to find a replacement sonographer for one who is off with an injury. If no replacement is found, the workload is then covered by the remaining sonographers. The increased workload then increases the risk of injury to those sonographers. While a larger staff can likely cover one sonographer’s workload with little risk for WRMSDs, a department with only two or three sonographers will have a much higher risk for WRMSDs due to the greater workload distributed across fewer sonographers. In addition, rescheduling patients creates other problems, not the least of which is delaying diagnosis for those who were rescheduled. The rescheduling of patients creates a snowball effect since the examinations will be rescheduled into appointment times that would have otherwise been available for new patients. The new patients then have to wait longer and so on. Rescheduling also creates more work for the staff responsible for booking.
To fully accommodate the work, the sonographers’ schedule must account for more than just direct examination time. A sonographer’s schedule must incorporate time for preparing observation notes and presenting the case to the reading physician. In addition, the schedule must allow for rest breaks between each patient to allow time for the muscle to recover. The time needed for recovery of muscles fatigued by static work, which is just one of the causes of WRMSDs in sonographers, can be more than 10 times that of active work. 8 A schedule that encourages task rotation to alleviate the strain placed on the same muscle groups over long periods of time also reduces the risk of WRMSDs. 15
Taken together, developing a culture of prevention is cost-effective. When sonographers are injured, there are extremely high costs associated with sick time, workers’ compensation claims, and long-term disability. 16 In addition to these costs, employers will often pay additional costs, such as overtime for other employees. A sonographer who is overbooked will most often incur overtime, which is generally paid at a rate of one and one-half times the regular rate of pay.17,18
In the end, the benefits of spending time and money on creating schedules for sonographers and ensuring staffing levels to meet the demand on the department outweigh the financial costs as WRMSDs are the highest of lost-time injuries and cost in workers’ compensation in Canada. 8
Future Research
This work is a case study of one department and is meant as a starting point for the field. Implementing a scheduling process could be useful in determining appropriate or maximum workloads for sonographers. This protocol for creating a schedule of examinations may only work for sonographers working in general diagnostic imaging, in which a wide variety of examination types are performed and cannot be extrapolated to cardiac and high-risk obstetric, where there are limited varieties of examination types. 3 Reports from other settings should be recorded and shared to provide insight and support for the broader sonography community. Importantly, quality improvement metrics should be captured to validate both the cost-effectiveness and performance of these processes.
In addition to examining the benefits of making administrative and scheduling changes within sonography departments, additional studies are needed to determine discrete thresholds of strain below which the risk of injury is acceptable. In particular, more information is needed to better understand the relationship of transducer time to rest time and the impact of individual examinations. This study used a weighting system based on individual sonographer ratings, but more objective measures of risk would be important. Smart clothing has been used in research to assess strain in white-collar workers and sterile processing staff. 19 Studies using similar methods, including wearable sensors or other applications, could be a very useful method of determining exactly how much strain a sonographer experiences over the course of a shift.
Footnotes
Acknowledgements
The author thanks Megan Brydon, MSc, BHSc, RTNM, and Jennifer Kressebuch, BHSc, CRGS.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.