
Abstract
Objective:
To investigate the level of occupational burnout syndrome in a cohort of sonographers and to determine any associations between sex, number of hours worked per week, and burnout.
Materials and Methods:
This study used a cross-sectional approach that replicated the Oldenburg Burnout Inventory and surveyed a convenience sample of sonographers who are members of the Society for Diagnostic Medical Sonography.
Results:
The study survey offered the total scores of occupational burnout, disengagement, and exhaustion, with a potential minimum score of 16 and a maximum score of 64. The results yielded a minimum score of 17 and a maximum score of 64. The mean score was 43.11 (SD = 7.02), indicating a moderate level of burnout.
Conclusion:
This cohort of sonographers demonstrated moderate levels of burnout, so it is important to acknowledge that preventing occupational burnout is necessary to ensure that workplace stress is managed to avoid significant issues. Further research is needed to assess how occupational burnout syndrome affects retention in the profession.
Occupational burnout syndrome is not a new affliction affecting health care professionals. It was first endorsed in the International Classification of Diseases, Tenth Revision in 1990 1 and, more recently, in the International Classification of Diseases, Eleventh Revision by the World Health Organization. 2 This phenomenon can be defined as a conceptualized syndrome resulting from chronic workplace stress that has not been successfully managed. It is often characterized by three major components: feelings of exhaustion, cynicism toward one’s occupation, and a reduction in the employee’s productivity. 2 Although occupational burnout syndrome is not identified as a medical condition, it may still cause physiological symptoms that can directly affect a person’s mental and physical well-being.
Using the library’s electronic databases, the following key terms were used to conduct the literature search: burnout among sonographers, burnout in radiology, compassion fatigue among sonographers, stress among sonographers, and burnout among diagnostic medical imaging professionals. The search was then narrowed down to peer-reviewed articles written in English between 2017 and 2022. Of the generated results, seven articles were chosen based on their relevance to occupational burnout syndrome among sonographers or if they contained similar topics, such as burnout among medical imaging professionals or radiologists. Articles that focused on health care professionals outside of diagnostic medical imaging were excluded.
Following article selection, the data were evaluated and extracted to formulate a synthesis matrix for assessing the three common themes found in the literature. The themes included potential causes and risk factors, methods of retrieving and measuring data, and occupational burnout findings.
Potential Causes and Risk Factors
Many workplace variables can lead to occupational burnout. In this collection of articles, increasing workloads and increasingly demanding work hours were identified as the major contributors to increased levels of work stress. Singh et al. 3 reported that profit-oriented organizations tend to have higher staff workloads, leading to failure to cope with increased patient needs and technological advances. Shields et al. 4 reported that it is difficult to manage workplace pressures when work demands exceed the ability of workers and available resources. Ayyala et al. 5 stated that on-call demands among pediatric radiologists are becoming more onerous, which can potentially compound their state of burnout. Guclu et al. 6 mentioned that on-call burden, in general, is a burnout risk factor for all health care workers. In addition to the increasing work hours in sonography, there is heightened pressure to generate high-quality sonographic examinations that are highly operator-dependent. 4 Cohen et al. 7 reported that sonographers are more compelled to deal with the demands of increasing examinations along with demanding work hours.
Singh et al., 3 Cohen et al., 7 and Johnson et al. 8 reported that daily interactions between health care professionals and patients are emotionally stressful. Johnson et al. 8 specifically mentioned that delivering difficult diagnostic information, such as pregnancy loss, fetal demise, or congenital fetal anomalies present during obstetric sonography can contribute to anxiety and depression.
Physical afflictions experienced by sonographers, such as eye strain, muscle aches and pains, carpal tunnel syndrome, and fatigue, have also been reported by Cohen et al. 7 Limited research pertaining to musculoskeletal disorders in conjunction with occupational burnout has been published.
Methods to Retrieve and Measure Data
Johnson et al. 8 evaluated occupational roles in burnout syndrome with sonographers who had prior disciplinary practice in radiography, midwifery, medicine, and other fields. Singh et al. 3 reported burnout among sonographers, radiographers, and radiologists. Shields et al. 4 also conducted surveys among sonographers and radiographers but included nuclear medicine technologists and radiation therapists in their study. Cohen et al. 7 analyzed data on sonographers from various countries, including the United States (Tennessee), the United Kingdom (Leeds), Nigeria (Anambra), Australia, and New Zealand.
Cross-sectional questionnaires and surveys were conducted, in the studies procured, and these were used to measure the prevalence of occupational burnout syndrome. Six out of the seven studies used versions of the Maslach Burnout Inventory (MBI) survey, which investigates three components: emotional exhaustion, depersonalization, and lack of personal accomplishment.3 –5 Emotional exhaustion refers to feelings of depletion and overextension. 5 Depersonalization is defined as a cynical attitude and personal detachment toward one’s job, and a lack of personal accomplishment, which can be described as perceived professional incompetence. 5 Shields et al. 4 and Johnson et al. 8 reported using the Oldenburg Burnout Inventory (OBI) survey; Johnson et al. 8 used this survey as the only measurement tool, whereas Shields et al. 4 included it with the MBI survey and Professional Quality of Life (ProQOL) survey. According to Johnson et al., 8 disengagement is characterized by feelings of detachment from work, whereas exhaustion is defined as a state of being overstretched by work. In addition to assessing disengagement and exhaustion, Johnson et al. 8 also measured general mental well-being and the development of psychiatric disorders, such as anxiety and depression.
Findings of Occupational Burnout
In this study, occupational burnout was measured using the MBI survey, which evaluates emotional exhaustion, depersonalization, and lack of personal achievement3 –5; the OBI survey, which evaluates disengagement and exhaustion 8 ; the ProQOL survey, which evaluates compassion satisfaction, burnout, and secondary traumatic stress; and general surveys that evaluate physician and mental well-being.
Regarding occupational burnout based on gender, Singh et al. 3 found that female sonographers and radiographers who worked more than 10 hours of overtime per week had significantly higher emotional exhaustion and depersonalization. Singh et al. 3 also reported that male sonographers who were involved in less than 10% of the training per week had higher levels of depersonalization than female sonographers.
Guclu et al. 6 reported that being on-call altered burnout parameters to a significant degree. A mean age of 35 years and completing on-call duty were reported to be positively correlated with severe insomnia. This study also demonstrated that there was a positive correlation between burnout, insomnia severity, and anxiety levels among health care professionals. 6 Johnson et al. 8 reported that 88.9% of their sonographer participants were classed as having mental health issues such as anxiety or depression, with 80% of the sample suffering from either mild (38.9%) or severe mental health issues.
Cohen et al. 7 reported that the incidence of sonographer burnout has increased based on published studies but varies considerably across different geographic cohorts. Participants from Nigeria reported average levels of burnout compared with cohorts from the United States, which reported moderate levels of burnout. 7 By comparison, participants from the United Kingdom, Australia, and New Zealand reported higher levels of burnout. 7
Based on the issues highlighted in the literature, this study aimed to investigate the incidence of occupational burnout syndrome among sonographers and to assess the potential factors that lead to chronic workplace stress perceived among working sonographers. The research questions are as follows:
Research Question 1: Is burnout a common phenomenon experienced among sonographers?
Research Question 2: Are there significant differences between the sexes, number of hours worked per week, and burnout rates among sonographers?
Research Question 3: Between disengagement and emotional exhaustion, which components of burnout are the most prevalent among sonographers?
Materials and Methods
A cross-sectional survey was used to collect data on burnout among sonographers. Ethics approval was obtained from the institutional review board (IRB) of the MD Anderson Cancer Center to conduct this survey (IRB no. 2022-1026).
Sample Selection
The participants of this study included sonographers who were members of the Society of Diagnostic Medical Sonography (SDMS) and employed at acute care facilities, outpatient facilities, imaging centers, and physician offices. The participants could be uncredentialed or hold single or multispecialty credentials from The American Registry of Radiologic Technologists, The American Registry for Diagnostic Medical Sonography, or Cardiovascular Credentialing International credentialing organizations. The participant frame comprised 14 724 SDMS members who opted for their mailing list.
Instrumentation
The OBI survey was built into Qualtrics and consisted of 16 items measuring disengagement and emotional exhaustion. Disengagement refers to feelings of withdrawal, whereas emotional exhaustion refers to feelings of depletion and overextension. 8 Each subscale includes various questions with frequency rating choices, including strongly agree, agree, disagree, and strongly disagree. There were six additional items in the survey to collect background information regarding sex, the type of facility the sonographer was employed at, what specific days and shifts the sonographer worked, and the number of hours worked per week. The last two items collected data on how frequently participants considered leaving their profession. The sex options included female, male, and preferred not to answer. Hours worked per week included 24 hours or less, between 25 and 32 hours, between 33 and 36 hours, between 37 and 40 hours, and 41 hours or more.
The psychometric properties of the OBI survey have shown acceptable to very good validity scores in terms of internal consistency, which made it a reliable instrument to measure burnout, in various occupational contexts. 9 The reliability estimate for the second-order burnout factor was .785. 9 Due to its validity in previous literature, a pilot study was not necessary. The first six survey items included demographic and occupational factors. There were eight statements in the matrix table (Q7) that evaluated disengagement and eight statements in the matrix table (Q8) that assessed exhaustion. The Q9 matrix table contains two statements regarding their consideration of leaving their profession (see Supplemental Appendix SC for the survey instrument).
Data Collection and Analysis Procedures
Participants received an e-mail from the SDMS with a Qualtrics link and a request for their participation in the study. The e-mail contained the purpose of the study, statements clarifying that participation was voluntary, statements affirming that their identity would remain anonymous, and statements indicating that their privacy would not be compromised. The e-mail also provided informed consent, detailed instructions on how to navigate the survey, and a link to the survey. The survey opened when participants selected “yes” to begin the survey, or the survey ended when participants selected “no.” The survey link was active for 3 weeks, from February 10 to March 3, 2023.
The results were exported from Qualtrics to SPSS (IBM Corp., Chicago, IL, USA) to analyze multiple-choice and demographic items using descriptive statistics and percentages. Given that the data were not normally distributed, a nonparametric set of statistics was used. To assess any variances between gender and hours worked per week with burnout, a Kruskal-Wallis H test was completed to determine whether there were any significant differences. The alpha level (P < .01) was determined a priori. All results and supporting files were saved on a secure network with limited personnel access behind the institutional firewall, and e-mail communication between the researchers was conducted over a secure server.
Results
A total of 1049 survey responses were received, yielding a response rate of 7.1%. Among them, 104 were incomplete and discarded, and the remaining 945 responses produced a 90.1% completion rate. An additional 31 respondents were identified as not working as sonographers, leaving 914 responses for analysis. The margin of error for this sample size of 914 is ± 3.2%, at the 95% confidence level. The Cronbach alpha for the Likert scale items was .880. A survey instrument is reported to have high reliability if its Cronbach alpha value is .70 or higher. 10
Demographics
Responses from this survey identified that 833 (91.1%) participants were women, 76 were men (8.3%), and five (0.5%) preferred not to select a gender classification. The respondents were employed at various facilities, including 506 (55.4%) at an acute care or hospital facility, 400 (43.8%) at an outpatient or imaging center, 202 (22.1%) at a physician’s office, and 27 (2.95%) at other facilities. Travel and mobile ultrasound companies, higher level educational institutions, and medical device companies were among the other types of facilities that were not listed. In addition, 880 (96.3%) participants stated that they usually worked on weekdays, whereas 269 (29.4%) stated that they usually worked on weekends. When asked what shift hours they typically worked, 824 (90.2%) answered morning, 703 (76.9%) answered afternoon, 212 (23.2%) answered evening, and 68 (7.4%) answered overnight, with 114 (12.5%) respondents selecting a variability of shifts. The results indicated that, in a typical workweek, 209 (22.9%) worked 41 hours or more, 379 (41.5%) worked between 37 and 40 hours, 144 (15.8%) worked between 33 and 36 hours, 107 (11.7%) worked between 25 and 32 hours, and 75 (8.2%) worked 24 hours or less.
Scoring Burnout
The scoring range for the disengagement and exhaustion subscales is a minimum of 8, indicating low levels of disengagement or exhaustion, and a maximum of 32, indicating high levels of disengagement or exhaustion. The mean score for disengagement was 20.46 (SD = 3.94), indicating moderate levels of disengagement overall (see Table 1). The mean exhaustion was 22.64 (SD = 3.85), indicating a moderate level of exhaustion (Table 2). To measure general burnout, disengagement, and exhaustion subscales were added, with a possible minimum score of 16 and a possible maximum score of 64. The data reported a minimum and maximum burnout score of 17 and 64, respectively. The mean score was 43.11 (SD = 7.02), indicating moderate burnout.
The Participant Responses to the OBI Survey, Which Measured Disengagement.
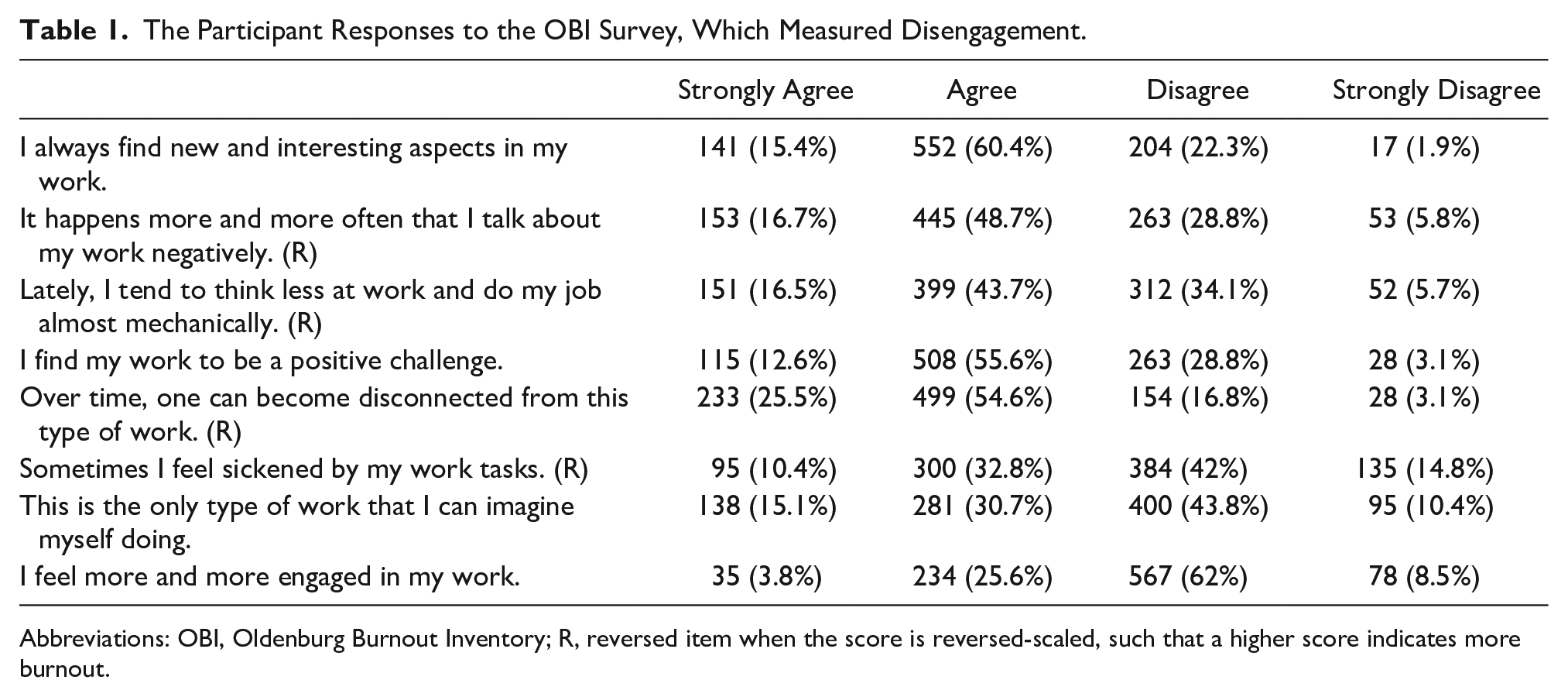
Abbreviations: OBI, Oldenburg Burnout Inventory; R, reversed item when the score is reversed-scaled, such that a higher score indicates more burnout.
The Participant Responses to the Oldenburg Burnout Inventory Survey, Which Measured Exhaustion.

Abbreviation: R, reversed item when the score is reversed-scaled, such that a higher score indicates more burnout.
A Kruskal-Wallis H statistical test did not detect a significant difference between sex and burnout score: χ2(2) = .8, P = .671. However, a second Kruskal-Wallis H statistic showed a significant difference between hours worked per week and burnout score: χ2(4) = 32.2, P < .001. Post hoc testing revealed significantly higher burnout scores among sonographers who worked 41 hours or more per week compared with those who worked 24 hours or less (P < .001) and those who worked between 25 and 32 hours (P = .001). Sonographers who worked between 37 and 40 hours per week had significantly higher burnout scores than those who worked between 25 and 32 hours per week (P = .041) and those who worked 24 hours or less (P = .003). Finally, sonographers who worked 33 to 36 hours per week had significantly higher burnout scores than those who worked 25 to 32 hours per week (P = .016) and those who worked 24 hours or less (P = .001; see Figure 1).
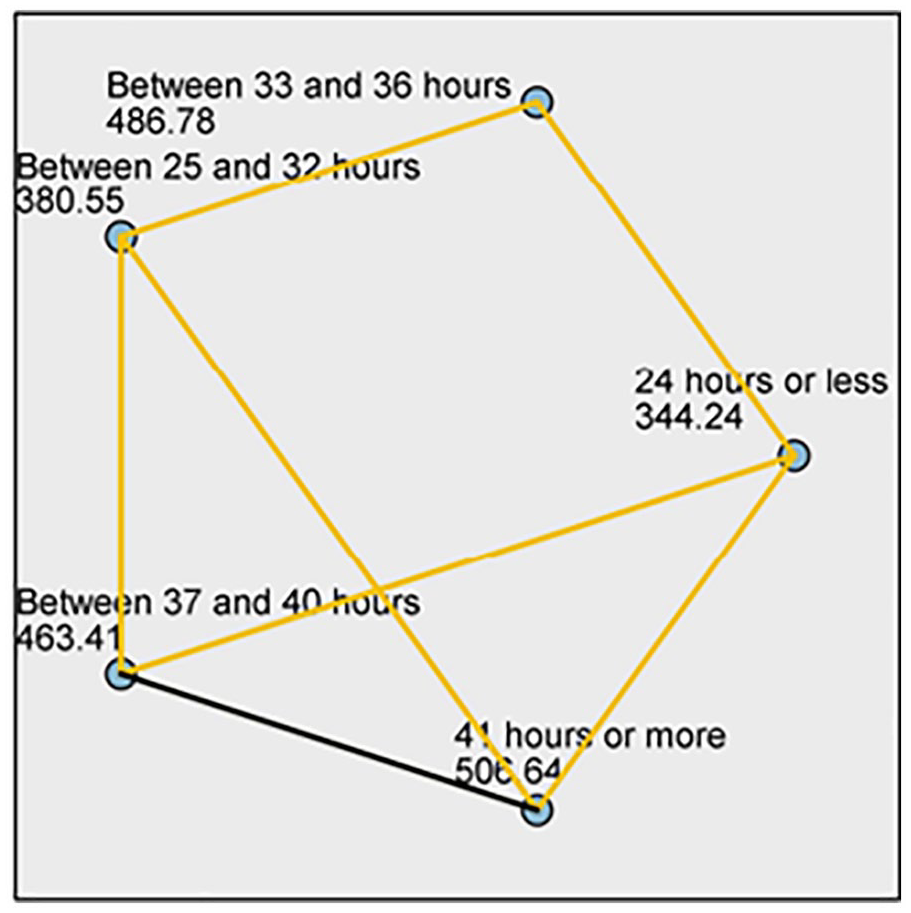
A diagram of the pairwise statistical comparisons of sonographers’ hours worked per week.
When respondents were asked to provide the likelihood of leaving the profession as a sonographer, 222 (24.3%) answered strongly agree, 400 (43.8%) answered agree, 234 (25.6%) answered disagree, and 58 (6.3%) answered strongly disagree. In addition, they were also asked to scale whether they were currently considering leaving the profession as a sonographer, and 148 (16.2%) selected strongly agree, 264 (28.9%) selected agree, 369 (40.4%) selected disagree, and 133 (14.6%) selected strongly disagree.
Discussion
This study evaluated a cohort of sonographers who provided survey responses between February 10 and March 3, 2023. These responses were analyzed to determine their level of occupational burnout syndrome. Findings from this survey yielded a mean score of 20.46 (SD = 3.94) for disengagement, indicating moderate levels of disengagement, and a mean score of 22.64 (SD = 3.85) for exhaustion, which indicated moderate levels of exhaustion. The total burnout score was 43.11 (SD = 7.02), indicating that the sonographers experienced moderate levels of burnout. Between the two burnout dimensions, exhaustion appeared to be more prevalent than disengagement. The implications for this finding could be due to poor work-life balance, as 695 (76.0%) respondents answered that they did not have enough energy for leisure activities after work, and 813 (88.9%) respondents answered that they felt tired before arriving at work. The inability to tolerate work-related stress or a heavy workload could also be a potential stressor, as 741 (81.1%) respondents answered that they felt worn out and weary after work, and 665 (72.8%) answered that they often felt emotionally drained during work. When compared with previously published work3 –5,7 that reported a failure to cope with work-related stress, increasing workloads contributed to employee exhaustion levels as a part of burnout. In addition, Ayyala et al. 5 reported poor work-life balance and mental health as additional factors that could lead to increased levels of exhaustion.
This study also aimed to identify any differences between gender and the number of work hours accrued per week with burnout syndrome. However, the analysis did not detect significant differences between sexes or burnout among sonographers. When assessing the differences between the number of hours worked per week and burnout, post hoc analyses revealed significantly higher burnout scores among sonographers who worked more hours.
Along these lines, when comparing previous studies with the current one, it is evident that there is a positive correlation between increased work hours and occupational burnout syndrome. Singh et al. 3 found that sonographers who worked more hours, specifically >10 hours of overtime, had significantly higher emotional exhaustion, F(2, 116) = 4.7, P = .011, M = 49.2, SD = 6.2, and higher depersonalization, F(2, 116) = 5.2, P = .007, M = 24.7, SD = 4.3. Increased workloads, which include increased work hours and responsibilities, have been shown in other studies to be associated with burnout.4,5,7 Moreover, Ayyala et al. 5 reported that, among the different dimensions of burnout, exhaustion was observed in 286/435 (66%) respondents, and depersonalization was observed in 265/433 (61%) respondents. Cohen et al. 7 also demonstrated a direct relationship between an increased number of sonographic examinations per week with increased exhaustion scores, and working more overtime hours per week with significantly higher exhaustion scores. Research conducted by Shields et al. 4 indicated that sonographers exhibited higher levels of exhaustion (64%) than depersonalization (46%) and personal accomplishment (27%). This is in comparison with the work by Singh et al., 3 who reported that 98.3% of sonographers indicated high exhaustion scores, 89.2% of their cohort indicated high depersonalization scores, and 34.7% had high personal accomplishment scores. Similar to this study, exhaustion has been demonstrated to be more prevalent when comparing the different components of burnout. Ayyala et al. 5 found a strong association between financial strain and poor mental health, highly demanding work hours, and the burden of on-call demands as potential stressors that can negatively impact exhaustion levels. Cohen et al. 7 found that exhaustion was more prevalent owing to increasing sonographic examinations, hours worked per week, working in a hospital setting, and chronic exposure to stressful situations. Shields et al. 4 also found that workplace pressure and increased workload affect exhaustion when it comes to burnout. Similarly, Singh et al. 3 found that an increased workload was a contributing factor, but failure to cope with job-related stress led to increased exhaustion levels.
Although this study did not detect an association between sex and burnout, a positive correlation was reported. Ayyala et al. 5 reported that burnout was more prevalent among female respondents due to work-life imbalance, a competitive job market, and stress from caring for dependents. Female respondents also reported experiencing higher levels of burnout from increased after-hours responsibilities and longer work hours, with an increasing 12% to 15% burnout score for each additional 5 hours worked more than 40 hours in a week. 5 Zanardo et al. 11 found that women with children had higher scores of burnout and higher scores of emotional exhaustion, compared with other components that contributed to burnout. This differed from other studies published by Singh et al., 3 Guclu et al., 6 and Johnson et al., 8 which found no significant correlation between sex and occupational burnout. This could not be investigated thoroughly in this study because of the unequal number of gender-based responses (833 women and 76 men), which made it difficult to make a comparison.
Limitations
This study had some limitations. First, the research design was pre-experimental and posed inherent threats to internal and external validity. This study was limited to a sample size of 914 participants with an SDMS. In addition, the participants were only those who opted for inclusion in the SDMS mailing list. The SDMS is an American-based organization; however, there is the possibility of members being located outside of the United States. In comparison, the survey instrument used was not as extensive as the MBI survey as it measures 3Ds of burnout rather than the OBI’s 2Ds. Finally, the OBI survey can be constrained because its Likert scale does not allow for the selection of a neutral response. With the only available choices being different levels of agreement or disagreement, the participants were forced to make a positive or negative selection.
Conclusion
This study aimed to investigate the incidence of occupational burnout syndrome among a cohort of sonographers and assess whether any differences between sexes and the number of work hours accrued per week contributed to occupational burnout. These results suggest moderate levels of burnout. There was also a significant difference between burnout and increased working hours, indicating that sonographers who worked longer hours experienced higher levels of stress.
Further investigation is needed to determine whether specific factors, such as place of employment, marital status, status of dependents, physical well-being, mental health, and years of experience in the profession play a role in the development and implications of occupational burnout among sonographers. Future research should recruit a larger cohort of sonographers and ensure that they are highly representative of the profession. It may also be important to consider using the MBI as it may provide a wider variety of responses from participants.
Although this review demonstrated moderate levels of burnout, acknowledging this issue is necessary to ensure that workplace stress is managed before it becomes a significant issue. Assessing how burnout affects working sonographers could aid in managing workplace stress and improving employee retention.
Supplemental Material
sj-docx-1-jdm-10.1177_87564793231213364 – Supplemental material for Incidence and Cause of Occupational Burnout Syndrome Among Sonographers
Supplemental material, sj-docx-1-jdm-10.1177_87564793231213364 for Incidence and Cause of Occupational Burnout Syndrome Among Sonographers by My Tran in Journal of Diagnostic Medical Sonography
Footnotes
Acknowledgements
I would like to express my special thanks of gratitude to my thesis adviser, Dr Suzieann Bass, and committee member, Dr Kevin Clark, for their guidance during the IRB (institutional review board) process, the editing of this thesis, and their mentorship throughout this graduate program. In addition, this endeavor would not have been possible without the leadership from the Society of Diagnostic Medical Sonography who supported and facilitated my survey to members. I am also grateful to my family, friends, and partner for being my driving force and whose love is with me in whatever I pursue. Finally, I would like to thank my dogs, Thea and Darla, for being my constant joy and for their emotional support during this journey. You are all my inspiration for my accomplishments. We would like to thank Editage ![]() for English language editing.
for English language editing.
Ethics Approval
Ethical approval for this study was obtained from the institutional review board (IRB) of the MD Anderson Cancer Center to conduct this survey (IRB no. 2022-1026).
Informed Consent
Informed consent was not sought for the present study because all case data was de-identified and/or aggregated and followed ethics committee or IRB guidelines (also referred to as the Honest Broker System).
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used for the study.
Trial Registration
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.