
Abstract
Objective:
Work-related injuries have a major effect on worker health and well-being. This is particularly true in sonography, where work-related musculoskeletal disorders (WRMSDs) are common. In response to the current challenge of understanding strategy implementation across social and organizational dimensions, this research captured sonographers’, echocardiographers’, and vascular technologists’ perceptions of critical administrative, organizational, and general health and training challenges, and potential solutions for improving worker health and well-being.
Materials and Methods:
A survey invitation was sent to the WRMSD Grand Challenge longitudinal study registry participants. Open-ended questions on the online questionnaire allowed respondents to share comments, ideas, or potential solutions to improve worker health and well-being regarding the administrative and organizational environment or through training and general health interventions. There were 377 free-text responses that were qualitatively analyzed using a grounded theory approach to generate overarching themes and identify emerging theory, supported by initial coding, focused coding, and reflexive memoing. A member check was conducted by interviewing four participants to refine and confirm the findings.
Results:
Five themes were identified: “Limits and Guidelines,” “Injury Education,” “Ergonomics Training Constraints,” “Resources and Equipment,” and “Individual Habits.” Participant suggestions within these themes were categorized and mapped onto a sociotechnical systems model that was developed previously to study the healthcare system(s) in which sonography users work. This conceptual mapping revealed how these solutions were situated to impact different levels of the work environment. The themes and mapping supported an emerging grounded theory: Risk Reduction Relies on Proper Employee Representation.
Conclusion:
These qualitative findings align with contemporary guidelines and recommendations for mitigating injuries in sonographers, illuminating challenges and solutions targeting levels of influence beyond the staff sonographers’ scope. The need for representation of sonographers at higher-level administrative levels has not heretofore been addressed by WRMSD guidelines.
Keywords
Maintaining health in the workplace is an evolving topic as people have adjusted to fluctuating work contexts that differentially affect various aspects of health and well-being.1 –7 An emphasis on individual responsibility has been a recurring theme in the evolution of work in the United States, particularly concerning personal health management. 8 Classically, managing personal health has been defined as “any informal, unpaid work done to manage, monitor, inform, or influence personal (or family) health outcomes.” 9 This concept has been acknowledged and problematized in multiple fields, including social work and nursing.10,11 In terms of work, an emphasis on individual responsibility to maintain personal health may begin to conflict with employees’ ability to simultaneously uphold workplace productivity standards. For example, workers seeking to balance work-life roles may find it an unattainable goal due to conflicting personal health and work demands.12,13
Implicated within this broad topic of worker health responsibility is the issue of work-related injury and poor psychological well-being. In sonography, the prevalence of experiencing musculoskeletal symptoms that are associated with work is high and has been for more than two decades. Over this time, three large surveys of comparable groups of sonographers (from Canada and the United States), asked respondents to report on symptoms that were associated with their work. In the first 1997 survey, 71% of respondents reported that they were experiencing symptoms which had developed since the start of their work as a sonographer. 14 An additional survey in 2009 reported that 90% of respondents experienced pain during scanning. 15 The most recent data, published in 2023, showed 86% of respondents regularly experience musculoskeletal discomfort that the respondents attributed to work. 16 Sonographers, echocardiographers, and vascular technologists are at risk for developing musculoskeletal symptoms and injuries as a result of repeated exposure to working in awkward postures and forcefully griping and pushing the transducer to obtain high-quality images.17 –19 In turn, these behaviors are driven by factors in the work environment, including patient body habitus, room configuration, and equipment design. Due to the ongoing elevated prevalence of musculoskeletal symptoms in this working population, there has been a renewed effort to identify a broader range of solutions for reducing the development of work-related musculoskeletal pain and disorders in ultrasound users. An example of these expanded efforts is the practice principles for preventing work-related musculoskeletal disorders (WRMSDs) generated through a cross-professional collaboration led by the American Institute of Ultrasound in Medicine (AIUM) that fall into several categories, including “Workplace Culture,” “Administrative Controls,” and “Personal Controls.” 20
As the focus of intervention expands, a resource that has been underutilized in the development of injury reduction strategies is directly capturing the voice of sonographers themselves, informed by their experiences, as acknowledged by Simonsen and Gard in their qualitative study of sonographers in Sweden. 21 The voice of participants with firsthand experience, captured by recorded audio or free-text responses using qualitative methods, can produce additional detail that may serve the utility of quantitative findings. In an earlier study of 81 cardiac sonographers, Horkey and King found that despite widespread awareness and implementation of several recommended ergonomic interventions that were under the control of the sonographers (e.g., vary your posture throughout the day while scanning, rotate between sitting and standing to perform exams, perform stretches throughout the day, use an adjustable bed and chair), musculoskeletal discomfort was still prevalent in the group (90%). 22 Notable on the list of intervention recommendations were several that management would need to initiate (e.g., fully adjustable ultrasound equipment system, scheduling that permits rest breaks of 15 minutes every 2 hours, walls in scanning rooms should not be painted light colors). 22 The study’s sonographers preferred interventions they could implement themselves and found these to be more feasible, but this preference was not explored further. That study concluded that efforts were needed to better understand the effects of specific ergonomics interventions. 22
Understanding the nuances of consistent behavior for injury reduction is complex due to intersections with social and organizational factors. Therefore, the current study gathered reflections from the lived experiences of a cohort of sonography users to examine how they ideate workplace injury prevention at multiple implementation levels, from the individual to upper levels of administration and authority, and the implications for currently promoted best practices. Capturing sonography users’ experiences with challenges and solutions for managing the risk of WRMSDs can provide valuable insights into what might constitute successful prevention strategies. Areas of emphasis extracted within this analysis were improvement suggestions for health and wellness related to the administrative and organizational work environment, worker training, and general worker health. Long-form comments concerning the challenges of applying ergonomics training were frequent, and thematic analysis resulted in solutions posed by these sonography professionals to assist their daily applications of this training.
Materials and Methods
Study Design and Research Paradigm
An online survey was distributed to practicing sonographic professionals who joined a longitudinal research registry focused on an improved understanding of factors associated with WRMSD within the field.23,24 The host university’s institutional review board approved the study (IRB#2021B0113), and respondents consented to participate before completing the questionnaire. Alongside close-ended questions focused on rating workplace challenges and identifying priorities for intervention, open-ended questions were included to gather comments and suggestions related to solutions for improving their health and well-being. Data included in this report are focused on comments regarding the workplace environment, training, and general health obtained from two prompts: “Please share any ideas or potential solutions that you think might address or improve ultrasound user health and well-being with regard to” followed by “the administrative and organizational environment” or “training and general health factors.”
The researchers used a constructivist grounded theory approach and employed inductive reasoning as the data generated by these prompts were reviewed and coded. 25 Particularly, the researchers drew from Charmaz’s constructivist grounded theory, which emphasizes researcher interpretation through theoretical coding and ongoing reflexivity. 26 The researchers first undertook line-by-line coding of the participant responses. As the coding process began, two researchers worked together to isolate key phrases and wording, which helped to construct categories of emphasis. This constructivist approach was made possible due to the detailed descriptions survey participants provided, allowing the researchers to arrive at a thematic consensus. Themes were generated at a semantic level in which researchers organized the data based on patterns in descriptive coding, summarized these patterns, and then attempted to interpret the significance of these patterns. The systems model proposed by Moray 27 was pivotal in simplifying the phrases extracted from the respondents and the memoing.
Data Collection and Participants
The Grand Challenge Alliance, a group of professional diagnostic medical ultrasound organizations with a general initiative to reduce WRMSD in sonographers, echocardiographers, and vascular technologists, launched the “WRMSD Grand Challenge.” 28 A longitudinal study is one of the efforts supported by the Grand Challenge Alliance, and data examined in this report resulted from one of the study’s follow-up questionnaires. The longitudinal study research registry created includes a diverse population of 3659 sonography users, including physicians, sonographers, echocardiographers, vascular technologists, and other healthcare providers. Within the registry, 95% of individuals are from the United States, 85% self-identify as white, non-Hispanic, and female, and the average age was 48.5 years. 23
In June 2022, a follow-up questionnaire was distributed to registry members using the online Qualtrics platform. 1276 survey responses were recorded (34.9% response rate), and 287 unique study participants commented on at least one of the two open-ended prompts. After removing responses that were either irrelevant to the prompt or illegible (n=11), responses from 274 individuals were analyzed. Demographic characteristics of these 274 respondents are as follows: average age at the time of the 2022 survey was 52.5 years (10.5), 84% self-identified as white, 86.5% self-identified as female, 75% reported having one employer and another 15% had two employers. Seventy-seven percent worked full-time, 17% part time, and the rest worked per diem, as a traveler, contractor, or were self-employed. Regarding primary practice areas, respondents could select multiple; Abdominal: 44%, Breast: 25%, Cardiac (adult): 33%, Cardiac (pediatric): 11%, OB/Gyn: 55%, Pediatrics: 23%, Vascular Technology: 55%, and all others being less than 10%. Of the sample, 95% worked in the United States and the rest of the participants worked in Canada.
A corpus of 377 comments from the 274-person sample were included in the qualitative analysis. Responses that were prepared for analysis varied in length from 2 to 156 words. A short participant response was noted to be less than one complete sentence long, an average response to be one complete sentence to multiple short sentences long, and a long response to be a paragraph to multiple paragraphs long, with a paragraph consisting of four or more descriptive sentences. Given this criterion, out of the 377 responses, 42 were short, 304 were average, and 31 were long.
Data Analysis and Trustworthiness
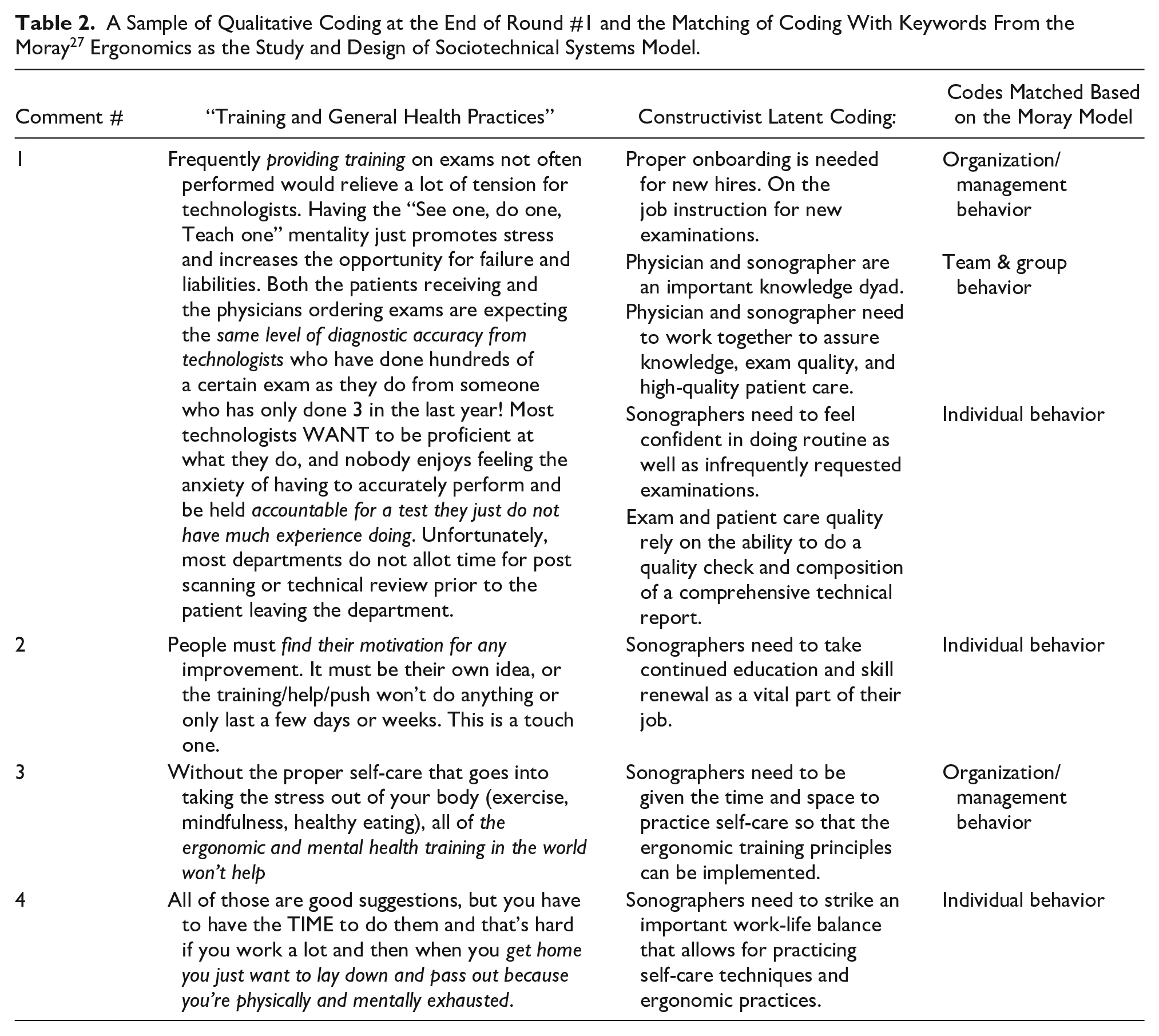
Two researchers (KDE and MRP) led the construction of a grounded theory, which was completed through two cycles of descriptive coding. In the first coding cycle, each researcher completed initial line-by-line coding. 29 The researchers worked via teleconference to compare their initial coding and collectively worked to confirm the meaning behind the statements provided by the respondents. Consensus on the use of codes allowed for a second cycle of coding, in which the researchers applied a focused coding approach. 29 Due to substantial overlap in content from the survey responses to the prompts regarding the “Organizational and Administrative Environment” and “Training and General Health Factors,” these data were merged during the second cycle coding. The outcome of the second cycle of coding allowed for a deeper understanding of how these codes could be logically grouped into categories to describe similar or related responses. At this point, the researchers compared these codes to the keywords used in Moray’s model of ergonomics as the study and design of sociotechnical systems. 27
Both researchers kept individual diaries of reflexive memos and met via teleconference to discuss their memos, coding, and observations during this analytical process. One researcher coding the responses had extensive experience in sonography and hospital/clinic management, and the second researcher was largely unfamiliar with sonography before joining the project. This “outsider” perspective was considered highly valuable as meaning was constructed from the responses. Ongoing reflexivity and discussions revealed that having two diverging perspectives added to the rigor of the coding and overall analysis, as it demonstrated how both researchers, with varied experiences, arrived at a mutual understanding of what was being expressed by the participants.
A final set of themed categories was built based on the groups of codes generated from second cycle coding, review of the Moray model, researchers’ memos, and collaborative discussions between researchers. The set of themes identified by the researchers was used to develop a conceptual map and a confirmatory step of interviewing was conducted as a member check. Selective interviewing was conducted with four participants in leadership roles in general (abdominal) sonography, cardiac, OB/Gyn, and vascular technology. Teleconference interviews conducted via online conferencing software-generated transcripts that were subsequently coded by the researchers and helped validate and refine the themes as part of the grounded theory process. The interviews ranged from 30 to 45 minutes in length. The final conceptual map, themes, and emerging theory were further discussed and validated by two additional researchers with extensive experience in ergonomics, injury prevention, and worker health within the sonography profession (SCR and CMS). The team worked together to report and interpret the findings.
Results
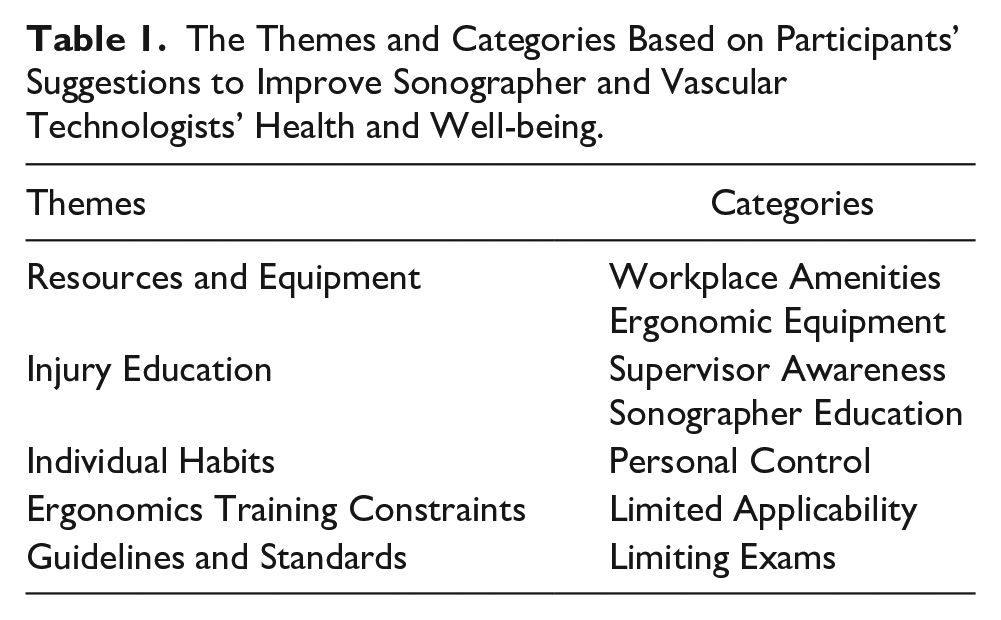
Of the 1276 responses received in the follow-up survey sent to the 3659-person longitudinal study registry, we qualitatively analyzed the 377 free-text responses provided by 274 of the respondents. Five themes with multiple sub-categories were identified from the 377 comments and suggestions for improving sonography workers’ health and well-being related to workplace administration and training practices (see Table 1). These themes are described below, and quotes from the data are provided to illustrate the synthesis of themes. A sample of the coding process connecting the data to researcher memos and organizing categories is provided in Table 2. The integration of these themes into a conceptual map and a description of the proposed emerging theory from this data is provided at the end of this section.
The Themes and Categories Based on Participants’ Suggestions to Improve Sonographer and Vascular Technologists’ Health and Well-being.
A Sample of Qualitative Coding at the End of Round #1 and the Matching of Coding With Keywords From the Moray 27 Ergonomics as the Study and Design of Sociotechnical Systems Model.
Theme 1—Resources and Equipment
The first theme built from the respondents’ suggestions was consolidated around this cohort’s desire for greater access to certain resources and equipment. This was specifically centered on the need for resources that directly assisted workers to prevent work-related injuries and alleviate-related musculoskeletal pain. Based on trends in the suggestions made in survey responses, the two categories of responses used to construct this theme are Workplace Amenities and Ergonomic Equipment.
Category 1: Workplace Amenities
Many participants made similar suggestions that called specifically for treatments, including physical therapy, massages, and chiropractic services, offered in the form of services available at the workplace, as well as paid time off to receive treatment. An example participant quote related to this category was as follows:
Maybe offer a massage program, as massage is the best way to relieve muscle issues . . . believe me, I have spent so much money on acupuncture, physical therapy, and out-of-pocket massage and chiropractors. We should perhaps develop a built-in insurance plan and include paid-for massage, acupuncture, and all the things I just listed.
An additional example of this expressed need is as follows:
Sonographers should be given money or at the very least discounts for routine massages, occupational/physical therapy, acupuncture, dry needling or any other things that can help prevent injury, treat chronic pain, and help with muscle tightness and maintain our overall physical health.
The responses grouped within this category were numerous. The seemingly straightforward reason for sonographers’ direct requests for tangible resources and treatments was to alleviate muscle pains, which have been established as a very common occurrence for sonographers. This category was also buttressed with memoing from the researchers:
Many employees were training in sonography at the community college level, where those institutions provided students with many resources such as sonography faculty, ergonomic scan labs, and recreation centers/gyms. Moving to the employer with these same expectations, the employee rightly is looking for a continuation of these same amenities.
Our OB/Gyn manager interview verified these assumptions:
Our sonographers have not been shy about asking for things like 15-minute massages during the day, stuff like that. That was something that was just brought up at our meeting last week too, like, “Can we maybe have more little things like that sort of help?”
Category 2: Ergonomic Equipment
Ergonomic equipment was another tangible resource that sonographers suggested to prevent WRMSD. Specifically, they raised the point that purchasing ergonomic equipment could directly assist ongoing efforts to prevent work-related injuries by improving the effectiveness of ergonomics training and workshops. An example participant quote related to this category: “Listen to sonographers who are requesting equipment to help their body mechanics and do the best quality scans.” Another respondent commented, “Workshops for ergonomic skills only work if employers are willing to purchase the equipment needed to allow sonographers to benefit from them.” This second participant’s response was similar those who suggested that the workplace purchase ergonomically designed equipment and to provide ergonomics training, which are important steps in reducing the risk of a WRMSD.
This request for equipment and compatible training was noted in the researcher’s memo:
This is further confused by the healthcare enterprise providing training, computer-based learning modules, but lacking in the full complement of resources that a community college provides. The more hospitals and healthcare enterprises situate themselves as educational institutions (e.g., resident training, fellowships, cross-training, etc.), the more confusing this is to the employee.
In addition, these assumptions were verified by our cardiac sonographer manager interview:
We stress ergonomics, and like raising the bed up and using the tools that we have. I also provide a reminder, you know, when you get busy, and you don’t want to take the time, try to take the time because it’s going to save you in the long run.
Theme 2—Injury Education
The second theme describes participants’ suggestions to increase injury education throughout the field of sonography, which was categorized in two ways. The first category of suggestions was to raise supervisors’ awareness of the commonness of workplace injury for sonographers and the gravity of the pain caused by frequently performing scans. The second category referred to improving injury prevention education for sonographers in training.
Category 1: Supervisor Awareness
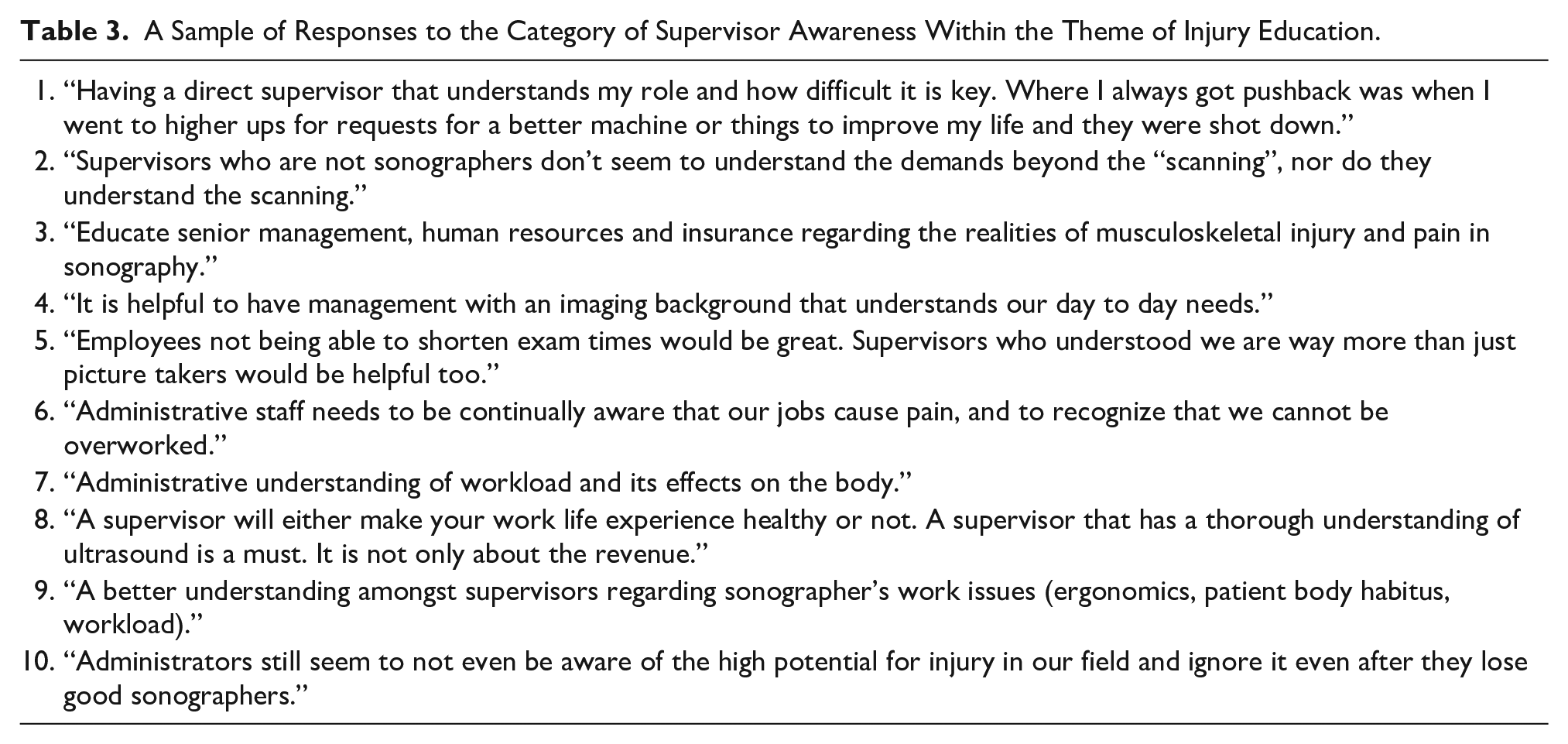
This first aspect of education identified from participant responses referred to educating people in supervisor roles to better comprehend the physical exertion demanded by the exams that sonographers perform. In their survey responses, numerous respondents noted a perceived lack of supervisor knowledge, suggesting that increasing supervisor knowledge of sonography could improve sonographer health (see Table 3). This suggestion is related to a specific sentiment within participant responses that the high number of exams assigned to sonographers by their supervisors results from supervisors not comprehending what performing sonography requires of an employee.
A Sample of Responses to the Category of Supervisor Awareness Within the Theme of Injury Education.
In the first cycle coding, one researcher referred to this repeated sentiment as “Proposing that supervisors should understand sonography work (and its proclivity to injury).” The rich context provided by respondents enabled a deeper understanding of the conflict experienced by many sonographers. Several respondents felt that the severity of the physical pain and potential for injury stemming from the job of a sonographer was not taken seriously by upper management, because it was not well understood by leaders who were not trained as sonographers. Overall, participants expressed that supervisor/manager/administration awareness of WRMSD and the physical demands of sonography were vital to promoting safe practice and preventing injuries. The cardiac sonography manager’s interview verified this:
I think this is true. They’ve worked their way up in management, even if they started out on a clinical end, and some of them haven’t, though some of them are more business, and so they’ve never experienced the clinical aspect of health care to the degree that we’re experiencing it.
Category 2: Sonographer Education Reform
The second category was centered on injury education that is provided for sonographers. In this category, suggestions underscored the current standard of education regarding WRMSDs and, more broadly, the physical strains common for practicing sonographers. One participant stated, “There is not enough information out there about how physical fitness, core strength, [and] mobility affects our ability to perform our jobs with less injury over time. This needs to be taught starting in [sonography] programs.” This sentiment was repeated by this respondent, “In my experience, students and younger sonographers are educated on the importance of good ergonomics and exercise, massage, chiropractic care, etc., but don’t seem to apply that knowledge until hurt.”
In some cases, respondents indicated that sonographer education curricula that cover injury awareness and prevention are incomplete. One researcher discovered this through memoing: “The reliance of some employees in the healthcare enterprise to provide community college resources is not an unrealistic expectation, given that these employers are taking on an education mission. Which is it, a hospital or an educational institution?” This was also verified by the interview with the OB/Gyn manager: “I haven’t seen a lot offered (ergonomics training), I guess sort of didactic training, or more of like the here’s research studies. These are ways that you can help prevent this.”
Theme 3—Individual Habits
This third theme describes participant suggestions that implicate individual control over health and the everyday decisions sonographers can make that have implications for their health outcomes, including protective action against WRMSD.
Category 1: Personal Control
Personal control was implicated throughout participant suggestions to focus on individual habits that can help lower the risk of WRMSD. One of the respondents shared this:
A healthy body is very important. Stretching and loosening up is very important. Have to contort our bodies and extremities many times to get what we need for the exam. This can be very tiring on the body. A healthy mindset is also important. Can’t worry about things that we have no control over.
The suggestions that fell into this category explored a lens that differed from direct requests for assistance or resources. Instead, participants focused on the individual habits that sonographers are solely responsible for and their importance in reducing their risk of WRMSD. It is worth noting that when participants were asked to make suggestions about collective sonography users’ health and well-being, some participants chose to emphasize their personal improvement of healthy habits and chose to focus on their individual control, as opposed to “worrying about what they have no control over.”
Within other participant responses, personal control was implicated not as the sole determinant of health and injury prevention, but as a determinant of the success of other solutions including ergonomics training and other work-provided resources intended for health betterment. An example is this statement, “Without the proper self-care that goes into taking the stress out of your body (exercise, mindfulness, healthy eating), all of the ergonomic and mental health training in the world won’t help.”
These responses on individual control and fostering methods for lowering the risk of injury were also noted in the researcher’s memo: “My personal experience as a middle manager has been that individual behavior is discretely that employee’s issue, but it can quickly color the team’s mood and ability to work.” The cardiac sonography manager’s interview also verified this idea: “You have to stick to your guns, and you have to do this for yourself, because if you don’t do it, nobody’s gonna do it for you. Once again going back to management, you gotta look out for yourself.”
Theme 4—Ergonomics Training Constraints
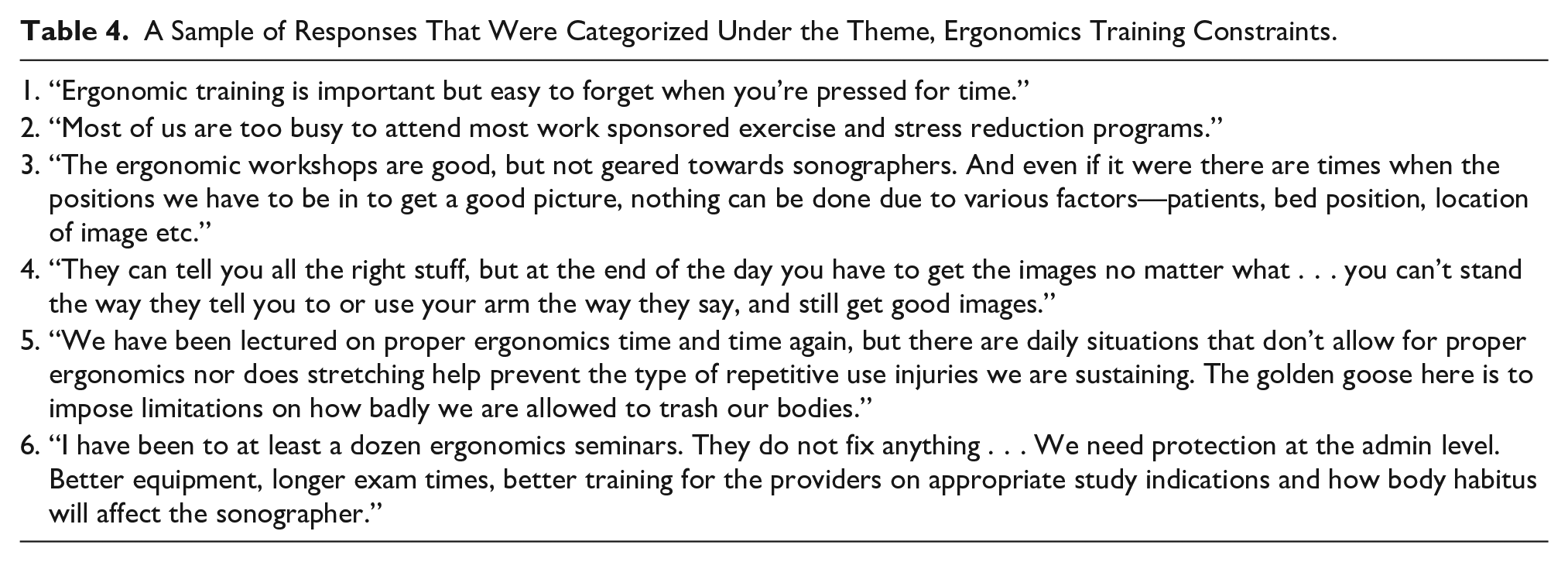
Ergonomics training is well-established as an important factor in WRMSD prevention in sonography. It is, therefore, not surprising that ergonomics was commonly mentioned throughout sonographers’ responses to the survey. Interestingly, some comments that pointed out the limited success of such training and related workshops introduced the suggestion to improve the applicability of ergonomics, as it was conveyed to them, to real-world work conditions. The effectiveness of ergonomics training workshops is debated throughout survey responses where its applicability constraints were implicated (see Table 4).
A Sample of Responses That Were Categorized Under the Theme, Ergonomics Training Constraints.
Category 1: Limited Applicability
Several respondents indicated that there were time constraints on sonographers’ ability to apply lessons learned from workshops under real-world conditions, as well as their ability to attend workshops. Many respondents expressed the sentiment that the information they are learning from the ergonomics training they are provided does not directly apply to their daily situations. The overarching concern was that sonographers perceived limitations in applying ergonomics effectively. In many cases, what was presented was not within a sonography context, and effective training is not a one-size-fits-all solution for sonographers. The interview with the OB/Gyn sonography manager covered this extensively:
I would describe our training as sonographer-to-sonographer training, as least part of it, especially when we hire a student. When students are hired like right out of school. I think that younger sonographers are sharing more, I think, like I said before, what they kind of do and what’s available in the room.
Theme 5—Guidelines and Standards
The participant suggestions that were made to improve the health and wellness of their colleagues, based on workplace administration and training practices, were labeled as Guidelines and Standards. This theme encompasses the suggestion that lab and educational accrediting organizations should play a more active role in determining and defining an appropriate workload and, to an extent, enforcing how sonographers spend their time. In sonography, the term “accrediting organizations” broadly referred to those agencies that participants mentioned as providing oversight for quality in sonography education and clinical laboratory services. The participants mostly mentioned the Joint Review Committee on Education in Diagnostic Medical Sonography (JRC-DMS), which reports to the Commission on Accreditation of Allied Health Education Programs and the Intersocietal Accrediting Commission’s (IAC) clinical accreditation for cardiac and vascular labs.
Some participants framed their suggestion to increase the involvement of influential accrediting agencies in a broad way, with few specific suggestions for what exactly they want accrediting agencies to enforce, “More support from accreditation and registry societies to educate and enforce standards.” Statements such as this one let us know that participants are witnessing what they perceive as examples of subpar or problematic practices in the field, and that they believe authoritative organizations may be influential enough to promote healthier standards. Other responses provided insight into what specific standards sonographers want accrediting agencies to help enforce, leading us to specify “Limiting Exams” as a category of limits and guidelines.
Category 1: Limiting Exams
In the overarching theme of limits and guidelines, participants have suggested that laboratory accreditation establish limits for the number of exams each sonographer is expected to perform each day and provide longer appointment times to complete exam protocols. A specific limitation some participants implicated within this broader suggestion included limiting the number of patients with obesity that sonographers could examine each day due to the physical strain required to scan people with a greater body mass index. These suggestions were made to improve the quality of their practice and reduce physical harm to themselves. One participant stated, “[It would help if] accreditation organizations set guidelines for exam times that reflect the protocols for each exam and patient medical conditions and body habitus.” This participant provided additional detail,
I think national organizations could do a better job to set guidelines to limit # of scans or scanning time, [and] structure schedules better for time before or after each exam. Unfortunately, so many institutions have such pressure from administration to get more tests done in [a] shorter time, and the sonographers are paying the price.
Participants suggested using guidelines set by accrediting agencies to get workload limits recognized and enforced by their employers. Without enforcing such standards, some sonographers feel they will continue to feel the pressure to meet productivity expectations, which takes a heavy toll on their bodies. It was interpreted that respondents’ calls for lab accrediting organizations to standardize longer exam times and fewer daily exams was an implication of sonographers’ perceptions that directly requesting these changes from their supervisors would not be as effective or has been attempted with limited success. Indeed, this may be related to sonographers’ perceptions of their supervisor’s valuing quantity over quality. One participant put it this way: “Supervisors have to support the health and well-being of the sonographers more and less to hospital bottom lines. Stop focusing on the number of exams done and focus on the quality of exams.”
The request for standards from the accrediting level may also reflect that many supervisors have limited control over certain productivity standards, and therefore sonographers feel inclined to reach beyond their direct administration to accrediting agencies. It is important to point out that WRMSD standards have been developed (and/or cited) by not only lab and facility accreditation bodies (i.e., ACR, AIUM, and IAC) and programmatic accreditation (e.g., CAAHEP), but also by professional societies (AIUM, ASE, SDMS, SVU, etc.), and credentialing organizations (i.e., ARDMS, ARRT, CCI). Regardless, some sonographer responses communicate a perceived benefit to receiving guidelines from authoritative organizational levels and believe this may assist with achieving a desired change within their local work environment.
Even where accrediting agencies’ role was not directly implicated, sonographers emphasized exam time as a key factor in both sonographers’ and their patients’ health outcomes. This was expressed as follows, “Exam times should be lengthened to accommodate the administrative time needed prior to and after an exam . . . The stress of getting patients in and out in 30 minutes is detrimental to the tech and produces poorer patient results.”
These expressed needs were also noted during the memo phase of analysis and recorded as follows (see Figure 1):
Healthcare is a larger multi-layered enterprise, and it reminds me of trying to play 3D chess. The employer is being asked to make changes on several levels of the enterprise: the sonography lab, the department/administration, and external agencies (e.g., lab accreditation). When you play 3D chess each move has consequences on the level you are playing and on levels above or below.
A sample of memoing during the qualitative analysis by one of the researchers.
The need to reach out to accrediting agencies was also not clearly understood by our OB/Gyn manager,
I don’t even know if that’s something that these accrediting organizations . . . is that even on their radar to be doing? I mean we’re accredited through AIUM in Maternal Fetal Medicine. I just feel like that’s all of that stuff is so much more based on image quality. And this is what your images should look like. And this is, you know, what you should be doing for these protocols.
Conceptual Mapping and Proposed Grounded Theory
Given the extensive data collection, analysis, and triangulation (manager interview and memos), it became evident that the Moray model, “Ergonomics as the study and design of sociotechnical system” could be applied to the categories to identify trends in the solutions communicated by the study participants. 27 A modified model was developed to serve as a conceptual map for understanding the implementation of solutions to support the health and well-being of the sonography workforce (see Figure 2). In the adapted model, the exam room, physical ergonomics, and individual behaviors are placed in the center since these factors directly influence the risk of work-related injury. However, this inner core is surrounded by multiple levels of influence that affect the workplace and activity within, including the team, organization, legal, and broader culture layers.
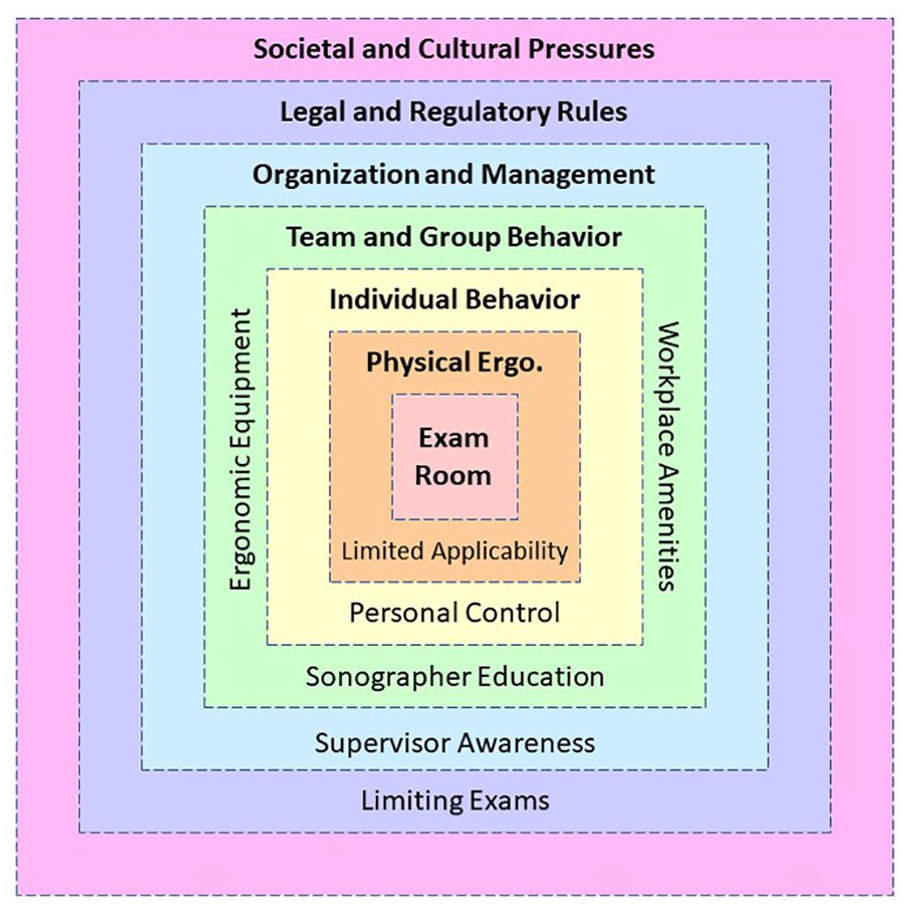
An adapted model that was created as a conceptual map during grounded theory analysis in the current study. This revision allows for sonography and vascular technology expressed needs for ergonomic assistance to be properly situated in a study and design of sociotechnical systems.
The multi-step analysis of survey responses, memoing, interviews, and conceptual mapping has resulted in a proposed grounded theory: Risk Reduction Relies on Proper Employee Representation. Specifically, when placing the themed categories within layers of the sociotechnical systems model and considering how the borders between each level are perforated, the inward-out and outward-in influences of the core aspects of WRMSD, within the individual workspace, become apparent. Adapting the exam room or relying on individual worker behavior is insufficient to address injury prevention. Instead, reducing risk must include meaningful awareness, employee representation, and actions throughout all the system layers, including the workstation, individual workers, teams, organizational administration, accrediting and legal agencies, and socio-cultural norms.
Discussion
Through this inductive process, five major themes were constructed based on the responses provided by practicing ultrasound professionals to the two open-ended questions about sonographer health and well-being. A resulting grounded theory, risk reduction relies on proper employee representation, was constructed using the participant suggestions. This theory emphasizes the importance of understanding the risks that are part of performing the duties of sonographers and vascular technologists.
“Risk reduction relies on proper employee representation” helps to decenter the emphasis on the sonography professional and instead look at organizational and management behavior and regulatory agencies for assistance in reducing the risk of WRMSD. One effort to reduce risk was the publication of Industry Standards (I and II) to push for changes in physical devices and address physical ergonomics.30,31 Although these efforts were important and likely significant, the need to move further externally for change is still needed. Another example is the AIUM’s recently published 2023 practice principles, where the present study themes overlap with numerous guidelines for WRMSD prevention. For one, the AIUM recommended workplace injury-prevention policies that provide physical and mental health resources and ergonomics training, 20 all of which match the resources suggested by sonographers, as discussed in Theme 1—Resources and Equipment.
In addition, since guidelines from the AIUM target workplace culture and policy at the individual workplace level, these recommendations are arguably intended for supervisors, managers, and sonographer employers broadly. Guidelines that are aimed at employers, as opposed to solely being directed at sonographers themselves, demonstrates a shift toward WRMSD prevention approaches that go beyond an emphasis on individual behavior change. The provision of these guidelines by an accrediting organization, such as the AIUM, potentially satisfies suggestions discussed under Theme 5—Guidelines and Standards. We acknowledge that responses to the survey analyzed in this manuscript were recorded in 2022 before the 2023 practice principles were published and had adequate time for distribution throughout the workforce, which can take considerable time.
Another critical issue that was expressed was the ongoing need for injury-prevention education. The current state of the curriculum is discussed in the 2023 practice principles within the statement, “Education on the prevention of WRMSD is currently part of accredited sonographer education, however, the level of detail can be quite variable; and education should be continued throughout one’s scanning career.” 20 The variability of education was implicated by sonographers’ divided comments on WRMSD-prevention education as discussed in Theme 2—Injury Education, with some respondents feeling ergonomics education for injury-prevention was not contextualized in ways that reflected the work of sonographers and vascular technologists. Therefore, our findings align with the statement provided by the AIUM that WRMSD-prevention may not currently be emphasized enough in sonographer curriculum.
The goal of reducing the prevalence of WRMSD among sonographers and vascular technologists has yet to be realized, and workers, on an individual level, are limited in what they can do to protect themselves when the work environment (e.g., equipment, workspace, and work schedule) provides limited support. This is evident by looking closely at the conceptual map, influenced by the Moray model. 27 Moray’s systems model of ergonomics provided a foundation for exploring the levels of influence that play an interconnected role in determining sonographer health outcomes related to injury-prevention solutions.
The highest level (represented by a pink square in Figure 2), Societal and Cultural Pressures, affects the other levels of influence because everyone living in an organized society is under social pressures and norms. None of the themes determined based on this dataset fall directly into this broad level, yet social pressures influence the solutions situated in the other levels, from the legal and regulatory rules that sonographers work under to the group and individual behavior they partake in within the workplace. Hays’ description of social structures is particularly helpful for understanding the societal level of our adapted Moray model; she describes structures as having both constraining and enabling effects that shape the thoughts and behaviors of individuals living in an organized society. 32
Within the nested model, it was important to park the category “Limiting Exams” in Legal and Regulatory Rules, a suggestion made by sonographers while requesting direct action from accrediting agencies, within the field of sonography. This acknowledges these participants’ suggestions that limited numbers of exams per sonographer and extended appointment times are needed to promote health and wellness. It is likely that these needs have not been met within the next level of influence, Organization and Management, as identified in the “Supervisor Awareness” category of participant responses. In this category, respondents expressed that managers of sonographers and vascular technologists need to be more educated on the risks of WRMSD in the field. It is possible that these comments were made by workers being supervised by non-sonographers or middle managers with limited healthcare experience. Therein lies the challenge to make these supervisors and manager acutely aware of the risk of career-ending injuries. This level certainly has great impact on work teams and their group behavior.
The “Sonographer Education” category is listed within the Team and Group behavior level, given that the employer needs to contextualize this instruction to the specifics of the work being conducted. Currently, sonography educational curricula vary across educational institutions. A baseline curriculum, specific and applicable to sonography, would likely be beneficial and could be supplemented with in-services and risk reduction seminars tailored specifically to exposures that may occur in specific workplaces. Additional categories that were identified included ergonomic equipment and workplace amenities. Nested deeper in the adapted model is Individual Behavior, where it was important to situate the category of “Personal Control.” Finally, within Physical Ergonomics is the category of “Limited Applicability.” This placement is made given that participants described the constraints of applying general ergonomics principles to their daily tasks.
In the adapted model, the inter-level and potentially bi-directional influence is represented by dashed boundaries defining each level. The porous nature of the systems model to account for the influence of individual behavior for workplace injury-prevention concurs with the findings of Lecours, who investigated preventive behaviors at work and found that while preventive behaviors are individual-level actions, individual actions are multidimensional in the way that they affect various levels of injury-prevention. 33 The next steps are to intentionally use the adapted model to address the expressed needs of the participants who provided this important data. The individual worker and their team only have a limited influence in reducing the risk of WRMSD. As the adapted model illustrates, the focus must be directed on those levels beyond the control of the individual sonographer and their work team. To fully address the persistent 80% to 90% prevalence of work-related musculoskeletal symptoms in ultrasound professionals, it is paramount to expand and focus efforts and understanding on the part of individuals with agency within these outer and higher levels of work-related influence.
Limitations
As a grounded theory study, the analysis was conducted thoughtfully and rigorously. The researchers pursued member-checking by interviewing managers who responded to the survey and were willing to verify and expand on the categories and themes discovered. It is also important to acknowledge the limitation that responses in these data may not represent sonographers across all practice settings. These results are exclusive to this cohort and should stimulate new directions for professional associations, accrediting bodies, and hospital systems to address the risk of WRMSD among sonography professionals.
Conclusion
Through the rigorous process of grounded theory analysis, it was possible to determine several salient themes based on the suggestions offered by survey participants. Many uncovered themes concur with and expand upon the practice principles published by the American Institute of Ultrasound in Medicine. 20 The postulation of the grounded theory, risk reduction relies on proper employee representation, was informed by conceptual mapping of the themes and categories into an adapted sociotechnical systems model of ergonomics specific to sonography practice. Using the adapted sociotechnical systems model will facilitate further development of solutions and approaches to WRMSD prevention in sonography, considering multi-layered influences across the entire system. Future work should explore the extent to which the AIUM’s practice principles are implemented within the workplace across all levels of influence and their success at reducing WRMSD risk factor exposures.
Footnotes
Ethics Approval
Ethics approval for this study was obtained from The Ohio State University’s Social and Behavioral Internal Review Board (IRB#2021B0113).
Informed Consent
Written informed consent was obtained from all subjects before the study.
Animal Welfare
Guidelines for humane animal treatment did not apply to the present study because no animals were used during the study.
Trial Registration
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study has been provided by the following members of the WRMSD Grand Challenge Alliance with additional financial support from Biodex, part of Mirion Technologies. The views presented in this study are the authors and do not necessarily represent those of the supporting organizations: American Institute of Ultrasound in Medicine, American Registry for Diagnostic Medical Sonography and Inteleos, American Society of Echocardiography, Intersocietal Accreditation Commission, Joint Review Committee on Education in Cardiovascular Technology, Society for Vascular Ultrasound, Society of Diagnostic Medical Sonography, and Society of Diagnostic Medical Sonography Foundation.
Peer Reviewer Guarantee Statement
The Editor/Associate Editor of JDMS is an author of this article; therefore, the peer review process was managed by alternative members of the Board and the submitting Editor/Associate Editor had no involvement in the decision-making process.