
Abstract
A bursa is a thin sac filled with viscous fluid to facilitate friction and gliding. In the human body, there are two types of bursae: synovial bursae in well-defined positions and adventitial bursae, which develop in sites where friction or pressure increases. This case study is on a young woman with an old distal radial extremity fracture, with occupational exposure to pressure on distal ulnar forearm. She noticed a small and painful mass, with some mobility on the above-mentioned site. Sonography was used to detect a small fluid accumulation with features of adventitial bursitis. This case presents a rare localization of an adventitial bursitis. It is believed to have developed over the distal ulnar epiphysis, with a small bone malalignment, after an old and consolidated fracture, of the distal radial extremity.
A bursa is a thin sac filled with a small line of viscous lubricated fluid. Bursae are found on certain anatomic areas to reduce friction and/or to provide resistance-free movement of body segments. Bursae are classified as native and non-native. 1
Native bursae, also called anatomic or synovial bursae, share common traits. They form during embryonic life in specific areas, although they may vary in position and number. Their wall is lined by a synovial membrane with two layers. The deep layer consists of fibrous connective tissue and vessels and the superficial layer contains synovial cells in an extracellular matrix. The synovial cells are responsible for the secretion of the capillary film of lubricating fluid, which allows gliding of both the superficial and profound walls on each other to minimize friction. 2 Synovial bursae, according to their position, are called subcutaneous, subtendinous, submuscular, and subfascial. Sometimes synovial bursae may communicate with the subjacent joint.
The non-native bursae, called adventitial or adventitious bursae, form later in life as a response to repetitive stress. They occur by accident, hence their name accidental bursae. Their position is rather superficial, in the subcutaneous fat, and lack the synovial lining and the synovial fluid. The fluid inside adventitial bursae is due to vasodilatation and extravasation of serum proteins and extracellular fluid into the bursa. 3 Foot is one of the most involved sites of adventitial bursa.
Inflammation of a bursa is bursitis. This condition may arise as a primary event in certain rheumatic condition due to the inflammation of the synovial membrane or as a secondary event to a repetitive trauma. The distinction between the two situations may be difficult.
This case illustrates an adventitial bursitis in a rare localization, on the ulnar edge of the distal right forearm as a result of professional repetitive stress.
Case Report
This case is of a 46-year-old woman, a computer technician, working around 10 hours/day on the computer desk. She was known to have had a fracture, of distal right radius, 10 years ago. It was treated with cast immobilization for a period of 6 weeks. Fracture consolidation occurred with some axial malalignment of the bone. She had no complaints during this time (Figure 1). On the posteroanterior radiograph of the wrist, in pronation, a small increase in the ulnocarpal space was noted. There was some degree of demineralization of the carpal bones.
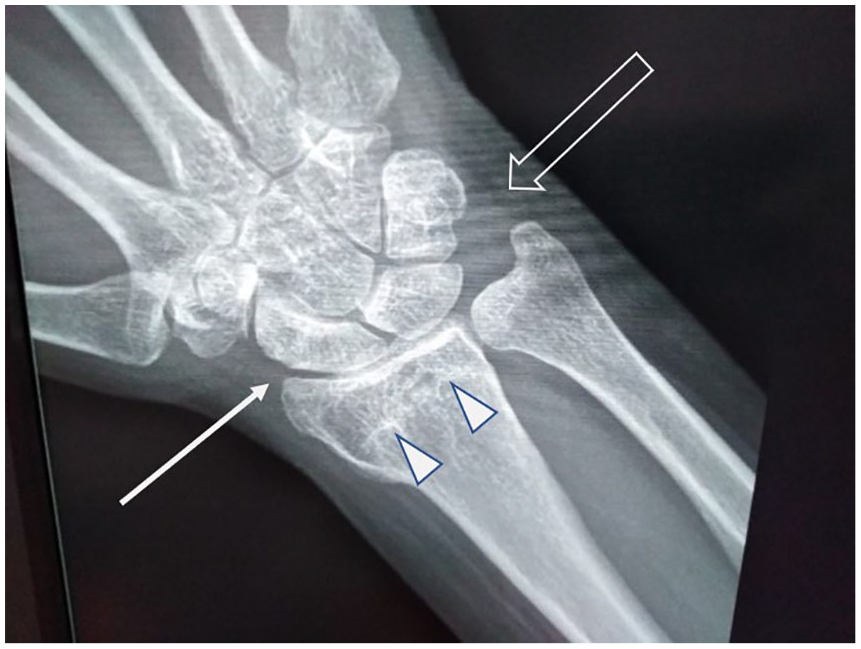
A radiograph of the distal right forearm. The callus of the old fracture is visible on the distal extremity of the radius (void arrows). The carpal displays some increase in radiotranslucency. The articular space between the distal extremity of the radius and the carpal bones is reduced (white arrow); in the meantime, the space between the distal extremity of ulna and triquetrum is widened (void arrow). There is deviation on both bones in the radial direction.
Two months ago, she noticed a little subcutaneous mass on the distal portion of the forearm, on the ulnar side, just proximal to the wrist. The mass was painful, and she reported a pain score, on visual analogue scale (VAS), of 5–6 at rest and of 7–8 at palpation and mobilization. Local discomfort was accentuated by prolonged lying on the cubital side of the forearm, when working at her desk. There was neither local warmth nor redness at the site (Figure 2).
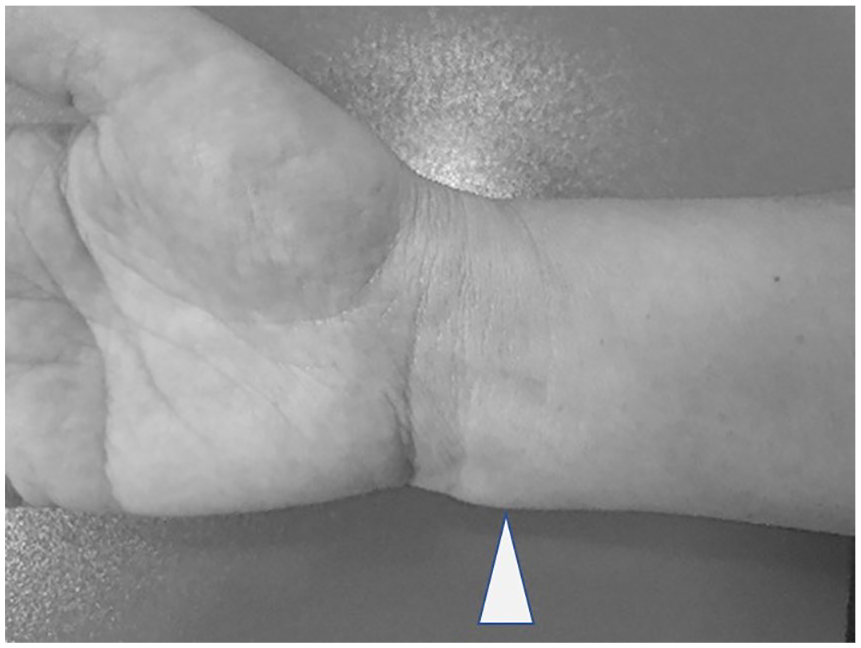
The distal extremity of the forearm with a small mass on the radial side (arrowhead).
After obtaining an informed consent from the patient, further investigation was pursued. A gray-scale sonogram was performed with a Toshiba Applio ultrasound machine and a 14-MHz linear-array transducer. The sonogram was performed on the longitudinal axis of the cubital margin of the forearm, parallel to the cubitus and on the transverse axis. 4 On the long-axis view, in the subcutaneous fat over the ulnar styloid, lay an ovoid mass. The mass had a well-defined outline and a coarse internal echostructure, with both anechoic and hypoechoic regions. Sonopalpation revealed partial compressibility of the mass. On the short-axis view, the mass in the subcutaneous fat was positioned lateral to the tendon of flexor carpi ulnaris. There was no sign of local hyperemia which was documented by a lack of internal flow, using color Doppler. The size of this mass was 11.5 mm × 9.5 mm × 4.4 mm (Figures 3 and 4).
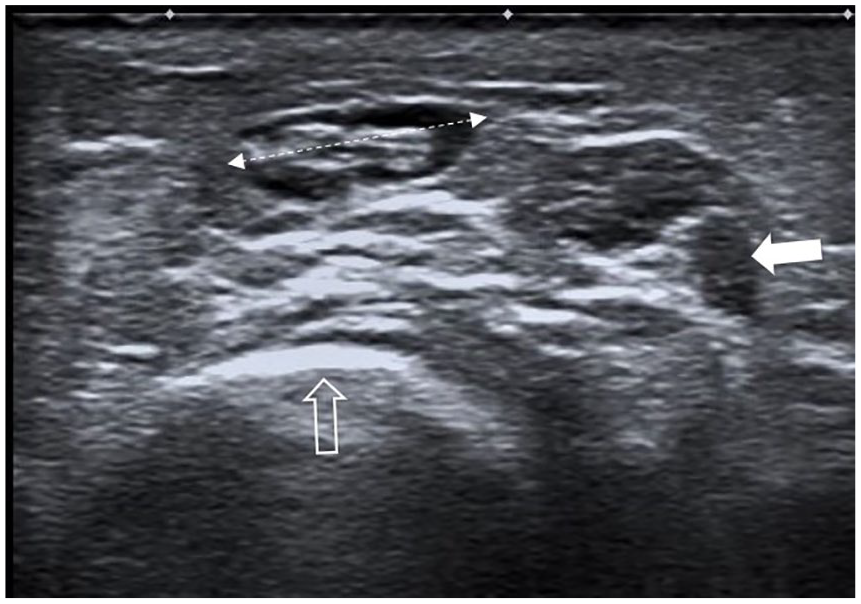
Short-axis sonogram of the distal forearm. The mass between the calipers situated in the subcutaneous tissue, with well-circumscribed walls and a heterogenous content, hypoechoic and isoechoic, over the distal extremity of the ulna (hollow arrow) and lateral to the flexor carpi ulnaris tendon (white arrow).
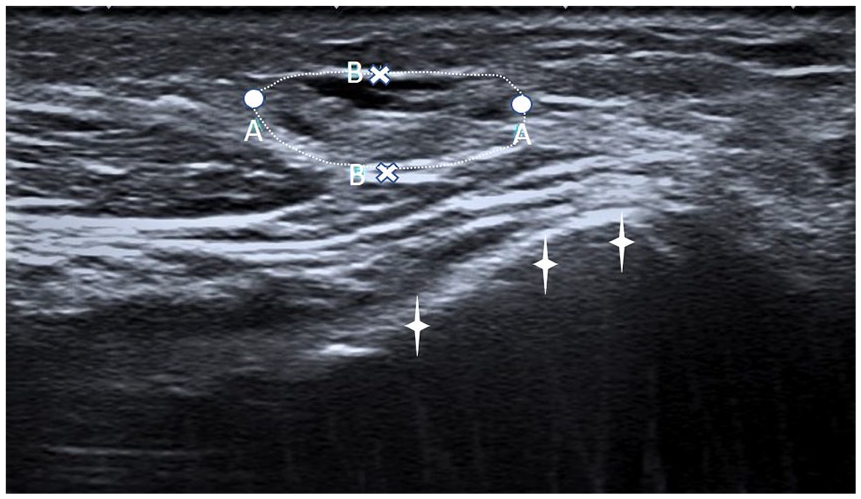
Long-axis sonogram over the distal extremity of ulna (periosteum marked with white stars). In the subcutaneous fat, there is ovoid mass (dashed contour) with a mixed structure, hypoechoic and isoechoic. AA, 11.5 mm; BB, 4.4 mm.
Discussion
In the case of a subcutaneous mass on the distal ulnar edge of the forearm, the clinician may consider a list of diagnostic differentials. An abscess is accompanied by local inflammatory signs, and the skin integrity must be checked to identify an entry point. A lipoma is a frequent condition with specific features on ultrasound scanning. A ganglion cyst is closely related to a tendon sheath or a joint; they occur frequently near the scapholunate joint. The communication with the tendon sheath or the articulation may be visible during sonography. This patient’s cystic mass was well-circumscribed, and the structure was anechoic and possessed some internal echoes or septae. It was noncompressible. Some of these cystic masses may occur due to a posttraumatic event. 5
Other types of soft tissue masses deriving from local tendons or nerves are visualized by sonography and require searching for the connection to a particular structure. Thrombosis of the superficial veins, especially on this area exposed to professional trauma, has local clinical signs, and sonography with color Doppler can be diagnostic. Adventitial bursitis is an infrequent diagnosis, after exclusion of the above-mentioned situations.
The above-described mass was considered an adventitial bursa. This specific localization over an osseous surface with mild anatomic deformation was likely due to the patient’s professional activity. The patient was working with the wrist and distal forearm resting on a hard surface (the table). Based on a general search of the literature, there are no other reports of an adventitial bursitis on the ulnar side of the distal forearm.
The mechanism of this bursitis is due to the prolonged pressure and friction between the ulnar edge and the rigid surface of the table. In addition, the poor alignment of the distal ulna may be an aggravating factor.
The sonographic aspect of the mass was similar to the description of previous adventitial bursitis in the literature: ovoid mass with well-defined walls and a heterogenous echotexture, both anechoic and isoechoic, with some compressibility, suggesting a complex fluid collection.6,7
The literature describes different localizations for adventitial bursae. The most frequent are the foot and the ankle, over the bony prominences: medial eminence of the first metatarsal head and plantar aspect of the metatarsal heads. In the amputated limbs, the stump may develop such adventitial bursitis. 8 There is no mention for such a peculiar localization of an adventitial bursitis over the distal ulnar epiphysis. In this particular case, this appearance may be considered as a professionally induced pathology.
Among information technology professionals, the literature documents tendinopathies and entrapment neuropathies as a frequent occurrence, with repetitive trauma and improper support being the contributory factors. 9
Conclusion
Adventitial bursae are accidental fluid accumulation in the soft tissue in areas where prolonged and repetitive trauma or shear forces occur. The development of this adventitial bursa, on the ulnar side of the distal forearm, with a mild bone malalignment, and exposure to work-related stress, could have been contributory.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.