
Abstract
Purpose:
Document a feasibility study of an interprofessional approach to targeted sonography training (TST) for medical students, incorporating computer-based simulation (CBS).
Procedure:
Three participants received TST on the abdominal aorta from credentialed sonographers using CBS. Training included didactic instruction, skill demonstration, debrief, and feedback. An assessment template was developed to assess students’ skills and provide structured feedback. Students completed a feedback survey on the learning process that followed the training.
Results:
Students’ template scores were similar, despite varying prior exposure to CBS. The importance of deliberate practice, direct feedback when a student is struggling, and a debrief session following skill demonstration was evident in this study. Students agreed that this targeted instructional process provided a low-pressure environment where they could learn from mistakes and improve their confidence.
Conclusion:
This case series demonstrated how readily a TST session can be accomplished using computer-based simulation and the value of structured feedback.
Keywords
Advancement in sonographic technology, affordability, portability, and recognition of the applicability of sonography as an imaging modality, for diagnostic and interventional purposes, has resulted in its rapid increase in use among medical specialties. 1 With the growing use of point-of-care ultrasonography (POCUS), focused sonographic assessments performed and interpreted by physicians bedside to provide rapid diagnosis, the American College of Graduate Medical Education (ACGME) requires POCUS training for accreditation of emergency medicine residency programs. 2 This has inspired many undergraduate medical educators to also incorporate sonography training into their programs. The integration of sonography into the national curriculum for medical students has been advocated, and suggested methods for implementation have been published.3–5 Yet, the level of sonography exposure can vary greatly among medical programs from adoption of longitudinal curricula designs to targeted sonography education with a goal of improving knowledge and skill in a specific area, typically within a short period of time.4–7 Bahner et al. 8 found that one of the top barriers that curricular administrators of US MD-granting medical schools face in incorporating sonography training into the curriculum is the lack of space in the current curriculum. Nevertheless, programs that are unable to fully integrate sonography training into their curriculum may have an opportunity to supplement more limited exposure to sonography through interprofessional collaboration with an academic or hospital-based imaging department. In particular, this report describes an interprofessional approach to targeted sonography training (TST) of medical students that incorporated computer-based simulation (CBS).
Simulation-based medical education is recognized in the literature and among medical educators for promoting health care professionals’ performance and providing an opportunity to learn from errors.9–13 McGaghie et al. 10 conducted a review of the published literature from 1990 to 2010 on the comparative effectiveness of simulation-based medical education with deliberate practice (DP) and discovered that simulation coupled with DP was superior to traditional clinical medical education for learning a variety of skills, including central line insertion, various laparoscopic surgical skills, and advanced cardiac life support. McGaghie et al. 14 published an update of their earlier work, a systematic review of the same topic that spanned from 2003 to 2009. This systematic review provided added publications over the six-year span that contributed to a best practices document describing a total of 12 features and best practices, 14 which was extended from their original list of five: curriculum integration, feedback, simulation fidelity, deliberate practice, and outcome measurement. Furthermore, high-fidelity computer-based simulators can augment traditional learning methods to improve students’ knowledge and psychomotor skills. A meta-analysis by Cook et al. 12 demonstrated that students who participated in technology-enhanced simulation compared to those with no intervention demonstrated better learning outcomes in both knowledge and skills. Kusunose et al. 15 found that medical students who underwent computer-based sonography simulation training subsequently acquired higher-quality images when scanning a standard patient than those who had only traditional textbook-based learning. Another study found participants (six medical students and six residents) to have an accuracy of 93% in interpretation of POCUS simulations after focused training with CBS. 16 In addition, qualitative reporting from diagnostic medical sonography (DMS) students and clinical mentors highlights the advantages of computer-based sonography simulators that provide students the opportunity to develop basic psychomotor skills in a safe and unpressurised environment before scanning patients in the clinical setting. 13
Based on (1) a desire to increase training opportunities for medical learners in programs that are unable to fully incorporate sonography throughout the curriculum and (2) the evidence in the literature supporting the benefits of CBS, through a limited case series the authors present an interprofessional approach to TST, consisting of didactic instruction, skill demonstration using a high-fidelity computer-based sonography simulator (Vimedix simulator; CAE Healthcare, Quebec, Canada), debrief, and feedback.
Materials and Methods
Educational Preparation
The students who were recruited to this feasibility study were all actively enrolled in a midwestern land-grant university with a medical school. 17 The medical school is a 2018 midwestern ranked program that provides a four-year medical doctorate degree and has an embedded limited vertical sonography curriculum that also includes levels of elective curricula: beginner, intermediate, advanced, and honors ultrasound. As part of the medical curriculum, students are provided with both didactic lectures and hands-on laboratories. Beginner level includes an introduction to basic ultrasound physics, knobology, and identifying basic anatomy. Intermediate and advanced levels include multiple POCUS examination techniques and advanced knobology, such as Doppler, M-mode, and optimizing the image. The honors ultrasound level is the keystone course for medical students interested in advanced training during medical school. This course includes monthly didactics covering multiple POCUS uses, hands-on sessions to practice image acquisition, review sessions on relevant pathology, and journal clubs to review current literature. During hands-on laboratory, students are placed in groups of three to four per station, and each station is facilitated by an upperclassman involved in the elective curricula, a resident, or ultrasound faculty. The facilitators start the session by providing a brief overview of the anatomy by scanning a volunteer and capturing views for students to replicate. On select examinations, such as echocardiography and gynecology, low-fidelity phantoms and a computer-based simulator (HeartWorks; Intelligent Ultrasound Group, Cardiff, Wales) are available. This is followed by students taking turns during hands-on scanning. Based on observation, it was noted that the level of feedback and direction during and after students’ scanning varied between facilitators. As such, the authors saw an opportunity to develop an assessment template to support this targeted training. Facilitators could use the template during and after students’ skill demonstration to provide debrief sessions that are consistent and provide focused feedback.
Assessment Template
An aortic examination is listed in the proposed national sonographic curriculum for medical students and is a common examination performed by medical professionals to rule out aneurysms in the emergency department. 5 The medical students were also exposed to didactic material regarding aneurysms in their curriculum, and as such, an aorta examination was selected by the authors as the focal topic for this targeted training. In creating an appropriate aorta assessment tool, the authors referenced the AIUM Practice Parameter—Ultrasound Examination of the Abdominal Aorta in Adults, which provides parameters that must be included in an abdominal aorta examination and was developed collaboratively by the American Institute of Ultrasound Medicine (AIUM), the Society of Radiologists in Ultrasound (SRU), and the American College of Radiology (ACR). 18 The new template was divided into four distinct sections: 2D images of the Aorta, Proximal Aorta Measurements, Mid-Aorta Measurements, and Distal Aorta Measurements. The section on 2D images of the aorta was dedicated to evaluating whether appropriate images were acquired at each segment, at accurate locations, and on axis; longitudinal and transverse views of the aorta were included (Table 1). Longitudinal views were considered on axis when captured images were parallel to the long axis of the aorta. Transverse views were considered on axis when captured images were perpendicular to the long axis of the aorta. This section accounted for 14 of the 35 points for this assessment. The proximal, mid-, and distal aorta measurement sections were each used to evaluate (a) minimum measurements to include an anteroposterior (AP) and width measurement at each segment, (b) measurement location accuracy for each segment, and (c) caliper placement accuracy (measurement accuracy) for each of the measurements. Each measurement section accounted for 7 of the 35 points for this assessment. In addition, the template provided the proctors with a section to mark any pathology the student identified, if applicable. Last, the template contained a microergonomic section to evaluate adjustments made to the height of the bed and monitor display (if adjustments were possible), to allow the person performing the sonographic examination to work in a comfortable posture.
Appropriate Images at Defined Aorta Segments With Corresponding Measurement Criteria.
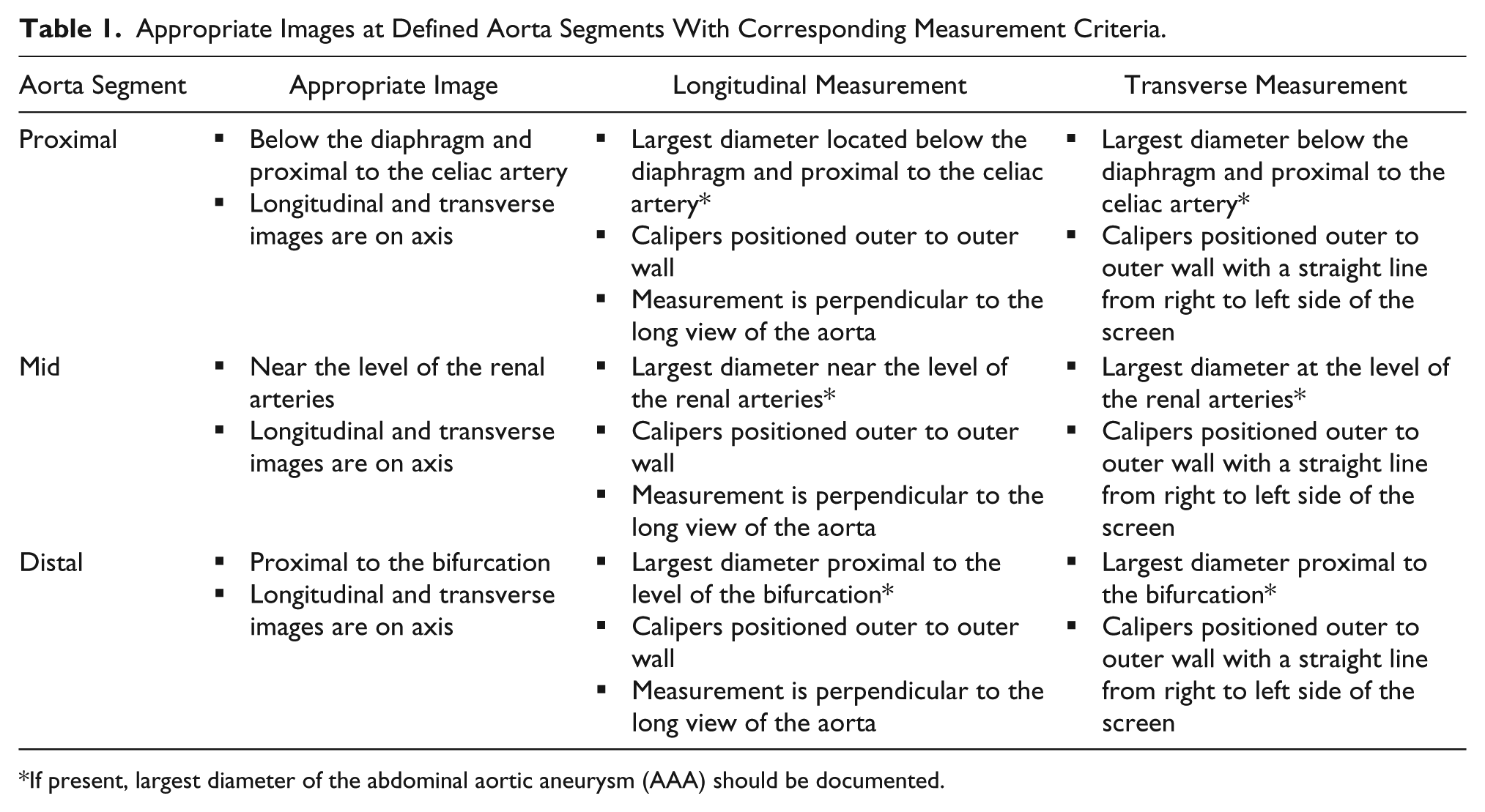
If present, largest diameter of the abdominal aortic aneurysm (AAA) should be documented.
Participants
Student participants were invited to join a feasibility study that was approved by the Behavioral and Social Science Institutional Review Board of the university as an exempt project. Students enrolled in the university as premed, with direct exposure to sonography via a sonography laboratory, and medical students, who were involved in the beginner level of the elective curricula, were provided with an overview of the study and researchers’ e-mail addresses to make contact if they were interested in becoming a participant. Students who wished to participate were verbally assented and, once again, assured that this feasibility study would have no effect on any course grade or academic standing.
Student 1 was a premed student who had recent personal interaction and training on a CAE Vimedix simulator. According to the student, prior to this study, he had approximately two hours of hands-on exposure to scanning the aorta, which included hands-on scanning practice of the aorta on the CAE Vimedix simulator and on a volunteer, with individualized feedback during scanning. The student was exposed to only normal aorta cases on the simulator.
Student 2 was a medical student, year 1 (M1), with a prior personal interaction on the CAE Vimedix simulator. Prior to this study, he reported having between two and four hours of exposure to aorta scanning, which included one-time use of a CAE Vimedix simulator, phantom and volunteer. The student was exposed to only normal aorta cases on the simulator.
Student 3 was a M1 with no previous interaction on a CAE Vimedix simulator. According to the student, he had no prior hands-on exposure to aorta scanning, but he stated that aneurysms were discussed in a current medical curricular course, where corresponding imaging was presented through magnetic resonance imaging (MRI) and computed tomography (CT) scans.
Both medical students (students 2 and 3) had completed the didactic cardiopulmonary content of the first-year program prior to study participation. They had also attended a mandatory sonography scanning laboratory that allowed M1s to practice obtaining cardiac views on volunteers and using the HeartWorks simulator. In addition, they had further opportunities to scan on volunteers and select cases via the HeartWorks simulator through their involvement in the elective sonography curricula. All three students expressed a desire to use sonography in some manner as part of their future clinical practice.
Didactic, Demonstrations, Debrief, and Feedback
All three students were invited by DMS educators (authors S.H.M. and K.D.E.) to a 15-minute didactic session to review the anatomy of the abdominal aorta and introduce key elements of ergonomics when setting up for a sonographic examination. The review of the abdominal aorta and the branches included the use of a diagram and live scanning on a CAE Vimedix simulator, referencing both corresponding sonography and augmented reality displays. After basic anatomy was reviewed, the designations of the proximal aortic segment (superior to the celiac trunk), mid-aortic segment (near the level of the renal arteries), and the distal aortic segment (proximal to the aortic bifurcation) were explained. These were reviewed as guidance for making measurements of the aorta. Instructional demonstration followed, during which one of the authors (K.D.E.) provided a scanning demonstration of the normal aorta on the computer-based simulator. The DMS educator scanned the manikin and demonstrated the desired segments for the three students as they stood together and watched the demonstration. Sample longitudinal and transverse measurements were made by the educator, placing the caliper on the outer margins of the aorta at all three specified locations. Benefits of creating an ergonomically friendly environment were also highlighted and ergonomic adjustments were demonstrated to the students for the simulated task. The examination table was demonstrated for its ability to alter the vertical location of the simulated patient, and the adjustability of the monitor was also demonstrated. A chair was provided if the student wanted to sit or the student could choose to stand to complete the sonographic examination. During the instructional demonstration, students were informed of basic proper ergonomic adjustments that should be made to maintain a relaxed and supported scanning arm, with minimal shoulder abduction and extension, as well as avoiding neck strain by setting the top of the monitor display near eye level. Furthermore, the students were assured that the educators would assist them with equipment-related inquiries, such as saving images during the aorta imaging examination. A postdemonstration question-and-answer session was held for the group before they were separated for the next phase of the instructional process: student demonstration of skills. The students not examining the aorta were asked to go into an adjacent office to wait while their colleague was assessed. No communication between students was permitted once student demonstration commenced.
Prior to students reentering the laboratory to complete their examination of the abdominal aorta, the educators adjusted the monitor and examination table to make the heights uncomfortable for use. The monitor was set well below the student’s eye level, and the examination table was set well below the student’s waist level; changes were documented on the template. The CAE Vimedix computer simulator was programmed to display a proximal abdominal aortic aneurysm (AAA) case. When the student reentered the laboratory to perform the aorta examination, the student was not explicitly informed of these changes. However, the educators did remind them of the need to freeze, measure the segments of the aorta, and record the images for later review. The DMS educators (n = 2) each used a paper copy of the aortic assessment template on clipboards for scoring, noting whether ergonomic adjustments were made to the workstation and any additional comments as the student completed a real-time examination of the aorta. Once the student completed the examination, a debrief session was held with the student that took no more than five minutes. The student was asked to present the case and reflect on the process of how each of the captured images and measurements was obtained. The educators used the four sections on the template to guide the discussion and included structured, individualized feedback on captured images/measurements and instructions on how to improve scanning performance. Students were also encouraged to live scan once again during the debrief session, after reviewing acquired images, to allow the student an opportunity to reflect on the feedback provided and attempt to acquire the appropriate image(s)/measurement(s). The augmented reality screen was also enabled to help students better visualize the pathology being scanned. In addition, ergonomic adjustments to the workstation were also discussed during the debrief session to provide further instruction on adjustments needed, if applicable. Students were also provided with an opportunity to ask questions that they still had. At the conclusion of the debrief session, each student was provided with a survey to complete before leaving to provide the educators with feedback on the learning process. The survey consisted of a demographic section, a list of statements for students to rate using a Likert scale, and open-ended questions at the end.
Results
All three students identified the presence of an AAA and accurately identified the location of the AAA that was presented as part of the abnormal aorta simulation case. In addition, all three students made ergonomic adjustments to the workstation; however, none of the participants raised the monitor to eye level. This was discussed with each student at the conclusion of the aorta examination, and proper monitor height (top of monitor near eye level) was demonstrated. The aorta examination scoring consisted of the following: 2D images of the Aorta (14 points), Proximal Aorta Measurements (7 points), Mid-Aorta Measurements (7 points), and Distal Aorta Measurements (7 points), for a total score of 35. Students’ total scores were very similar, ranging from 27 to 31. The simulation assessment tool was used to standardize performance evaluation during the student’s skill demonstration and standardize provision of feedback to the student during the debrief session.
Student 1
Student 1 immediately recognized the AAA and stated such. The participant also appeared to be comfortable moving between a longitudinal and transverse view of the aorta at each segment, with the aorta in view the entire time. All images and measurements were obtained at appropriate segments of the aorta, and each view was on axis. However, caliper placements for width measurements at the proximal and mid-aorta were inaccurate. Calipers were placed slightly diagonal on the transverse view of the aorta rather than directly across to obtain a true width measurement. This student completed the abdominal aortic sonogram in nine minutes. A debrief session was held with the student at the conclusion of scanning. The DMS educators reviewed the acquired images with student 1 and referred to the aorta assessment template to provide structured feedback on scanning performance. In reviewing proximal and mid-aorta measurements, the discussion centered on proper caliper placements. It was at this time that the student stated that he had initially intended to place the calipers straight across the transverse images of the proximal and mid-aorta, but he had noted there was not a hyperechoic border to place the caliper on one side of the aorta. Thus, he instead placed the calipers at a slight diagonal, where he stated a defined hyperechoic border was more clearly visualized (Figure 1).
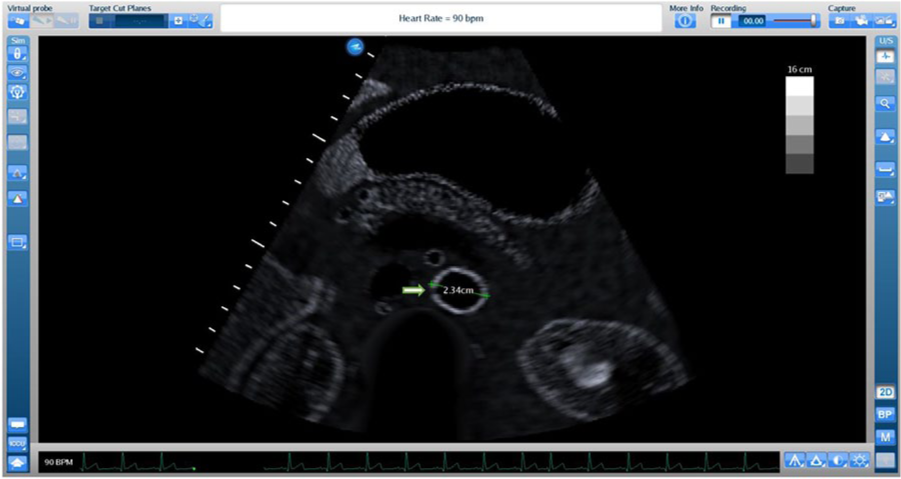
Arrow represents the location where students 1 and 2 identified the lack of a clear hyperechoic wall. Measurement was made diagonally to avoid placing caliper at that location. Used with permission from CAE Healthcare.
Student 2
Student 2 located the aorta immediately and appeared comfortable moving between a longitudinal and transverse view of the aorta at each segment, with the aorta in view the entire time. This student was also noted to self-critique his measurements throughout the examination and would take additional measurements to ensure his values were consistent. Student 2’s acquired images and measurements were all at appropriate segments of the aorta, and each view was on axis. However, this participant’s caliper placements for width measurements at the proximal, mid-, and distal levels were inaccurate. Similar to student 1, student 2 placed the calipers slightly diagonal on the transverse view of the aorta rather than directly across to obtain a true width measurement. This student completed the abdominal aortic sonogram in ten minutes. A debrief session was held with the student at the conclusion of scanning. The DMS educators reviewed the captured images with student 1 and referred to the aorta assessment template to provide structured feedback on scanning performance. As with student 1, when discussing proper caliper placement for transverse images, student 2 explained that not viewing a clear hyperechoic wall of the aorta made him question whether to place a caliper at that location or instead have a diagonal measurement by avoiding that location.
Student 3
Student 3 had difficulty locating the aorta and was initially evaluating the inferior vena cava (IVC). To prevent the student from continuing on the incorrect path, one of the educators stepped in and provided this student with assistance on how to distinguish between the IVC and aorta. Student 3 then identified and acquired appropriate images and measurements of the aneurysm at the proximal aorta, but AP measurements for the mid- and distal aorta were obtained at inappropriate locations. For example, the AP measurement for the mid-aorta was taken near the level of the inferior mesenteric artery (IMA) rather than near the level of the renal arteries. In addition, the student appeared to struggle to elongate the aorta while scanning and acquired a transverse image off axis at the mid-aorta, resulting in a larger mid-aorta measurement (2.85 cm) than obtained by the educators (2.3 cm) (Figure 2). This student completed the abdominal aortic sonogram in 14 minutes. A debrief session was held with the student at the conclusion of scanning. The DMS educators reviewed the acquired images with student 3 and referred to the aorta assessment template to provide structured feedback on scanning performance. Since the student had difficulty locating the aorta, the anatomy and psychomotor movement was reviewed using the split-screen feature of the CAE Vimedix to present both a sonography and augmented reality display. This was then followed by reviewing each of the four sections on the assessment template and providing further feedback on psychomotor control, as the student live scanned once again to acquire the necessary images and identify accurate measurement locations.
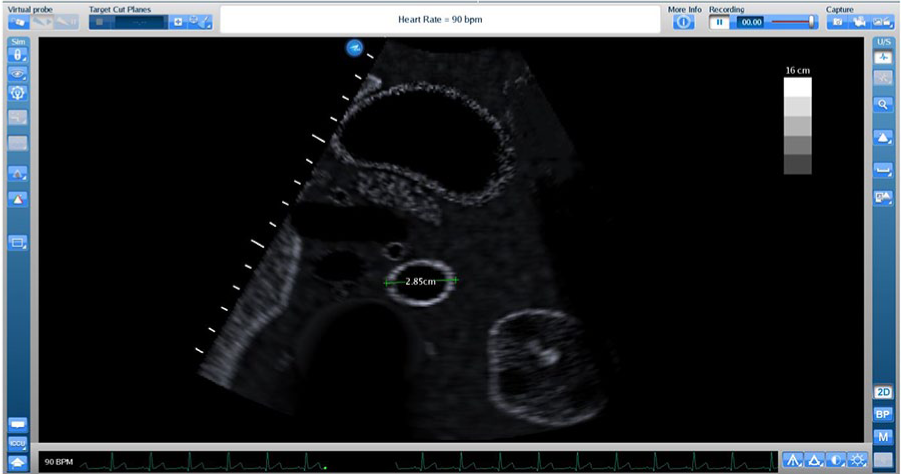
Transverse mid-aorta image taken off axis, resulting in larger measurement (2.85 cm) than obtained by the authors (2.3 cm). Used with permission from CAE Healthcare.
Survey
A survey of the students’ simulation experience provided quantitative and qualitative feedback to the authors about the experience, which could be used to refine the instructional process.
Each student was asked to rate a set of statements using a Likert scale and an option to elaborate on the reasoning behind the rating selected.
For statements 1 to 3, the Likert scale was as follows: 1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, and 5 = strongly agree.
I really enjoyed the debrief session afterwards. I also liked not being rushed, so I could take my time scanning and going back and forth between images. It is acceptable to make mistakes when real people are not involved as test subjects. It helps you correct yourself because you can simply try again.
I liked the fact that I got a “real clinical case” and was able to find a diagnosis. I would feel more comfortable scanning a real patient after completing this simulation. Loved the practice and debrief.
It was a lot of fun and low pressure. Great step to help learn scans without pressure of a patient being scanned. This provides a great tool for learning to scan.
The Likert scale for this statement was as follows: 1 = none, 2 = a little, 3 = somewhat, 4 = moderate, and 5 = a lot. Students’ ratings were 4, 5, and 5. Students elaborated on their ratings, stating the following: Great step to help me feel more comfortable scanning patients. I learned proper technique for transverse image measurements.
The students were also presented with open-ended questions at the end of the survey.
The texture of the mannequin’s skin was a little unrealistic. The hardware of the body was difficult. There is no change in the image with various pressures.
I loved the realistic image it produced and how we could go at our own pace. The virtual reality is also very useful to check to make sure we are picturing the image the correct way in our head. I liked that the interface was easy to use and less intimidating then a [ultrasound] machine. It was also nice to go at our own pace. The aneurysm images were good.
Absolutely! Like I said, it is low pressure when it is not an actual person who is dying in front of you. It’s also nice to get repetition and feedback on what I did well and what I can work on. Yes, great tool to transition and give students plenty of practice time to see how a scan should be done and how it should look before starting to scan a patient. Yes! They are a great steppingstone before live patients.
Discussion
Sonography is a highly operator-dependent imaging modality that requires deliberate practice to improve psychomotor skills. With a host of priorities to address, some medical schools may have difficulty integrating sonography into the curriculum to the extent needed for students to develop the requisite knowledge and psychomotor skills to effectively use sonography in practice (i.e., sufficient deliberate practice time and feedback to students). To this end, the authors piloted an instructional process that can provide students with the desired exposure to sonography in a relatively short period of time through didactic instruction, demonstrations, and debrief sessions. The process capitalized on the proximity of a DMS educational program but could be organized through collaboration with a hospital’s DMS department.
Following the instructional session, during the student skill demonstration, two of the three students identified the aorta immediately and appeared to be very comfortable moving between a longitudinal and transverse view of the aorta at each segment, with the aorta in view the entire time. The third student struggled in identifying the correct structure at the beginning of the examination, initially imaging the IVC, in addition to having difficulty elongating the aorta. This points to the importance of continued deliberate practice to improve psychomotor control and the need for direct guidance when a student is on the wrong path. Without the guidance of an educator, the student could have continued imaging the incorrect structure and may have left the session with a false sense of confidence in locating and effectively evaluating the aorta. With medical errors accounting for a major source of mortality and morbidity in developed countries, it is crucial to have an engaged instructor present during the student’s first demonstration of skills to provide immediate feedback to students if they are on the wrong path and ensure they can learn from this mistake.19,20
Furthermore, debrief sessions at the conclusion of student demonstration allow for students to receive overall feedback, reflect on performance, and voice questions they may still have regarding the scanning activity. 9 Feedback is regarded as a key feature in simulation-based education to increase self-confidence and level of participation, improve retention, and ensure that mistakes made during simulation-based training are not repeated in the clinical environment. 21 Multiple studies recognize the importance of debriefing sessions and have made it a point to include debrief sessions at the conclusion of their students’ assessments.13,14,22–24 In the current study, the authors aimed to set up a structured approach to the debrief sessions by using the assessment template to direct the conversation and note where improvements can be made, as well as provide students an opportunity to reflect on their performance. During a debrief/feedback session, proctors are encouraged to reinforce what students performed accurately and what can be improved. As noted by the students, it appears that they found value in the debrief session. One student explicitly stated that he appreciated learning what aspects he had done well on and what aspects need further development. Similarly, Young et al. 23 found that feedback to the participants helped them view their mistakes as learning opportunities, and Hughes et al. 24 discovered that students’ confidence was boosted when they received positive feedback on their performance. In addition to debrief sessions helping students reflect on their performance, it also allows examiners an opportunity to gain insight into the students’ thought process and better understand the rationale behind actions taken. This was the case during the debrief sessions with students 1 and 2, who explained their reasoning behind the incorrect measurements obtained on some or all of their transverse views of the aorta. This is a limitation of the CAE Vimedix case module that the authors had not initially identified when reviewing the fidelity of the case. If not for the debrief sessions, the students may not have voiced their uncertainty regarding appropriate caliper placements when a border is not clearly visualized, and proctors may not have identified the reasoning behind the inaccurate caliper placements. This issue and the inaccurate representation of the stomach on the sonogram decreases the simulation fidelity to a degree and should be further assessed.
The students each expressed a desire to increase their practice of scanning, and all agreed that this targeted instructional process contributed to their learning and improved their confidence in their scanning abilities. Although the students did not receive specific instructions on aneurysms and no aneurysm cases were demonstrated, they were able to build on the instructional demonstration and recognize the pathology. Students noted this unique added value of practicing on a computer-based simulator that allows for examination of a pathology case. A known limitation of scanning model patients includes limited or no opportunity to evaluate and practice scanning pathologic examinations. 25 This supports the use of CBS, which provides various pathology cases and ready access for individual or group practice. The students in this study also noted that this learning method was low pressure and that it was acceptable to make errors when real patients were not involved. This was similarly reported with nursing students who used a high-fidelity manikin-based simulation and reported that they valued the opportunity to practice on simulators and learn from mistakes in a safe (low-stakes) environment rather than in a clinical setting with patients. 26 In addition, in the current study, students were separated during the student demonstration and debrief phases to provide them each with a private environment to practice their skills on a pathology case and receive feedback. However, for large class sizes, these phases could be implemented in a small group of students. An added value to student demonstration and debrief phases provided in a small group setting would allow students to learn from one another’s demonstrations. As seen in this case series, both students 1 and 2 made similar errors in caliper placements on their transverse images and may have found value in observing classmates’ demonstrations and debriefs. However, it is important to ensure that students feel safe and comfortable demonstrating skills and having a debrief session in a group setting.23,24
This case series also incorporated a microergonomic lesson to educate students on adjusting equipment at their workstation to improve posture and decrease risk of work-related musculoskeletal injuries (WRMSIs). The prevalence of WRMSIs among diagnostic medical sonographers has been reported to be as high as 90%. 27 As the use of sonography increases among other medical specialties, prevention measures should be taken to decrease the risk of WRMSIs. While the authors noted that all three students made adjustments to both the bed and monitor heights before beginning the examination, the students needed further education on appropriate height of the monitor to ensure maximum comfort.
An important limitation to the current study is that the three participants in this feasibility study were all interested in sonography education and actively sought out opportunities to learn more about the use of ultrasound, beyond what is provided in their respective curricula. These results might differ for M1s with more limited ultrasound exposure.
Implications for Practice
The best practices that were proposed by Issenberg et al. 11 (curriculum integration, feedback, simulation fidelity, deliberate practice, and outcome measurement) were demonstrated in this discipline-based education research. Although the results from the students in the current study are unique to them, the case series demonstrates how educators or clinical preceptors could use computer-based simulation to engage medical students and support their educational outcomes. Direct assessments are very difficult with large classes of professional students, and therefore having options for informal demonstration of skills with focused feedback and debriefs can make the educational experience more robust. Instructors can also review and reflect on this kind of curricular set of exercises and determine when the desired outcomes are achieved. Given the difficulty of providing hands-on scanning sessions that allow students to evaluate and identify pathology, the integration of CBS can close that gap.
Footnotes
Acknowledgements
The authors thank CAE Healthcare for providing access to Vimedix simulators for this discipline-based education research. The authors also thank John Mickley, BS, and Isaiah Bloom, our research technician, for their assistance in this project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was generously supported by funding from Inteleos, Inc.