
Abstract
Purpose:
Evaluate obstetrics and gynecology (OB/Gyn) residents’ current obstetric sonography knowledge, confidence, and psychomotor skills to provide clinical preceptors with a greater understanding of how to approach teaching sonography to residents.
Methods:
Ten OB/Gyn residents were assessed on their sonographic performance by measuring psychomotor skills and evaluating diagnostic accuracy of images. At the conclusion of the assessment, residents received feedback and completed a survey to establish their current confidence level in performing and interpreting sonograms.
Results:
Motion analysis revealed excessive transducer movements made by the residents when acquiring images, particularly in terms of angular movement. The median score on the assessment template was 33 out of 66 points (interquartile range, 26.75–42.5), where residents had difficulty acquiring all required criteria for first-trimester dating and biometry views/measurements, determining fetal situs, and identifying landmarks to ensure intended anatomy is visualized.
Conclusions:
Absence of formalized sonography training creates a need for clinical preceptors to teach basic anatomy/landmarks, transducer movements, and criteria for dating and biometry views/measurements. This poses a challenge for preceptors at high-volume sites; thus, high-fidelity simulation could be part of a solution. Simulation can provide residents with the opportunity to develop basic sonography skills outside of clinical, then refine and build upon those skills with preceptors.
Continued advancement of sonographic imaging, portability of equipment, absence of ionizing radiation, and advantages to real-time evaluation of anatomy has resulted in the significant increase in the utilization of this imaging modality among various health care professionals. The annual global utilization of imaging for 2000 and 2011 revealed a greater than 10-fold increase in the number of sonograms. 1 This would be compared to the annual global use of magnetic resonance imaging (MRI), computed tomography (CT), and nuclear medicine, which approximately doubled during this same time period. 1 As the use of sonography continues to expand clinically, it is also being integrated across various medical specialties. This would portend that medical schools, residencies, and fellowship programs across the United States will need to invest in sonography training as part of their respective curricula. 2 Currently, several radiology and obstetrics and gynecology (OB/Gyn) residency programs incorporate joint efforts with diagnostic sonography laboratories, where these learners can be preceptored by registered diagnostic medical sonographers (RDMS). While this provides residents and fellows with an opportunity to learn directly from sonographers, a lack of standardized sonographic education, across residents’ subspecialties, poses a challenge to those who serve as clinical preceptors.
As residents rotate through sonography laboratories at different times during their education, clinical instructors may be unaware of the level of knowledge and hands-on experience that each resident has accomplished. In a sample of OB/Gyn residency programs, a survey found that 30.2% of residents received no sonography didactic training, and for those who did, 40% of lectures were offered no more than once a year. 3 Nevertheless, sonography plays a significant role in OB/Gyn, with 97.8% of Ob/Gyn residency directors and 93.9% of residents reporting that sonography is performed daily or weekly. 3 Although OB/Gyn residents are required to complete a minimum of 50 OB and 50 Gyn sonograms by the end of their residency training, per the Accreditation Council for Graduate Medical Education (ACGME), little guidance is given on the quality of the examinations.4,5 Instead, quality of the examination becomes the purview of clinical preceptors to ensure that residents, of varied expertise, obtain accurate fetal images and measurements.
This research evaluated a cohort of OB/Gyn residents, from an accredited residency program, and assessed their sonographic knowledge, level of confidence, and psychomotor skills, using a high-fidelity computer-based sonography simulator (CBSS). This educational research was designed to inform clinical preceptors of the degree of residents’ clinical mastery, regardless of their prior sonographic experience.
Materials and Methods
Participants
Incoming postgraduate year 2 (PGY2) residents who successfully completed their first year of residency were invited to participate in this institutional review board–approved study. A total of 10 participants consented to the study. As part of their first year of residency, residents had been introduced to sonography through a limited-skills laboratory during orientation. This skills laboratory provided a brief overview of knobology, fetal presentation, and images of biometry views. In addition, throughout their first year, they rotated through multiple clinical sites at different times and with varying levels of exposure to sonography. Their clinic rotation provided opportunities for residents to observe and scan with a RDMS. Other clinical sites provided “hands-on” experience with sonography, including triage area, antepartum/high-risk obstetrics unit, and labor and delivery department. During these rotations, the residents were able to image patients, preceptored by faculty or residents with more experience. However, without formalized sonography education, the residents relied heavily on a RDMS, faculty, and peers in those clinical sites for personal training.
Equipment
A CAE Vimedix OB/Gyn sonography simulator (CAE Healthcare, Quebec, Canada) was used for this research. This high-fidelity CBSS included the following equipment: computer processing unit (CPU), monitor, curvilinear transducer, and a female manikin. The system allowed for measurements, saving images/cine clips, limited optimization (e.g., depth, gain, contrast), split screen of a sonography and 3D augmented reality display, selection of over 50 pathology cases, and a unique feature that captures motion data, called the Target Cut Plane (TCP). The TCP function allows instructors to archive images and corresponding transducer placement for an ideal image. If desired, instructors can reveal the reference images, during a training session, to provide learners with guidance on appropriate transducer manipulation and how to achieve the required fetal view. Once TCP(s) are activated, quantifiable kinematic metrics are recorded. Kinematic metrics include the following:
Time. Total time, in seconds, from the start of the scan until an image is acquired
Distance traveled. The sum of the total distance, in centimeters, traveled with the transducer from the start of the scan until an image is acquired
Peak movements. Number of accelerations made from rest, determined by the transducer transitioning from a speed of 0.05 cm/s to a speed greater than 0.05 cm/s, made from the start of the scan until an image is acquired
Angular movement. The sum of angular movements (degrees) made with the transducer from the start of the scan until an image is acquired
Assessment of Residents
Each participant was assessed during a one-on-one 60-minute session with a proctor (S.H.M.). The assessment of participants’ sonography skills and knowledge included fetal presentation, fetal situs, fetal heart rate (FHR), biometry views and measurements, documentation of bilateral fetal extremities, and crown-rump length (CRL) images and measurements. The assessment items were based, in part, on a consensus report that provides a standardized sonographic curriculum and a list of competency assessments for PGY1–4 OB/Gyn residents. 4 Before finalizing the list of assessment items for this study, the list was reviewed by the OB/Gyn residency director and a department faculty member. The assessment list for this study was also constrained by the examinations available on the high-fidelity CBSS used to assess the participants. Sonographic performance was evaluated via a combination of kinematic metrics obtained with motion analysis technology to measure psychomotor skills and an assessment form to evaluate diagnostic accuracy. At the conclusion of the evaluation, a brief debrief session was held to provide each participant with feedback on his or her completed sonographic study. The residents were also provided with an opportunity to practice obtaining a few of the views and measurements. Last, a survey was provided at the conclusion of the assessment and debrief to establish the resident’s current level of confidence in performing and interpreting basic obstetric sonograms.
Acquisition of Target Cut Planes
A normal 20-week case, with fetus in a breech presentation, was selected by a RDMS, with OB/Gyn sonography credentialing. The sonographer created a set of reference images, within the TCP package, for the following fetal images: (1) head circumference (HC)/biparietal diameter (BPD), (2) abdominal circumference (AC), (3) right lower extremity (femur, tibia and/or fibula, foot), (4) left lower extremity (femur, tibia and/or fibula, foot), (5) right upper extremity (humerus, distal upper extremity), and (6) left upper extremity (humerus, distal upper extremity).
For documentation of the distal lower and upper extremity long bones, it was determined that residents would be required to capture an image of at least one of the fetal long bones in a longitudinal plane (i.e., tibia and/or fibula for distal lower extremity). In addition, the umbilicus of the manikin was established as the starting point for all TCP metrics where the transducer was placed vertically and on a transverse plane, relative to the manikin. Prior to working with participants, the data obtained via TCP metrics were validated by placing the transducer in the same locations along the manikin and confirming the consistency and reproducibility of the metrics. Furthermore, two expert sonographers with 5 and 10 years of high-risk OB clinical experience, respectively, were invited to assist the research team by setting expert-level metrics. These sonographers were deliberately chosen with limited or no previous hands-on exposure to high-fidelity CBSS. They scanned through the newly created TCP package, and extracted metrics were reviewed for face validity and saved for comparative reference metrics.
Assessment Form
In addition to capturing kinematic metrics using TCPs for images listed above, the proctor created an assessment form to record the participants’ responses and accuracy of the captured images and measurements, compared to the required examination components. The form contained an assessment for 20-week and 12-week fetal sonograms (see Appendix A or supplemental material). The 20-week fetal assessment included evaluation of presentation and situs, FHR, biometry views/measurements, and documentation of bilateral extremities (long bones and bilateral feet). The requirements of biometry views and measurements were based, in part, on biometry competency assessments created by Abuhamad et al. 4 The 12-week assessment included evaluation of three fetal crown-rump length images and measurements.
Statistical Analysis
The data gathered were entered into Microsoft Excel (Microsoft, Redmond, WA), and this program was used to generate descriptive statistics. The data demonstrated nonnormal distribution; therefore, median and interquartile ratios were generated instead of means and standard deviations.
Results
Assessment Form Scores
The median score on the assessment template was 33 out of 66 points (interquartile range [IQR], 26.75–42.5), with the following median values per category: fetal presentation and situs (3.5/7), FHR (3/3), biometry views and measurements (15/25), documentation of bilateral extremities (7.5/22), and first-trimester dating scan (3/9). Please review the supplemental material provided for a detailed breakdown of assessment scores.
At the start of the assessment, two fetal presentations were presented to the residents: breech and transverse lie. All 10 residents had correctly identified the breech presentation of the fetus, and nine of the residents correctly identified the transverse presentation of the fetus, with one resident stating the latter was a breech presentation. In addition, six residents were able to verbally state the correct approach to confirming normal fetal situs (i.e., stomach located on fetal left and cardiac axis pointing to fetal left). However, when asked to identify the left side of the fetus in the breech and transverse lie cases, only three were able to correctly respond.
Furthermore, when acquiring biometry views and measurements, there were key anatomy structures that most residents did not capture in their HC/BPD image (Table 1 and Figure 1). Although six of the 10 residents obtained accurate HC measurements, multiple errors were noted for the BPD measurement. Of the 10 residents, eight did not place the caliper in the near field of the image at the outer edge of the cranium (instead placing caliper at the skin line), five did not make the measurement at the widest diameter of the cranium, and seven did not make their measurement perpendicular to the cerebral falx. Nevertheless, higher median scores were noted for the AC image and measurement, 5.5/7 and 1/1, respectively. The one criterion that most residents (6/10) struggled to acquire for this view was a circular abdomen with only one pair of ribs visualized. Last, the median scores of the femur length image and measurement were 1.5/3 and 0.5/1, respectively, with three residents not selecting the femur in the near field of the image for measurement, six residents not setting the femur perpendicular to the ultrasound beam, and four residents not fully elongating the femur bone. Two residents were also noted acquiring an image and measurement of the left humerus (located in the far field of the image) for their femur length. One of those two residents noticed their error and reimaged the femur length. Yet, the replacement image was of the left femur, and the bone was not perpendicular to the ultrasound beam.
Frequency of Criteria that Post Graduate Year 2 Obstetrics and Gynecology Residents (n = 10) Either Did (Yes) or Did Not (No) Meet for Each Diagnostic Quality Assessment Criterion on Head Circumference/Biparietal Diameter Sonographic Image.
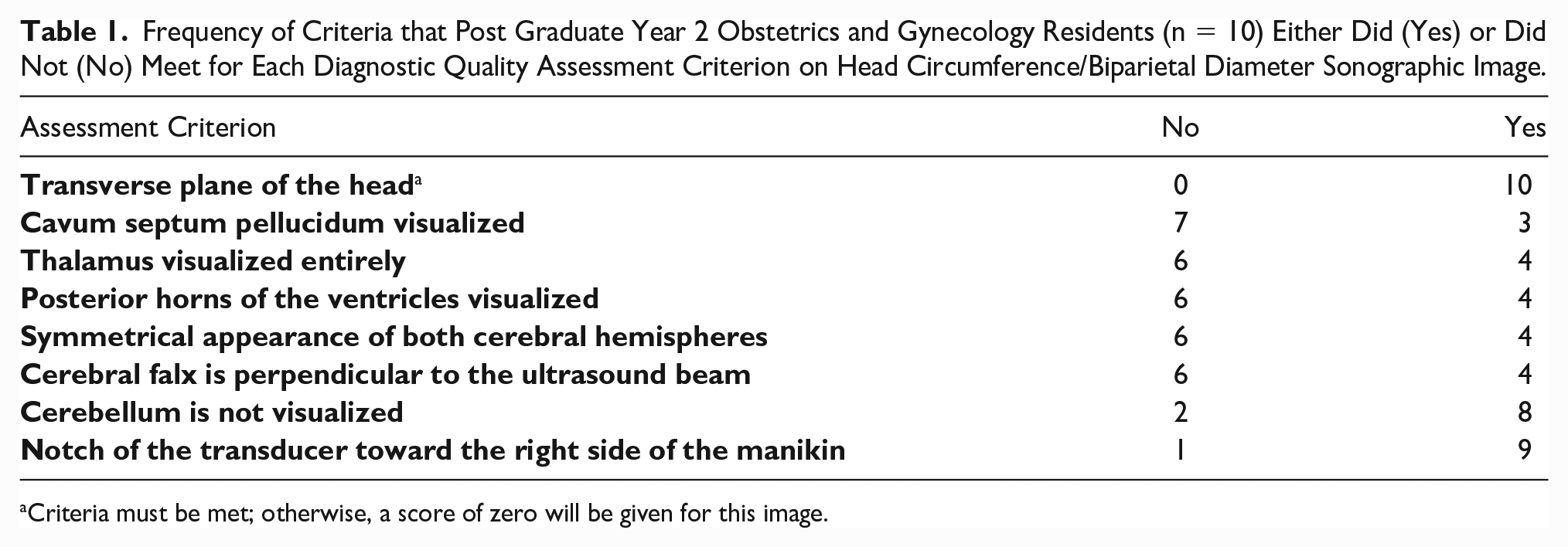
Criteria must be met; otherwise, a score of zero will be given for this image.
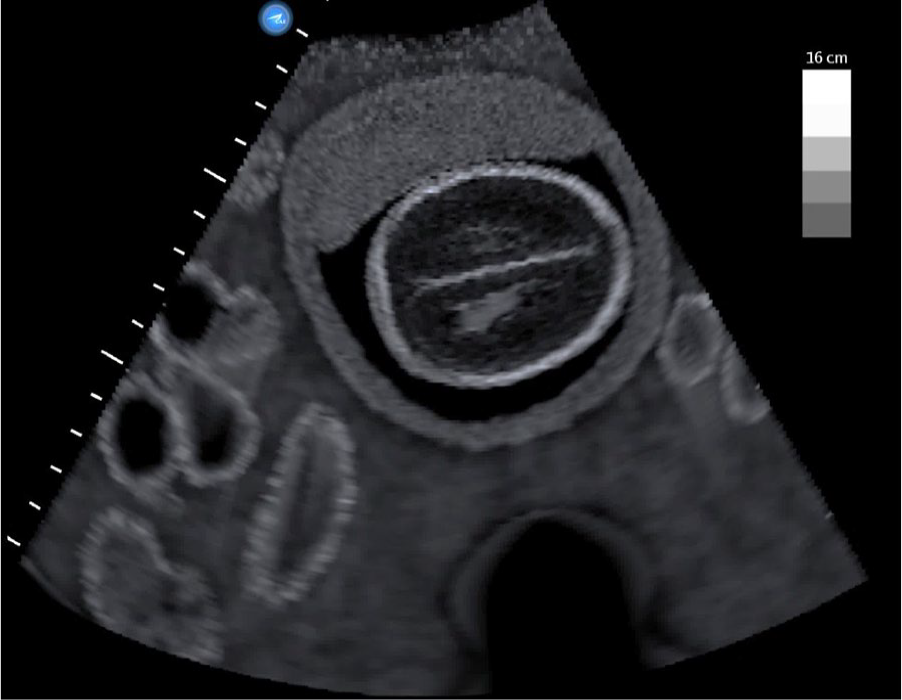
A fetal head sonogram produced by a postgraduate year 2 resident for head circumference/biparietal diameter measurements. The image was taken superior to the appropriate level for fetal biometry head measurements. The following anatomy are not visualized: cavum septum pellucidum, thalamus, and posterior horn of the right ventricle. Additionally, the following criteria were not met: Cerebral falx is perpendicular to the ultrasound beam and symmetrical appearance of both cerebral hemispheres. Used with permission from CAE Healthcare Inc.
During documentation of bilateral lower and upper extremities, the assessment form was used by S.H.M. to evaluate the accuracy of the images captured. Figure 2 provides descriptive data on the number of residents who did and did not meet the criteria set for documentation of bilateral lower and upper extremities. Two residents had difficulty locating and following the right lower extremity (RLE) and left lower extremity (LLE). For documentation of the right lower extremity, one resident first acquired an image of the left femur and then switched to the right side of the fetus for documentation of the distal lower extremity and foot. This error was again made for documentation of the left lower extremity, resulting in the same bones being documented. In addition, the same resident who documented the humerus length as the femur length for a biometry measurement once again misidentified the humeri for the femur bones. As this resident began to document the RLE and then the LLE, the resident initially documented one of the humeri as the femur image and then proceeded to move to the lower extremity of the corresponding side to acquire the distal lower extremity images. Nonetheless, most residents were able to document the following bones in their entirety: bilateral femurs, unilateral tibia and/or fibula, and bilateral humeri.
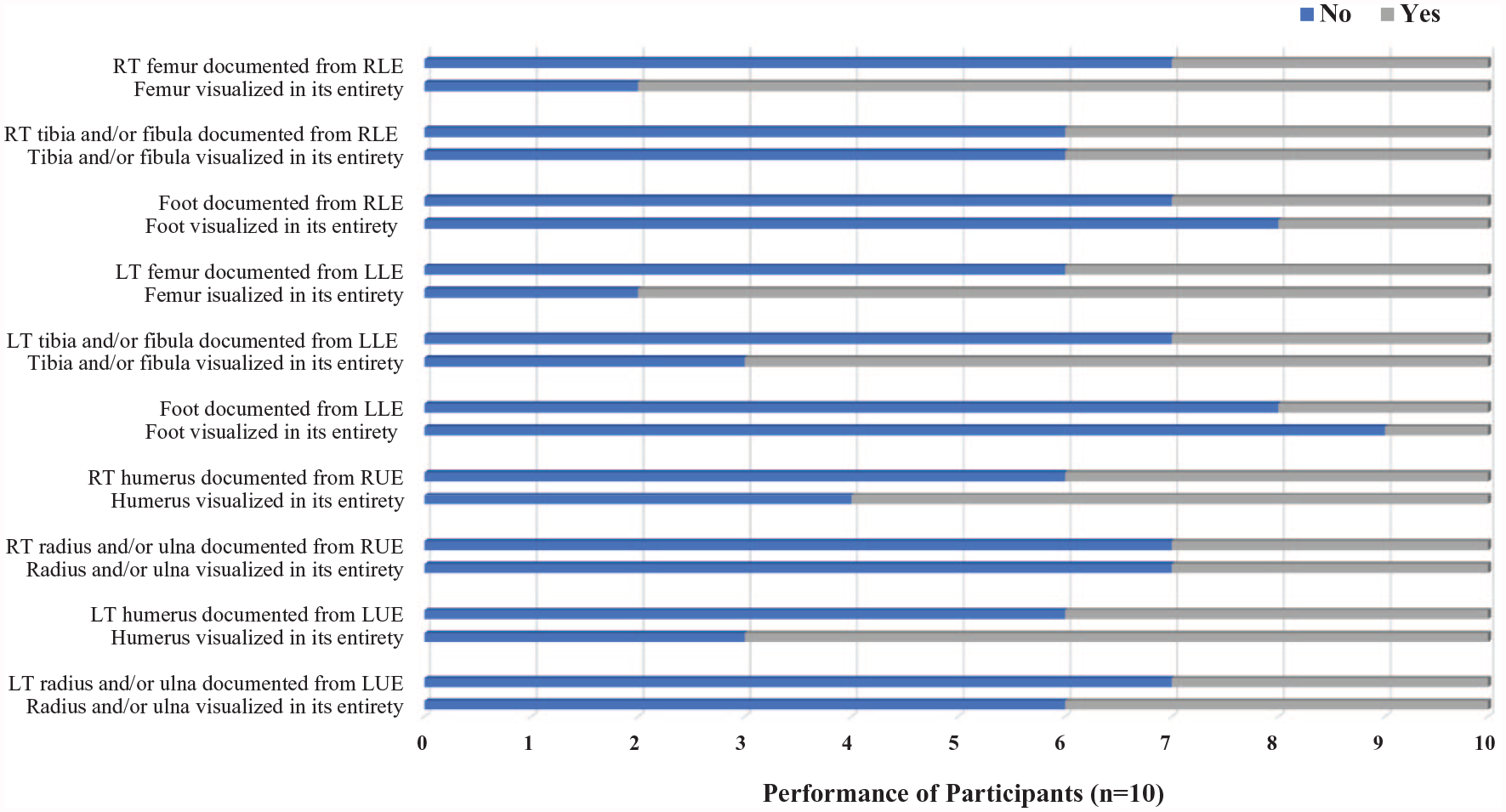
Postgraduate year 2 residents’ documentation of bilateral fetal lower and upper extremities. LLE, left lower extremity; LUE, left upper extremity; RLE, right lower extremity; RUE, right upper extremity.
After concluding documentation of extremities, a first-trimester dating scan was performed on a 12-week fetus. All 10 residents had difficulty acquiring midline sagittal images of the fetus for their CRL measurements, and calipers were improperly placed on the fetus (Figure 3). Only two residents acquired an image of a midline sagittal view of the fetus, yet in both cases, the calipers were not placed on the longest axis of the fetus. Furthermore, while seven of the 10 residents acquired three CRL measurements, the remaining three residents acquired only two CRL measurements.
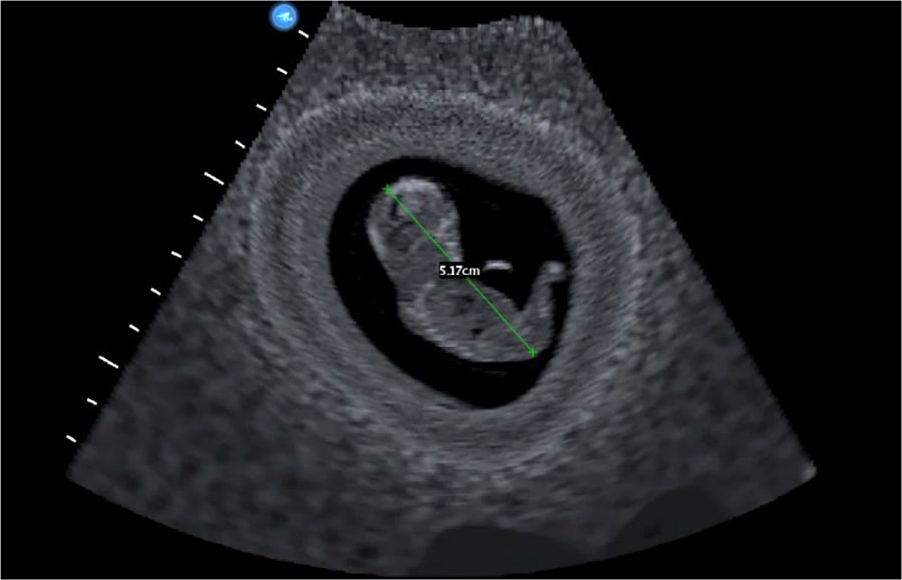
A crown-rump length image and measurement produced by a postgraduate year 2 resident. The image does not demonstrate a mid-sagittal view of the fetus and caliper placement is not placed at the rump of the fetus. Used with permission from CAE Healthcare Inc.
Target Cut Plane Metrics
Through TCP metrics, researchers were able to document the total time until image(s) were captured, in addition to total distance traveled (cm), angular movement (degrees), and number of peak movements made from rest with the transducer during that timeframe (Table 2). For each of the TCP metrics, there was a wide range between the minimum and maximum values acquired, particularly across the total angular movements made with the transducer. The largest difference between residents’ and experts’ TCP metrics was also noted for total angular movement. While experts made deliberate, small movements to acquire the images needed, most residents were making larger movements in both distance and angular movement to achieve an image they perceived as ideal (Figure 4 and Figure 5). This was predominately seen when residents were acquiring longitudinal views of the long bones. After locating the long bone, many residents struggled to lengthen the bone and were making large movements to obtain the desired image. Furthermore, they consistently took longer to acquire their images and tended to take more stops and accelerations compared to the experts.
Descriptive Data Generated by the CAE Vimedix for the Cohort of Postgraduate Year 2 Residents Assessed.
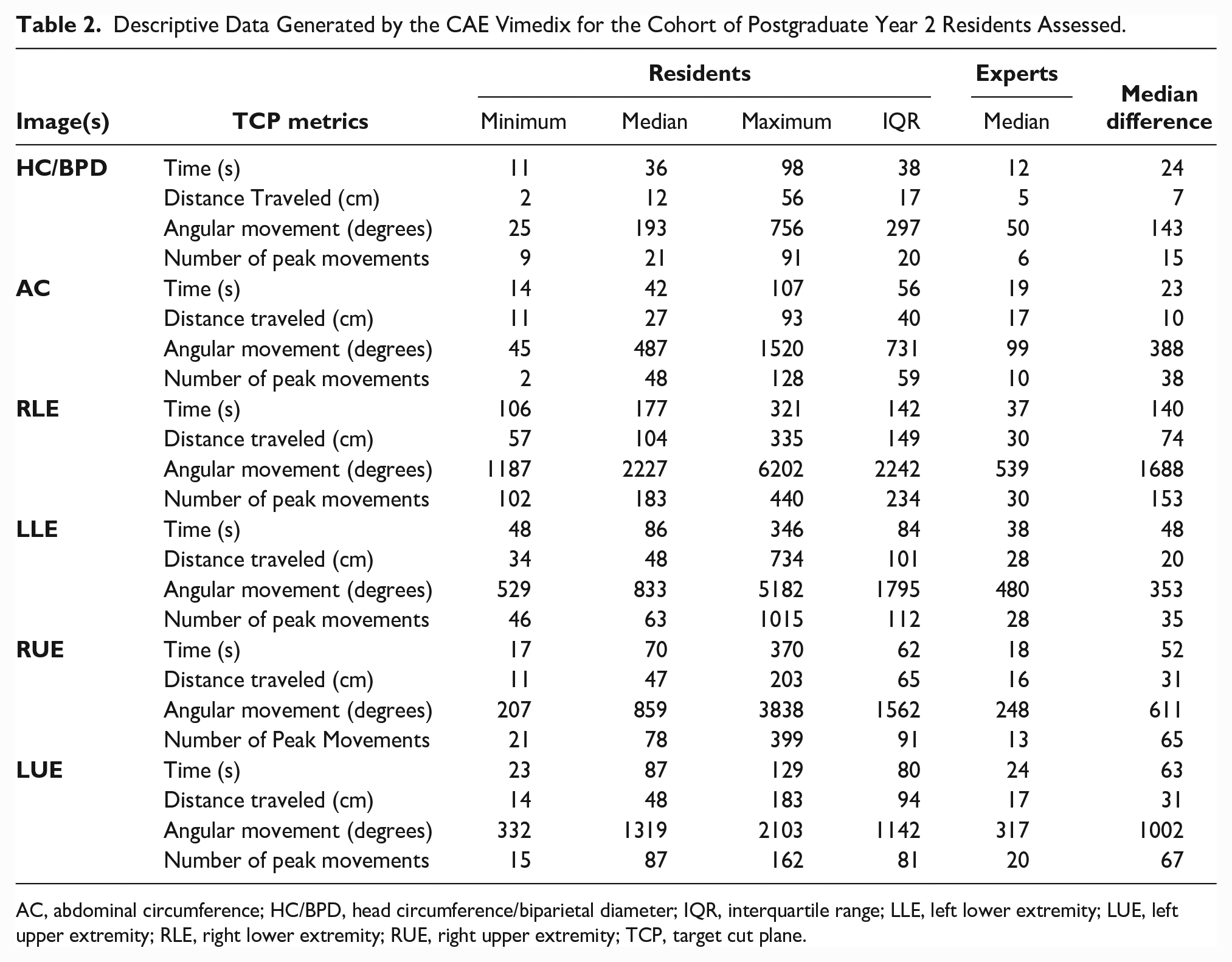
AC, abdominal circumference; HC/BPD, head circumference/biparietal diameter; IQR, interquartile range; LLE, left lower extremity; LUE, left upper extremity; RLE, right lower extremity; RUE, right upper extremity; TCP, target cut plane.
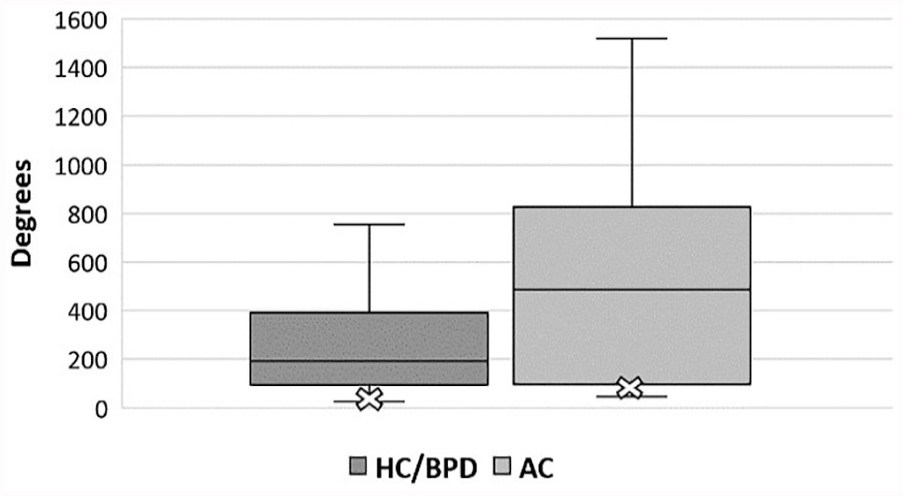
Head and abdomen. Postgraduate year 2 residents’ total angular movements obtained via target cut plane metrics for head circumference/biparietal diameter (HC/BPD) and abdominal circumference (AC) images. X marks the median value of experts’ total angular movements for HC/BPD and AC images.
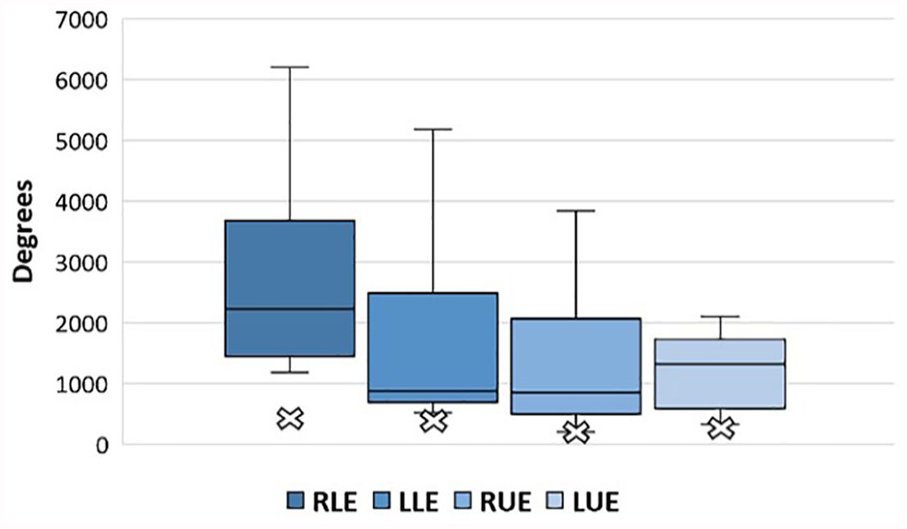
Extremities. Postgraduate year 2 residents’ total angular movements obtained via target cut plane metrics for bilateral upper and lower extremities. X marks the median value of experts’ total angular movements for bilateral upper and lower extremities. LLE, left lower extremity; LUE, left upper extremity; RLE, right lower extremity; RUE, right upper extremity.
Survey
Most PGY2 residents agreed that they are confident in identifying/locating fetal anatomy, performing a first-trimester dating scan and fetal biometry views/measurements (Table 3). However, it was noted that a few residents had either never performed a first-trimester scan or rarely performed them and would not feel comfortable performing a dating scan without assistance. Furthermore, most residents did not feel that they have had sufficient hands-on scanning opportunities to strengthen their scanning skills (survey question 6: four residents, disagree and three residents, neutral). Similarly, residents noted that they did not feel that they had the opportunity to practice obstetric scanning at their own pace, with one resident elaborating on a neutral rating, stating, “We are extremely busy, so I often rush through scanning patients.” On the other hand, other residents stated they feel that they have had the opportunity to practice at their own pace and learn through trial and error, with one resident stating, “Regular scanning opportunities. Lots of [high patient] volume end up [allowing me to] be able to [scan] enough [patients] at different paces.” Additional comments provided to the open-ended questions regarding overall experience with the simulator are included in Table 4. All PGY2 residents agreed that the simulator was a useful tool and believe that they would benefit from continued practice. The significance of feedback was also emphasized with a few residents stating that while simulation alone may be beneficial, simulation coupled with feedback would be ideal for their continued learning.
Median Value and Range of Values in Response to the Poststudy Survey Generated by the Cohort of Postgraduate Year 2 Residents (n = 10). a
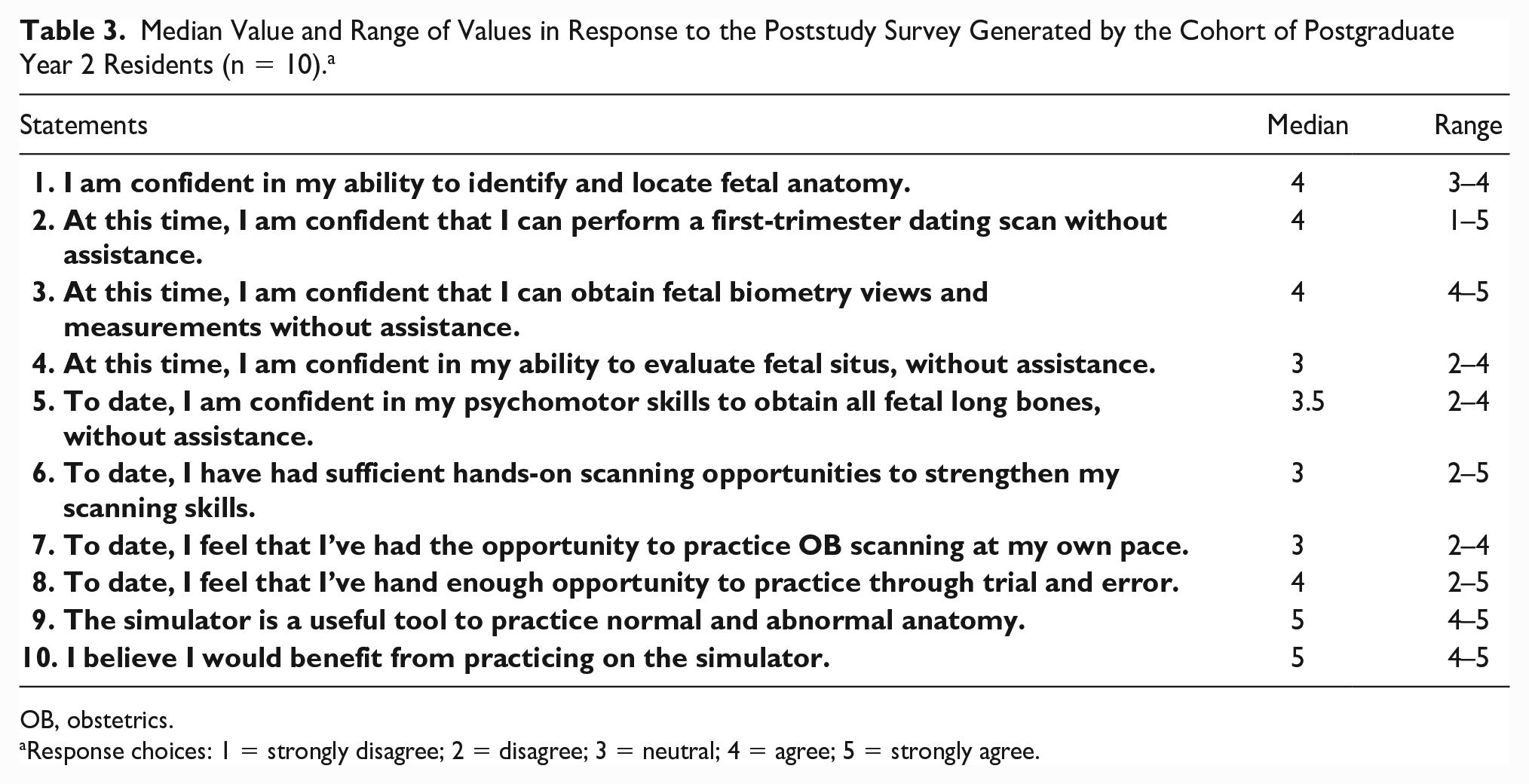
OB, obstetrics.
Response choices: 1 = strongly disagree; 2 = disagree; 3 = neutral; 4 = agree; 5 = strongly agree.
Open-Ended Survey Questions and Corresponding Responses from Postgraduate Year 2 Residents Who were Assessed with the CAE Vimedix.
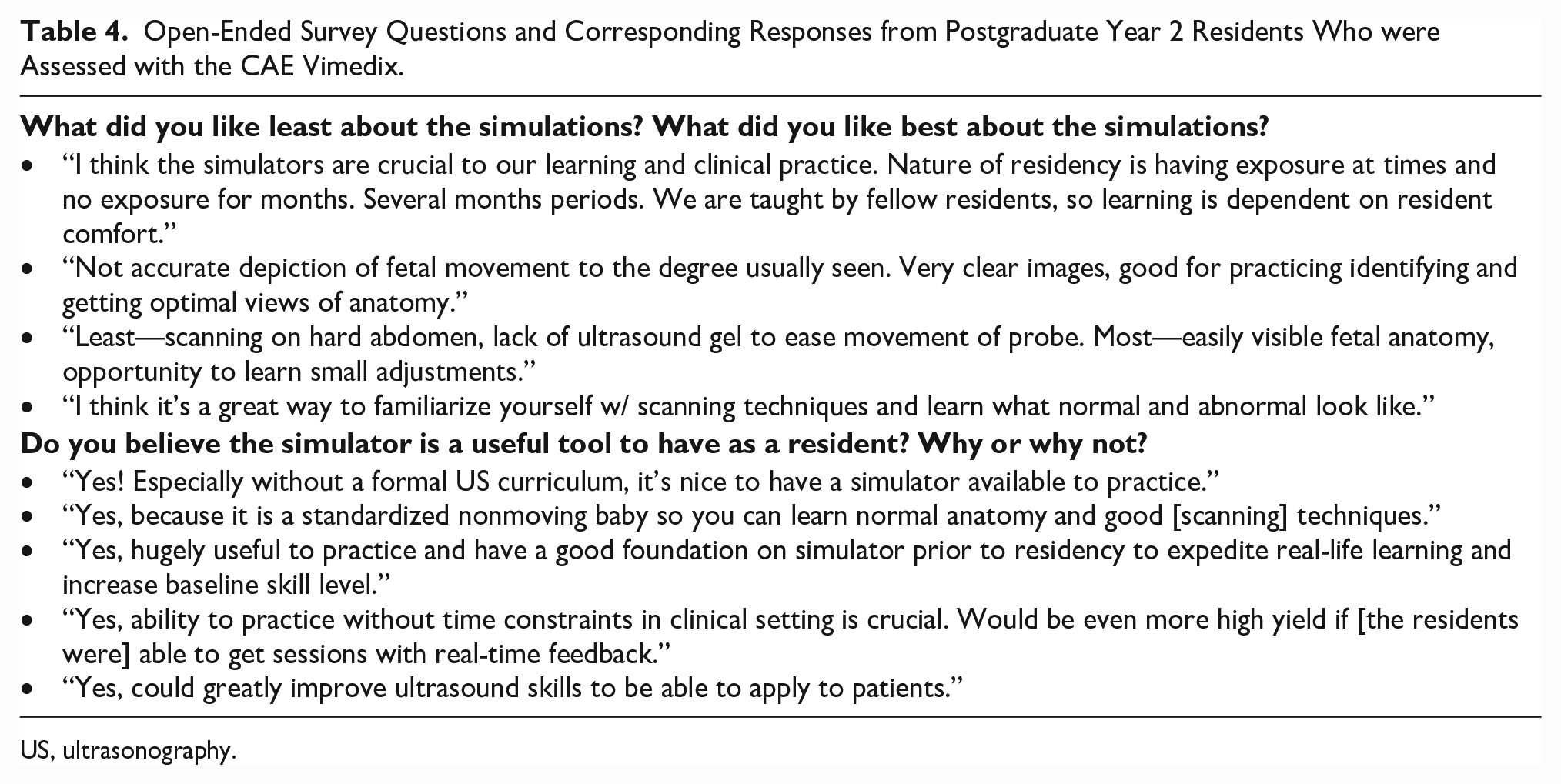
US, ultrasonography.
Discussion
Sonography is a highly operator-dependent imaging modality and, as such, requires hands-on exposure to develop the necessary hand-eye coordination skills. Many residency programs do not incorporate longitudinal formalized sonography training into their curriculum, and as such, residents gain most of their knowledge and psychomotor skills by scanning patients during clinical rotations, preceptored by sonographers, faculty, or peers. The absence of formalized and standardized sonography education can result in a discrepancy in the level of knowledge and psychomotor skills among residents. This fact makes it difficult for clinical preceptors to approach sonography training during clinical rotations in which they are expected to train residents. In this study, researchers found that although participants rotated through the same clinical sites during their first year of residency, there were differences in their level of exposure, knowledge, and confidence in acquiring obstetric sonograms.
During the assessment, most residents were unable to capture all the required components of biometry views, and some measurements were inaccurate due to misplaced calipers. With the absence of formalized sonography training, there is a need for clinical preceptors to begin each training session by teaching and/or reviewing fetal anatomy and the components that must be visualized, and not visualized, for each biometry view. In addition, a basic understanding of presentational lie and situs should be confirmed. While most residents were able to correctly identify the fetal anatomy presenting at the cervix, there was difficulty in visualizing how the fetus was lying to determine which side of the fetus was left, distinguishing between upper and lower extremities and unknowingly switching between right and left extremities. Specific landmarks for identifying the upper and lower extremities (i.e., hip bone for femurs) should be discussed to prevent errors such as humerus measurements in place of femur length measurements. Moreover, a basic understanding of the required components of a CRL should also be emphasized as CRL measurements taken between 8 and 14 weeks are the most reliable form of establishing gestational age. 6
Furthermore, kinematic metrics captured via TCPs provided enlightening data regarding residents’ psychomotor skills. It revealed the degree of excessive movement of the transducer made by the residents as they acquired what they perceived as the ideal image. A study by Montealegre-Gallegos et al. 7 applied motion analysis via TCP on cardiology fellows performing transthoracic echocardiography (TEE) at the start and end of a TEE training program. They found similar types of excessive movements were made at the start of the training program. However, by the end of the program, a statistically significant reduction in the total time, path length, and probe accelerations was noted. 7 During assessment and feedback of participants in the current study, the researchers found that despite completing the first year of residency, not all residents had a foundational understanding of basic transducer movements and their corresponding effects on the sonographic image. For example, rotating the transducer will result in lengthening the view of a long bone, rocking the probe can help in setting the long bone and cerebral falx perpendicular to the ultrasound beam, and fanning the transducer can help relocate a long bone when the bone is no longer in view during a rotation. Through repetition and teaching each resident basic transducer movements, clinical preceptors can help improve residents’ psychomotor skills.
One of the essential components to learning is receiving feedback to help facilitate reflection on performance and learn what was done well, as well as what aspects need further development. Many studies have revealed the benefits of feedback and debrief for effective and efficient learning.8–10 Thus, this study incorporated a brief debrief session at the conclusion of the assessment, which involved an overview of residents’ assessment findings and providing feedback on basic transducer manipulation to improve psychomotor performance. The survey revealed that residents also recognized the significance of feedback on their clinical education. As such, it is recommended that clinical preceptors set time aside to provide trainees with direct and personalized feedback that includes encouragement on what was done well and what aspects need to be improved. Nevertheless, feedback should also be followed with continued deliberate practice to apply the new information and refine existing skills.8,11 This learning model can be described using the cycle of practice and feedback that consists of three components: observed performance, allowing for targeted feedback, which then guides further practice, at which point the cycle repeats. 11 Due to sonography requiring a high level of psychomotor control, the need for deliberate practice is essential to develop the necessary muscle memory and fine motor control. As such, although residents received targeted feedback at the conclusion of the study, continued deliberate practice is needed to develop the required skills. This sentiment was echoed by some of the residents who recognized that further practice is needed before feeling confident in their skill level, such as documentation of fetal bones, with one resident noting that they are most familiar with acquiring the femur bone but would be able to acquire the remaining fetal extremities with practice and time.
The authors acknowledge that with the increase in patient volumes, clinical preceptors may have limited time to review basic anatomy and psychomotor controls with each resident. As such, this study would suggest that residency programs should consider the value of more formalized sonography training utilizing a high-fidelity CBSS, coordinated instruction, and limited debriefing. Currently, less than 20% of residency programs reported having experience with sonography training using simulation. 12 Limited research exists on the impact of a high-fidelity CBSS for training OB/Gyn residents, however evidence suggests that some form of simulation has a positive contribution for students as they strive to enhance their sonographic knowledge and performance.13–15 Thus, there is great value in integrating simulation into residents’ training, coupled with the expertise of clinical preceptors, which can help residents refine and gain advanced sonography skills.
There were limitations to this study. This study had a small sample size, mainly due to the cohort of residents per class and participants all came from the same residency program. As such, findings of this study may not be representative of other residents and residency programs. Furthermore, a limitation of using a high-fidelity CBSS is the static display of the fetus with only dynamic movement of the fetal heart. Nevertheless, this did allow for psychomotor skills that are comparable due to a standardized manikin and fetal position. Next steps for this research include assessment of residents who do receive sonography training using a high-fidelity CBSS to determine if a significant difference is identified between the two cohorts. Further research should also be conducted to evaluate whether skills learned using a high-fidelity CBSS are transferable to the clinical setting.
Conclusion
With the absence of standardized and formalized sonography training in OB/Gyn residency programs, many residents gain their knowledge and psychomotor skills in various clinical settings, with guidance from clinical preceptors. As such, the responsibility of sonography training falls into the hands of clinical preceptors, who must oversee the training of residents with varying levels of sonography education. This study identified a need for clinical preceptors to begin each initial training session by reviewing basic anatomy/landmarks, psychomotor skills, and criteria for dating and biometry views/measurements. Nevertheless, the authors recognize that teaching obstetric sonography, supplying clinical assessment, and providing feedback require added time for a busy clinical preceptor. A potential solution could include the utilization of high-fidelity CBSS to provide a safe (low-pressure), readily accessible, and controlled environment for resident education. The use of high-fidelity CBSS can aid in providing a uniform educational foundation for residents and potentially facilitate translation of those skills to the clinical setting.
Supplemental Material
JDMS-19-12-121-OR.R1_AppendixA – Supplemental material for Assessment of Obstetrics and Gynecology Residents’ Knowledge of Basic Obstetric Sonography and Psychomotor Evaluation With Motion Analysis Using a Computer-Based Simulator
Supplemental material, JDMS-19-12-121-OR.R1_AppendixA for Assessment of Obstetrics and Gynecology Residents’ Knowledge of Basic Obstetric Sonography and Psychomotor Evaluation With Motion Analysis Using a Computer-Based Simulator by Sundus H. Mohammad, Carolyn M. Sommerich, Angela N. Butwin and Kevin D. Evans in Journal of Diagnostic Medical Sonography
Footnotes
Acknowledgements
We thank CAE Healthcare Inc. for providing access to Vimedix simulators and Pamela Foy, MS, RDMS, FSDMS, and Phillip Samuels, MD, for their contribution to this research project. The primary author would also like to thank the SDMS Foundation and Inteleos for their financial support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support was received from SDMS Foundation Research Grant, and Inteleos.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.