
Abstract
Objectives:
Worldwide medical schools that provide sonography training appear to be very heterogeneous in their offerings. A medical school has developed a training program with limited resources, which used a peer teaching method, to provide sonography training. The implemented courses consist of a voluntary laboratory practical and a required didactic seminar.
Methods:
To analyze this concept, the effects on knowledge, skills, and attitudes were examined by using surveys, multiple-choice tests, and practical tests.
Results:
The teaching concept demonstrated a positive effect on theoretical knowledge, practical skills, and attitudes. Nevertheless, some practical skills such as conducting gallbladder sonography deteriorated over the time of the study.
Discussion:
The peer-teaching approach with well-trained students as instructors and tutorials in smaller groups appeared to be a key element for success. This cohort study underlines the need to provide both theoretical and practical mandatory training.
Conclusion:
Peer teaching may be a cost-effective way to teach sonography skills to medical students during their training.
Keywords
The improvement of medical school education is a widely discussed topic across the world.1–3 Many different teaching techniques have been implemented in several countries, such as flipped classrooms and e-learning, which have been evaluated to provide theoretical education as well as trusted professional activities for students.4,5 Also in the field of sonography education, training programs are being created and optimized in various countries.6,7 Nevertheless, educational resources may be limited, and there exists a need to investigate ways to more effectively use these resources.1,8,9 However, a variety of different sonography training programs and techniques exist to educate students.10–12 Sonography is one of the most commonly used imaging techniques. 13 Hence, ambulatory and clinical diagnostics could not be completed without sonography as a noninvasive, nonionizing imaging technique. In many cases, sonography is an integral part of the patient’s diagnostic examination. 14 However, the quality of the sonographic examination is strongly dependent on the training provided to the examiner. Therefore, a good practical training is needed to raise the diagnostic quality of the patient examination. 15 Furthermore, the clinical question should be quickly determined and the patients should be checked to determine if they are suitable for a sonographic examination. 16 A good theoretical understanding of this examination method would help young physicians to determine the proper indications and correctly interpret the results. The assumption is that sonography training should be incorporated into a medical curriculum to ensure that graduates have a profound basic knowledge of its application. Therefore, it was important to attempt to implement sonography training in a medical school curriculum but do it with limited resources.
Materials and Methods
In this observational, descriptive study, sonography training was implemented into a medical school curriculum and was evaluated. The training consisted of a voluntary laboratory practical. The laboratories were staffed with physician-trained students who offered peer teaching in small student groups (maximum three participants). Medical students enrolled in any clinical study semesters could take this course.
In addition, the required didactic seminar was provided by physicians with experience using sonography as part of students’ internal medicine training. After the seminar, which was held during the third clinical year of the curriculum, the students were examined with problem-/case-based tasks, based on the Internal Medicine Objective Structured Clinical Examination (OSCE). Due to the popularity of the laboratory practical, students often choose to participate in the laboratories before attending the mandatory didactic seminar.
The attitude toward the method in general (14 items regarding the role of sonography in clinical practice, the relevance in undergraduate education, and their particular role in future medical practice) was evaluated by two successive groups of medical students. The groups were given the identical questionnaires prior to the intervention (T0), directly after the intervention (T1), and four to six months after the intervention (T2). The demographic data at T0 were recorded.
At T1, the students were also asked to state the subjective value of the course. This assessment used five items to gauge student feedback: motivation of the teaching staff, comprehensibility, practical relevance, interactivity, and reasonable timing. In the laboratory practical, an additional item was added: student recommendation. The medical students could rate these dimensions on a 5-point Likert scale (1 = excellent to 5 = poor).
In the laboratory practical, skills were evaluated at three time points. During the laboratory practical devoted to procedural skills, the time needed to produce the picture (maximum two minutes) was measured. In addition, the preparation and interaction categories were assessed with five items, such as giving correct instructions for breathing maneuvers (maximum 5 points), orientation in the image (three items, maximum 3 points), and basic functions/knobology (six items, maximum 6 points), and they were rated with standardized checklists. For the evaluation of the imaging quality, five predefined common sonograms (cross section of the urinary bladder, longitudinal section of the abdominal aorta, longitudinal section of the right kidney, longitudinal section of the gallbladder, lateral intercostal section of the spleen) had to be produced by the medical students. The volunteer subjects who were scanned were students from each laboratory practical group. These images were evaluated by experts blinded to the study (consultants in internal medicine with more than 15 years of experience in sonography) and one trained student. The images were rated on a scale of 0 points (structure not visible), 1 point (fair quality/structure visible <50%), 2 points (good quality/structure pictured >50%), or 3 points (excellent quality/structure completely visible). A maximum of 15 points could be obtained per study.
In the didactic seminar, knowledge was assessed using a multiple-choice examination (10 questions on the topic of transducer function, ultrasound modalities, nomenclature, orientation of the sonographic image, and pathologies), and this occurred at all three time points. The questions were based on the content covered during the didactic lectures, and a maximum of 10 points could be achieved.
The study was approved by the Medical School’s Ethics Committee (project number 5806/13). Every participant was asked to give written consent. After receiving written consent, the students in both teaching units were provided with the questionnaires and the results of the tests that were recorded.
Statistical Analysis
The descriptive presentation of the results was performed using a percentage distribution and mean value (standard deviation [SD], respectively). Group comparisons were completed using one-factor variance analysis with measurement repetition. Interactions were analyzed by two-factor variance analysis with measurement repetition. A P value of .05 was chosen a priori.
Results
In the laboratory practical sessions, the participating medical student’s mean age was 23.7 years and the average time in the curriculum was 3.5 years. In the didactic seminar, the students’ mean age was 25.1 years and the average time in the curriculum was 4.9 years. A total of 60 students attended the voluntary laboratory practical. At T0/T1, 96.6% of the students provided data, and at T2, 62.5% provided data for this study. There were 158 medical students who attended the mandatory didactic seminar. The participation rate was calculated at 89.9% for T0 and T1, while 63.3% participated at T2. There were 42% of the students in the seminar who had already attended the laboratory practical tutorial.
The laboratory practical was rated by the students with a mean (SD) response of 1.1 (0.3), and the didactic seminar was rated with a mean (SD) overall response of 1.5 (0.7). In the free text comments, over 75% of the students stated that more sonography training possibilities should be provided. Furthermore, advanced training courses as well as individual opportunities to train independently were requested. Finally, 15 students (25% of the participants in the laboratory practical) indicated a need to make the laboratory practical courses mandatory.
The evaluation of the practical skills around the tutorial showed a significantly better performance in the procedural skills, with a mean (SD) increase from 6.2 (1.5) out of 14 points (T0) to 11.7 (1.2) by T1 (P < .001). Ten percent of the students obtained the full score by T1, which nobody reached by T0. By T2, the score decreased slightly with a mean (SD) of 10.5 (1.4) but remained significantly higher than at the beginning (T0) (P < .001; see Figure 1).
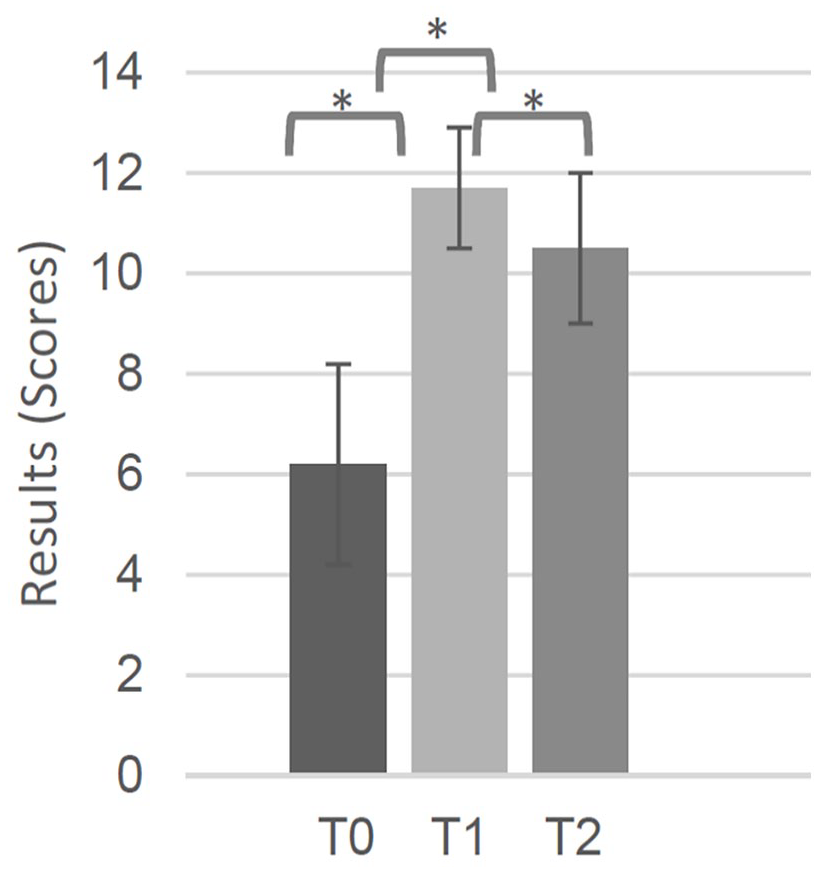
Procedural skills (mean ± standard deviation). *P < .001.
Across all the different laboratory tasks, a long-term learning effect could be observed. Nevertheless, there were large differences between the laboratory tasks observed longitudinally, especially in the postassessment (T1 vs. T2). In basic functions/device operation, the score significantly improved from a mean (SD) of 1 (0.5) at T0 to 4 (1.0) out of 6 at T1 but decreased to 3 (1.0) points at T2 (P < .001). In preparation and interaction (mean [SD]: T0, 3 [0.6] out of 5; T1, 5 [0.5]; T2, 5 [0.5]) and orientation in the image (mean [SD]: T0, 2 [1.0] out of 3; T1, 3 [0.3]; T2, 3 [0.4]), a persistent learning effect was achieved.
The overall imaging quality increased from a mean (SD) of 6.8 (2.3) out of 15 at T0 to 9.3 (1.9) at T1 (P < .001) but decreased again over time to 7.2 (1.9) points at T2 (see Figure 2). As in the procedural skills, depending on the type of image, heterogeneous outcomes were observed. A persistent improvement was observed in the imaging of the spleen (mean [SD]: T0, 0.6 [0.8]; T2, 1.1 [0.8]) and the right kidney (mean [SD]: T0, 1.3 [0.7]; T2, 1.8 [0.6]), both P < .05. In the imaging of the urinary bladder (mean [SD]: T0, 1.6 [0.9]; T1, 2.3 [0.5]), a significant short-term improvement could be shown (P < .001). Imaging the aorta seemed to have no learning effect that could be observed over all the time points. In the imaging of the gallbladder, a decrease (P < .05) of the skills appeared over time (mean [SD]: T0, 1.4 [1.1]; T1, 1.5 [0.9]; T2, 0.7 [0.8]).
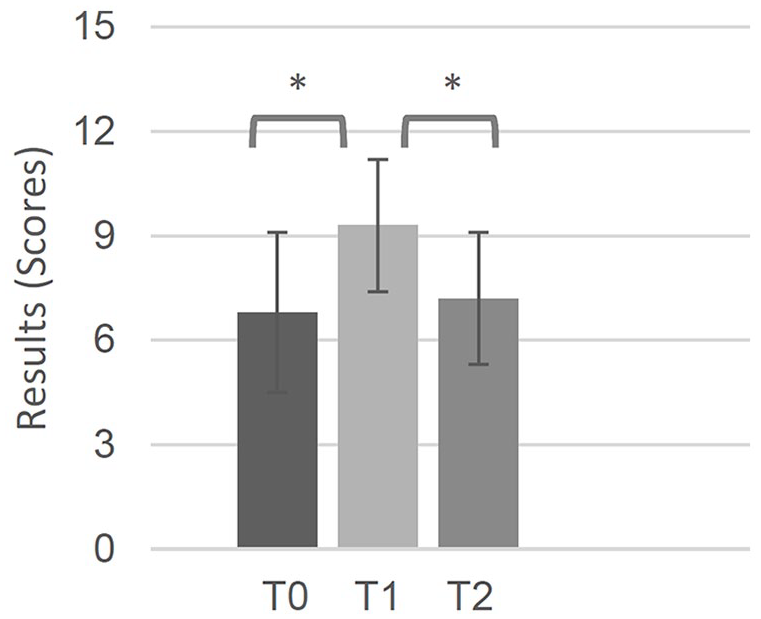
Overall imaging quality (mean ± standard deviation). *P < .001.
The time needed to produce the sonogram decreased significantly from 286 seconds at T0 to 197 seconds at T1 (P < .001) but increased again to 273 seconds at T2.
The knowledge test in the didactic seminar showed a significant sustainable knowledge growth with a mean (SD) score of 4.8 (2) out of 10 at T0, 8.4 (1.2) at T1, and 7.4 (1.5) at T2 (P < .001; Figure 3).
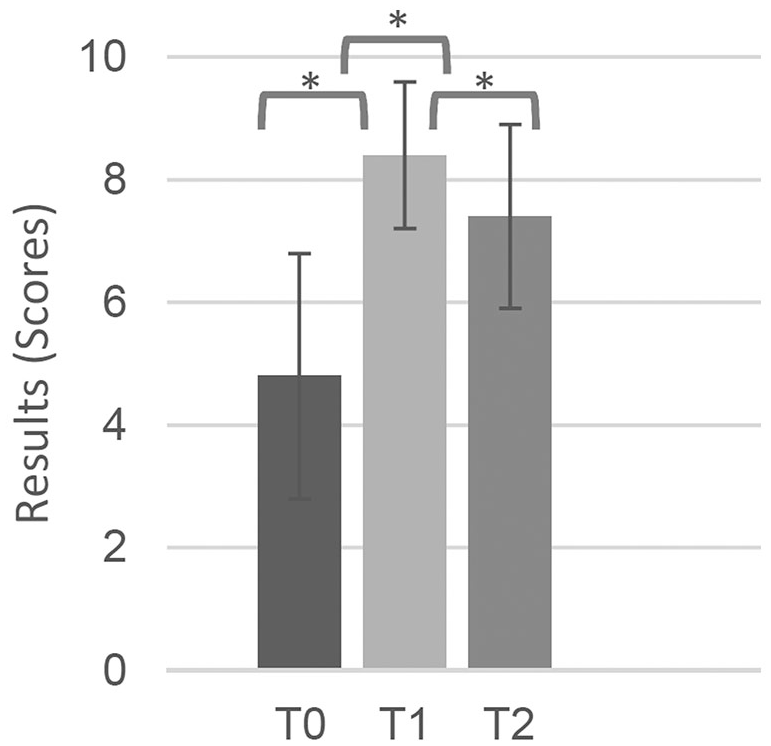
Multiple-choice test results (mean ± standard deviation). *P < .001.
At T0, the students demonstrated little knowledge in the content “transducers” (18% correct answers) and “ultrasound modalities” (20% correct answers). This improved in the didactic seminar over the short term (T1) and also over time (T2): 68% and 61% regarding transducers, respectively, and 85% and 52% regarding ultrasound modalities, respectively.
Students who had attended the laboratory practical before visiting the didactic seminar (42%) showed initially better theoretical knowledge (T0) than students without, but the knowledge levels equalized by the postassessments (T1 and T2).
The majority of the students judged sonography as not or slightly inferior to the use of computed tomography or magnetic resonance imaging. This opinion was improved throughout the laboratory practical (T0, 57%; T1, 67%; and T2, 74%) and the didactic seminar (T0, 70%; T1, 72%; and T2, 77%). Most students were motivated to focus more on sonography in their personal career (voluntary tutorial: T0, 86%; mandatory seminar: T0, 85%). In the laboratory practical, a persistent increase (T1, 95%; T2, 95%) was observed.
Discussion
A voluntary laboratory practical that is provided by peer instructors may increase medical students’ sonographic performance in a sustainable matter. Dickerson et al. 17 also concluded that the peer teaching method has an important place in sonographic training of students. By offering a small group format, this may help improve a student’s sonographic skills. 18 Nevertheless, in this study, the ability to operate the ultrasound device operation and the time needed to produce sonograms partially deteriorated over the time recorded. This may be due to the lack of sonographic training in between the laboratory and didactic seminar. Further educational research may be needed to determine the optimum number of ultrasound units for student training and additional educational materials (i.e., accompanying scripts).
This cohort of medical students was able to image the spleen and the right kidney sonographically with high quality. However, the sonographic quality of the gallbladder images deteriorated at T2. Since the volunteer subjects for scanning were medical students, there could have been a bias. Due to the laboratory setup, volunteer subjects were not always the same person being scanned. Still, this would not fully explain the difficulties with scanning one single organ. Interestingly, a study by Garcia de Casasola Sanchez et al. 19 found that their student groups had similar difficulties with gallbladder imaging. Possibly, in more complex imaging, the concept of peer teaching may have limitations, and more training time and repetition are needed. This corresponds with the medical students in this study having indicated their desire for more sonography training during their medical school education. However, sonography laboratory practicals are very resource intensive, so a careful evaluation is needed to determine whether an increase in training is possible, without risking a decrease in the overall educational quality. This also underlines the importance of also having an intensive train-the-trainer program.
Overall, a long-term improvement in the practical sonographic skills that were taught by peer teachers was observed. Furthermore, in this study, peer teaching offered benefits for both the peer teachers (learning by teaching) and the medical students. It also allowed for very small tutorial groups 20 that are mostly considered ideal by participants. 21 Ahn et al. 22 also showed that trained senior medical students could be useful when there is a lack of medical staff trained in sonography. Garcia-Casasola et al. 23 stated that in their experience, peer teaching leads to an adequate sonographic training level. In this context, more educational research into the optimal sonographic training for peer teachers would seem important.
The didactic sonography seminar led to a significant sustainable improvement of the theoretical knowledge. Beside enthusiastic teaching staff and well-structured lessons, the principle of “assessment drives learning” 24 (every student was tested in an OSCE) may have its impact on the favorable results. As profound basic knowledge should facilitate future training, 25 an OSCE can be recommended as a method to increase students’ motivation to occupy themselves with the teaching content.
After both teaching units, the relevance of sonography as a diagnostic method was rated higher. The comparison of the mostly earlier laboratory practical and the later didactic seminar suggests that progression in the clinical curricula ameliorates this attitude but also increases directly after the interventions. It is assumed that the teaching activities strengthen these medical students’ attitude. This may also affect graduate physicians’ use of unnecessary radiation exposure and cost-intensive examinations.
The laboratory practical tutorial appeared to increase students’ motivation to occupy themselves with sonography as part of their future medical career. The small group size and the commitment of the peer teachers may have contributed to increased student motivation. 26
In summary, the sonography training concept provided by this medical school curriculum may lead to an improvement of ultrasound competence in all three dimensions: knowledge, skills, and attitude. Peer teaching may be a helpful method to teach sonography skills, especially when there are limited educational resources available. Yet, careful and intensive training of peer instructors is needed to guarantee high-quality training for small student groups.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.