
Abstract
Urinoma formation is usually a consequence of trauma to the urinary collecting system. It is a collection of urine that is outside of the kidneys, ureters, or bladder. Similarly, a collection of bile outside of the biliary system is a biloma. Diagnosis of these is possible with a combination of imaging techniques such as sonography and computed tomography. A case is presented of a combination urinoma/biloma that formed after penetrating trauma to the superior pole of the right kidney and lower segment of the right liver lobe. Computed tomography was used to diagnose the pathology, and sonography was used to further characterize the lesion and place the drain that was used as treatment. Use of both of these modalities allowed the patient to receive a quick diagnosis and appropriate intervention.
A urinoma is defined as a collection of urine in a confined area bounded by a pseudocapsule. 1 Urinomas are generally located within the retroperitoneum but outside of the urinary tract. Urinomas are usually caused by blunt or penetrating abdominal trauma or iatrogenic injuries. 1 Blunt or penetrating renal injury occurs in approximately 1% to 5% of all traumatic abdominal injuries. 2 The formation of a urinoma occurs in 1% of all patients with renal trauma, unlike urinary extravasation, which is found in 2% to 18%. 3 Urinary extravasation is the leakage of urine along the collecting system, while a urinoma may result from extravasation by forming a capsule around the localized collection. There are three factors necessary for a urinoma to form: a functioning renal unit, a breach in the pelvicalyceal system, and ureteral obstruction, although the last factor often may not be demonstrated with imaging. After the urine collects, a fibroblastic reaction creates the fibrous capsule that surrounds it. 3 If the urinoma is left undiagnosed for too long, it can lead to a perinephric abscess, urinary granuloma, retroperitoneal fibrosis, paralytic ileus, systemic sepsis, or electrolyte imbalance. 4 Although urinoma is rare, prompt diagnosis and treatment are critical to avoid potentially serious complications.
A biloma is characterized as an abnormal intra- or extrahepatic bile collection most commonly due to a traumatic or spontaneous rupture of the biliary system. 5 It can also be associated with choledocholithiasis, cholangiocarcinoma, acute cholecystitis, tuberculosis, hepatic abscesses, or hepatic infarction. A biloma is a rare finding, usually seen in cases of high-grade liver injuries and reported to be found in 2.8% to 7.4% of blunt hepatic traumas. 5 No specific laboratory findings can identify the presence of a biloma, but they are usually symptomatic, which aids in the diagnosis. The patient may present with right upper quadrant abdominal pain, chills, fever, or nausea. The differential diagnoses would include lymphocele, abscess, hematoma, pseudocyst, liver cyst, and seroma. 6 While it is rare for either a urinoma or a biloma to form, it is exceptionally rare to find the two together due to their different etiologies. The following case presents a combination of a urinoma and a biloma in the liver.
Case Report
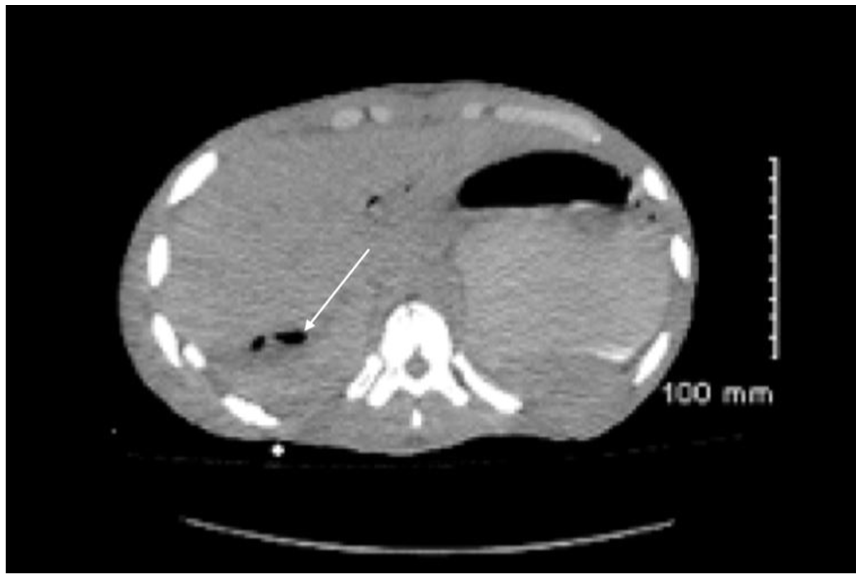
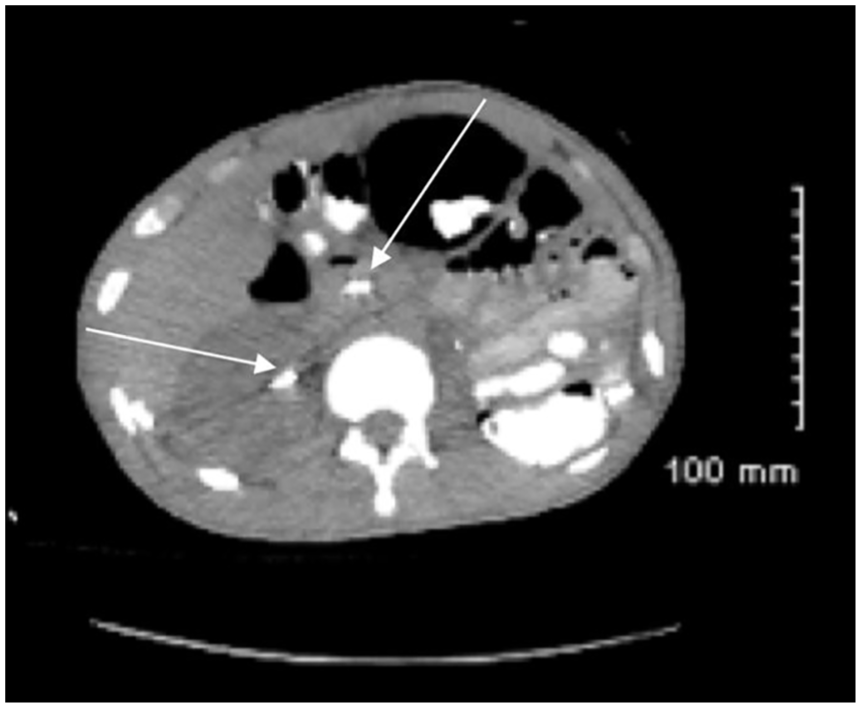
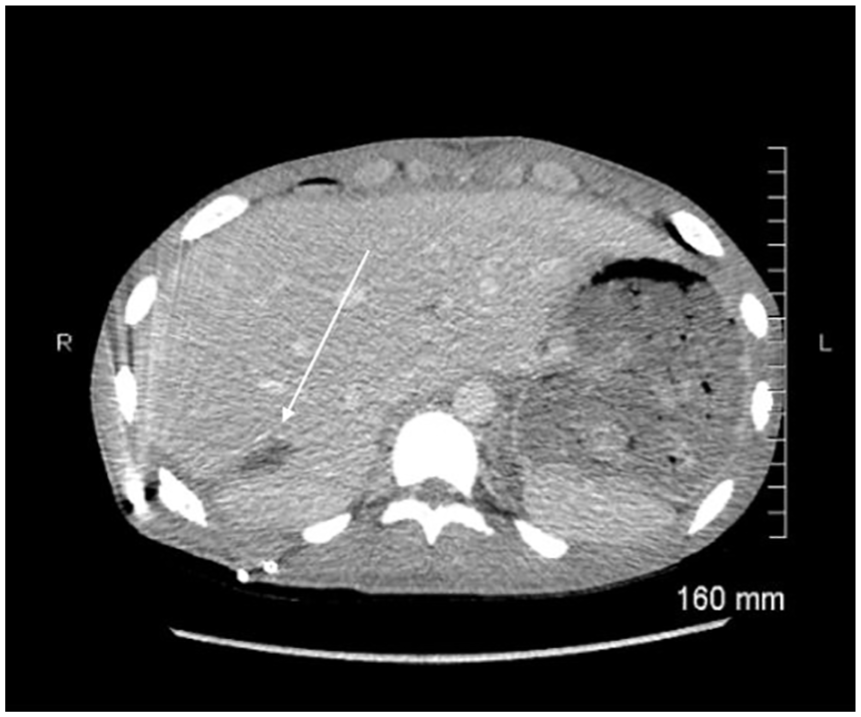
The patient in this case was a 19-year-old man who reported to the emergency department with an abdominal gunshot wound that lacerated the superior pole of the right kidney and the right hepatic lobe. These lacerations were classified as a grade 4 renal laceration and grade 2 hepatic injury. The clinical history included the patient’s complaint of acute abdominal pain and laboratory result of leukocytosis. Surgical history included recent left nephrectomy. In his initial emergency department workup, the patient underwent a targeted ultrasound of the right kidney to establish the presence or absence of blood flow. The superior pole was not clearly visualized in this initial study due to dressings covering the gunshot wound, but sufficient blood flow was visualized to document renal perfusion. No other abnormalities were seen on the initial sonogram due to limited acoustic windows and the trauma setting, which limited the sonographer’s time and access to the patient. During the emergency workup, the patient also received a computed tomogram (CT) of the abdomen and pelvis, with and without contrast media. The CT demonstrated that the bullet was lodged in the right posterior abdominal wall, along with internal damage in the right upper quadrant (Figures 1 and 2). It was then noted that the patient had a combination urinoma and biloma within the injured portion of his liver. This area measured 5.8 by 3.1 by 7.9 cm. A CT with contrast allowed the physician to determine how fluid collections were situated in the body. In this case, CT was especially helpful in demonstrating the urinoma component of the hepatic fluid collection. The use of the CT contrast injector, programmed for a 10-minute delay, allowed contrast to be seen extending into the fluid collection from the superior right kidney to the area of the liver laceration (Figure 3). No hydronephrosis or hydroureter was seen within the right kidney.
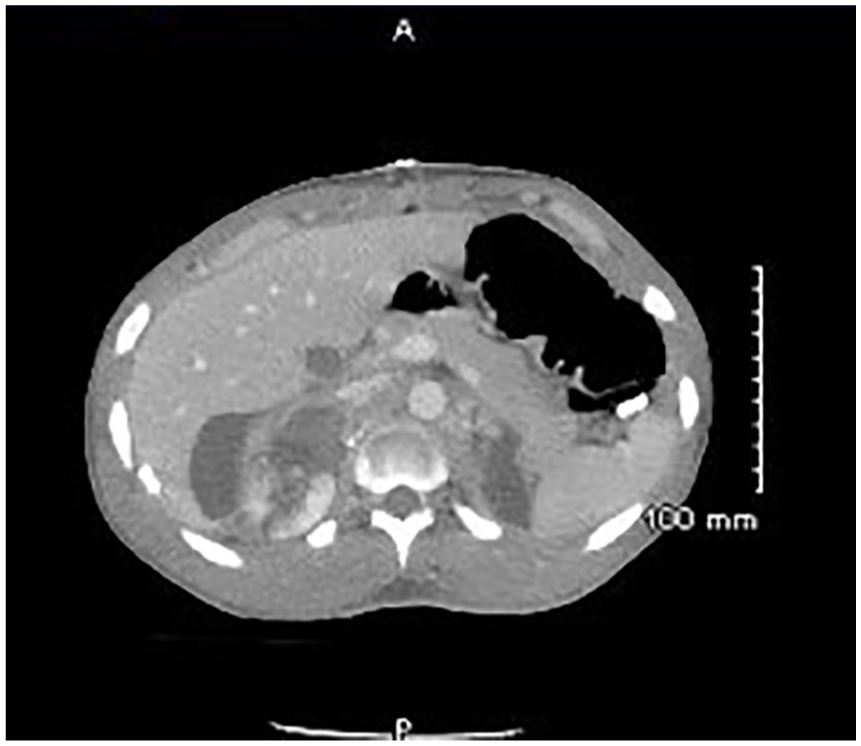
Initial computed tomogram without contrast showing the hypodense lesion adjacent to the right kidney.
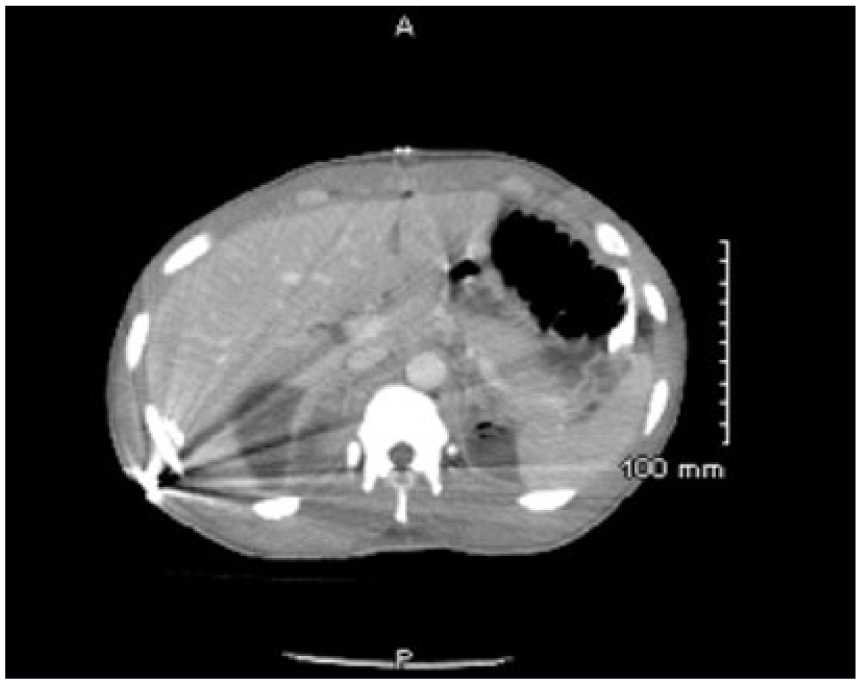
Computed tomogram of abdomen showing bullet lodged in posterior abdominal wall.
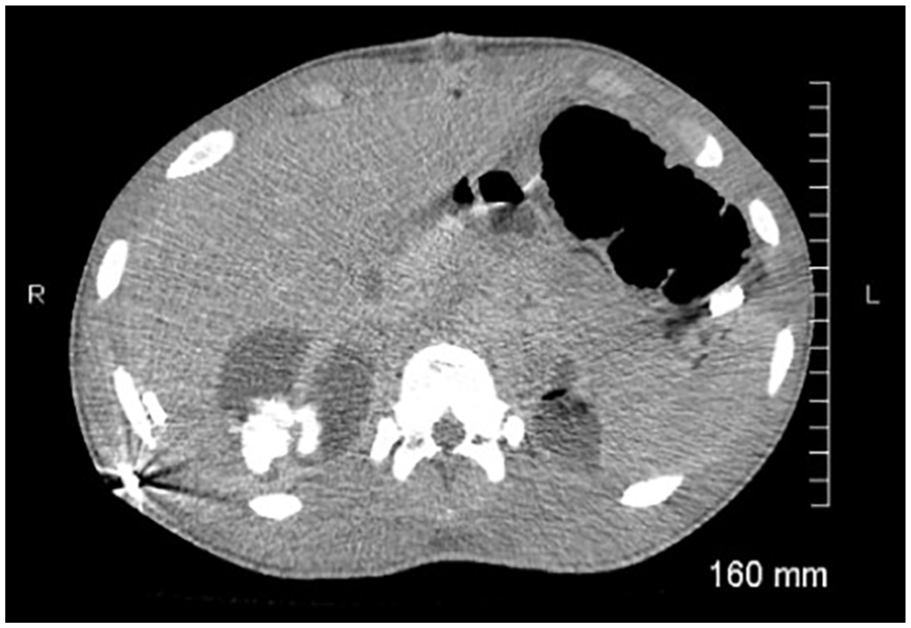
Computed tomogram with contrast, showing fluid entering the collection from the superior pole of the kidney.
The patient also received a nuclear medicine hepatobiliary scan, which showed accumulation of bile within the abnormal fluid collection in the inferior right hepatic lobe with consistent accumulation over the three-hour scan. The nuclear medicine images were unable to distinguish the gallbladder from the adjacent biloma. These findings, along with those of the CT, made it clear that the hepatic fluid collection was a combination urinoma and biloma. The patient also received an endoscopic retrograde cholangiopancreatography (ERCP), which showed the contrast leaking from the common bile duct into the hepatic fluid collection.
The urinoma/biloma was drained under sonographic guidance. A drainage catheter was successfully placed in the dependent portion of the fluid collection (Figures 4 and 5). Guidance was necessary because the collection was close to the lung and between the ribs. The use of sonography made this a safer and easier procedure for both the patient and the radiologist. A right nephroureteral stent and a stent in the common bile duct were also included in the patient’s treatment plan (Figure 6). The patient’s medical team hoped that the combination of drain tube and stent placement would encourage normalized drainage of urine and bile through the stents via a “pathway of least resistance” as well as decompressing the intrahepatic fluid collection with the drain tube. On follow-up CT, the hepatic fluid collection had significantly decreased in size, measuring approximately 5.2 by 1.0 cm, leading the physicians to expect continued recovery without need for further intervention (Figure 7), prompting removal of the drain. Another CT was performed approximately one month after the drain was placed showing the collection had nearly completely resolved (Figure 8).
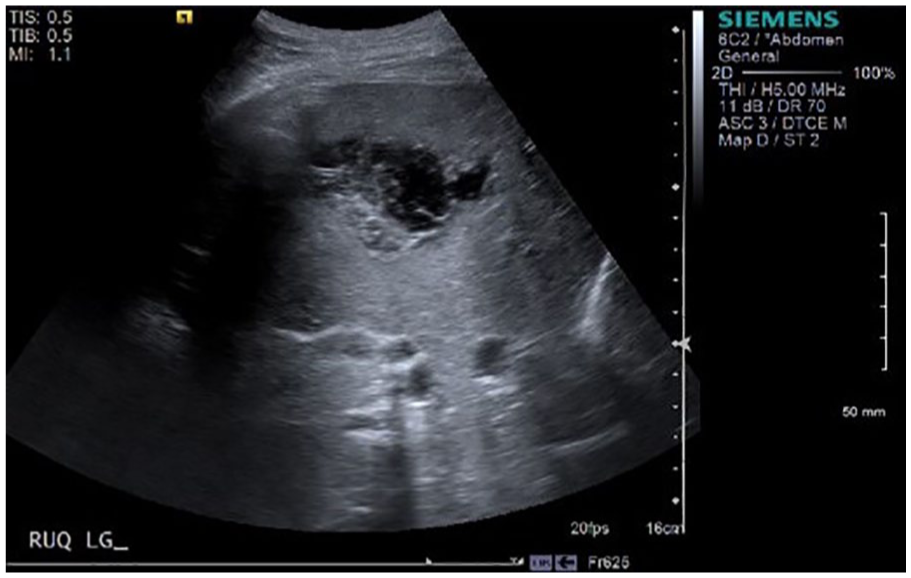
Sagittal gray-scale image of right lobe of the liver showing the complex collection.
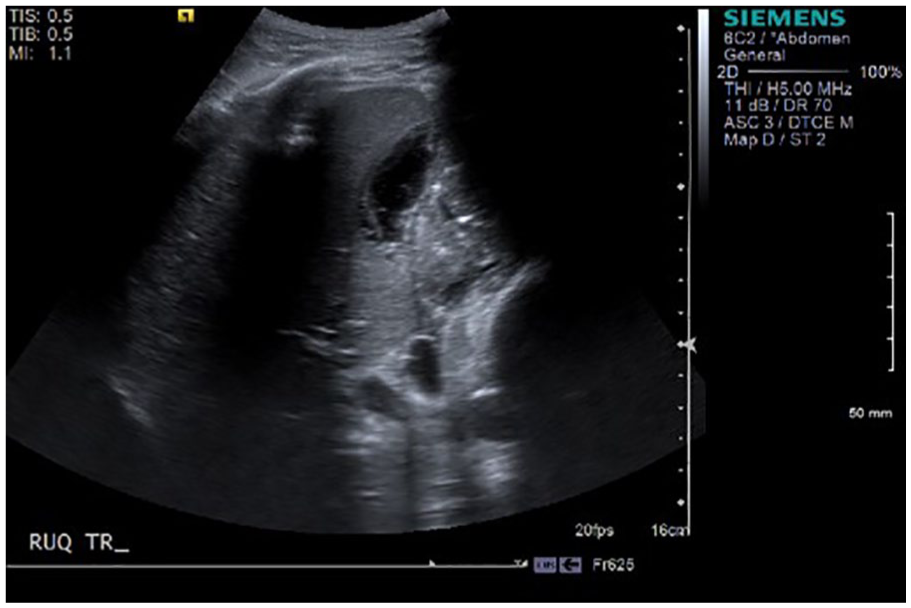
Transverse gray-scale image of the right lobe of the liver showing the collection immediately prior to drain placement.
Follow-up computed tomogram demonstrating reduced size of fluid collection following stent and drain tube placement.
Computed tomogram demonstrating placement of biliary and right ureteral stents.
Abdominal computed tomogram performed one month after drain placement.
Discussion
Urinomas are caused by disruptions in the urinary collecting system at any level, in the kidney, ureters, or bladder. 7 In this case, the kidney was damaged due to trauma; other causes could be obstruction, infection, or iatrogenic injuries. Risk factors that may lead to urinoma formation include a history of traumatic injuries, infection, or predisposing diseases that cause urinary tract obstruction. 8 A patient with urinoma may be asymptomatic or could experience hematuria, urinary disorders, nausea, vomiting, or abdominal pain due to pressure from the mass effect of the fluid collection. 5 In this case, the patient’s pain may have been attributed to the urinoma/biloma or to the trauma of the gunshot wound. His leukocytosis may have been associated with the urinoma/biloma combination or may have been due to a preexisting abscess in the patient’s left renal fossa. In the presence of extensive abdominal trauma, it is difficult to identify the exact cause of each abnormal laboratory value. Laboratory tests may show a progressive increase in serum creatinine or electrolyte imbalance. 8
Urinomas have the potential for a good outcome if they are diagnosed early. If not, there may be complications such as abscess formation, electrolyte imbalances, hydronephrosis, and paralytic ileus. 7 Untreated, many of these complications can lead to permanent loss of renal function. Sonography is the first-line imaging modality when urinary tears are suspected. 9 While renal trauma cases are generally evaluated with CT in the United States, there is recent literature explaining that sonography is equally effective and reduces the use of ionizing radiation. 8 This could produce a change in requesting diagnostic examinations, and therefore sonographers should be familiar with this pathology and their role in its assessment.8,9 In this case, the initial sonogram demonstrating renal perfusion was important to help reassure the medical team that the patient could safely undergo a CT with contrast since he had a previous left nephrectomy, leaving only the right kidney to function.
The sonographic appearance of urinoma is often characterized by multiloculated, thick-walled, complex fluid collections adjacent to the kidney 10 (Figure 9). Color Doppler may be used to detect the motion of urine flow, a “urinary jet,” into the urinoma from the site of the leak. CT with contrast is also useful in the visualization of urinary tears, with delayed imaging techniques demonstrating the accumulation of contrast in the urinoma over time. 10
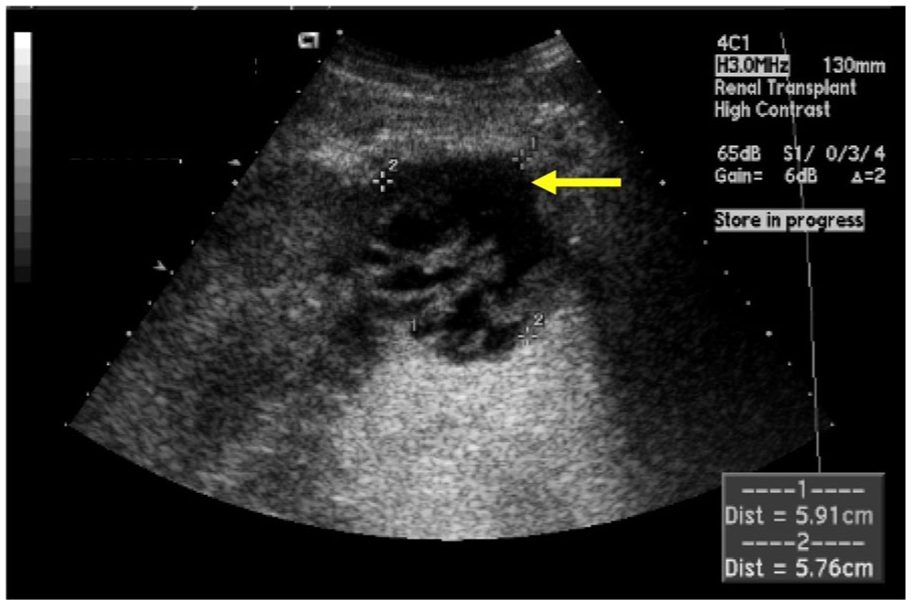
Sonogram of a complex urinoma found at the inferior pole of a transplanted kidney. Source: Afaneh et al. 15
Treatment options depend on the size and characteristics of the urinoma. Small urinomas may reabsorb spontaneously. If the urinoma is large or if the patient develops symptoms of sepsis, drainage is required. 10 The drain should be placed in the most dependent portion of the urinoma and can be placed under sonographic or CT guidance. It is also important to locate the cause of the urinoma formation and treat it. This could include placing a ureteral stent in order to assist healing of the collecting system. 7
Sonography is usually the first imaging modality used when assessing for fluid collections. 7 However, it is difficult to distinguish between urinomas, seromas, or abscesses, as they are all complex in appearance. Potential differential diagnoses include cystic masses, pelvic hematomas, seromas, and abscesses. The abovementioned jet seen on Doppler can be a helpful indicator of urinoma when evaluating with sonography. Overall, CT is currently considered the best modality to detect urinoma because of its ability to use contrast to demonstrate urine flow into the collection. CT may also be more beneficial in pinpointing the source of the leak. 7 While CT can aid in the diagnosis, sonography is unique in its ability to be used portably, facilitating bedside examination and rapid detection of abnormal fluid collections, which can be essential in trauma cases.
Sonography is generally the preferred modality used to diagnose a biloma because it is noninvasive, fast, and can clearly demonstrate this pathology. 6 Being able to diagnose these fluid collections is important, especially in posttraumatic cases, where therapeutic intervention is needed. Bilomas appear sonographically as single or multiple well-circumscribed anechoic lesions with posterior enhancement. They may be complex with debris or septations (Figure 10). A sonographic-guided percutaneous aspiration can helpful with diagnosis, as laboratory tests may reveal that the aspirated fluid contains a high concentration of serum bilirubin, which indicates bile leakage, and will confirm the diagnosis. 11 This aspiration can also be therapeutic and aid in resolving the biloma. Most small leaks can be managed by percutaneous drainage under imaging guidance, while larger leaks may require stent placement such as in this case. Cases involving major biliary injury will likely require surgical intervention. Delayed management can result in significant hepatic damage. 11 After treatment, sonographic follow-up is recommended. CT can be a useful diagnostic tool in these cases, but bile duct injuries tend to be visualized more clearly sonographically. Magnetic resonance imaging can differentiate between other liver lesions such as hematomas if the appearance is questionable on the sonogram or CT image. 6
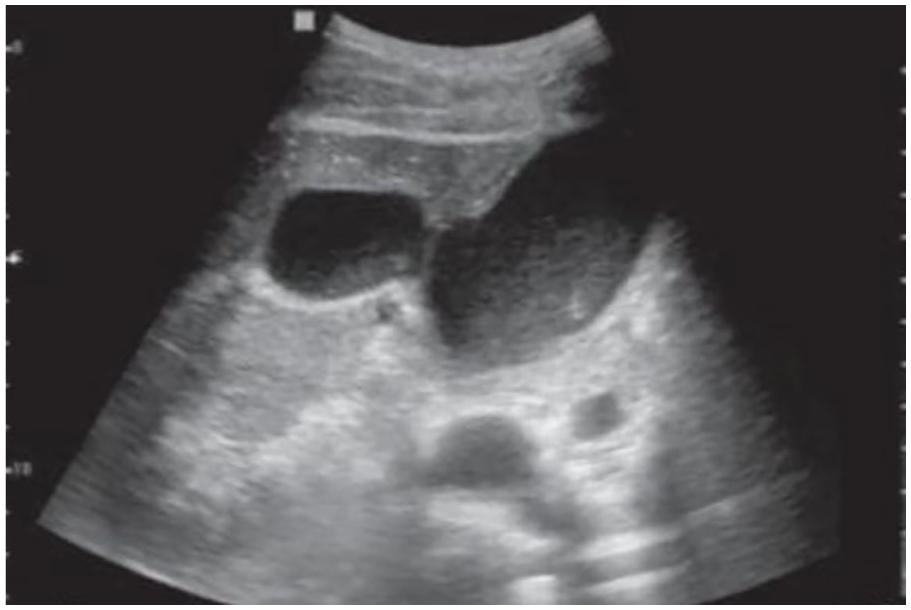
The image shows a perforation in the gallbladder wall and the presence of a fluid collection adjacent to it, which is likely a biloma. Source: de Hollanda et al. 16
Localization of abnormal fluid collections is a common task for experienced sonographers. But finding a fluid collection containing both urine and bile is challenging to find in the literature, which speaks to its rarity. This is likely because the bile ducts are located far from the urinary system in the body. Upon detection of the fluid collection in this case, the health care team struggled to define which organ injury was causing the accumulation. Using a combination of imaging modalities, it was confidently established that the lacerated kidney was leaking urine into the liver, accompanied by bile from nearby damaged bile ducts. Finding a urinoma in the liver is incredibly rare, and the additional combination with a biloma makes it even more unique. It is important for sonographers to pay close attention when scanning trauma cases to assist in an accurate diagnosis. This also allows for a successful treatment plan to be initiated, as this rare case required both urinary and biliary stents to prevent progression of this pathology. Careful diagnostic scrutiny was essential to this case because the actual diagnosis, while unexpected, strongly affected the treatment plan as the patient required both urinary and biliary stents to discourage the collection from filling again.
Conclusion
The unique pathology in this case was diagnosed using a combination of imaging techniques, specifically sonography, CT, and nuclear medicine. Sonographically, urinomas can appear as multiloculated masses with thick walls and hypoechoic features. In contrast, bilomas do not generally have thick walls and hypoechoic features, and they are typically not complex in appearance. This mixed fluid collection was unique because urinomas rarely form within the liver and do not generally coexist within the same space as a biloma. It is important for sonographers to recognize traumatic fluid collections and expedite the necessary intervention. Drain placement conducted under sonographic guidance is often a successful treatment method and can prevent the collection from progressing into an abscess, causing further damage in trauma patients.
In this case, sonography had the potential to have a more significant role and could have saved the patient from the ionizing radiation through repeated CT examinations. Currently, the American College of Radiology’s Appropriateness Criteria do not directly address this specific case, as the patient had abdominal pain that was a result of trauma. 12 While CT was useful in the diagnosis, it was not necessary for monitoring the posttraumatic fluid collection. During the sonographic-guided drain placement procedure, there was a clear window of the collection (Figures 4 and 5), meaning that it could have been followed up sonographically in the following weeks instead of by CT. According to the Image Wisely and Ultrasound First campaigns, sonography should be chosen rather than ionizing radiation examinations to prevent excessive x-ray exposure.9,13,14 As imaging is used more often in health care, it is important to consider sonography first as it plays a prominent diagnostic role, given its portability, cost-effectiveness, and limited ionizing radiation dose. Sonography plays a vital role in the diagnosis and treatment of both urinoma and biloma whether they appear together, such as in this case, or separately. It is essential for sonographers to recognize and fully evaluate these pathologies to support effective treatment and optimal patient outcomes.
Footnotes
Acknowledgements
The authors thank Sa Phan, RDMS, RVT, Klaira Ekern, RDMS, RVT, and Emily Bromagen, RDMS, RVT, for their assistance, leadership, and guidance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.