
Abstract
Fournier’s gangrene is a rare type of necrotizing fasciitis specific to the superficial fascia and subcutaneous tissues of the external genitalia, perineum, perirectal, and ischiorectal regions. It is usually diagnosed clinically, and imaging is used to support the diagnosis, assess the extent of the necrosis, and aid in surgical planning. Computed tomography (CT) is the primary imaging modality to diagnose Fournier’s gangrene, usually after symptoms are severe. Sonography may be used to diagnose early stages of this disease and to differentiate it from intrascrotal pathology or benign cellulitis. A case of Fournier’s gangrene is presented that discusses sonographic findings of Fournier’s gangrene and the disease process.
Keywords
Introduction
Necrotizing fasciitis is the necrosis of soft tissue, which can lead to eventual widespread systemic toxicity and high mortality rate. Fournier’s gangrene is a rare type of necrotizing fasciitis specific to the superficial fascia and subcutaneous tissues of the external genitalia, perineum, perirectal, and ischiorectal regions.1,2 The appearance of this disease process was first described by venereologist Jean Alfred Fournier in 1883. 3 Due to its rapid onset and spread, Fournier’s gangrene is lethal without surgical debridement. Fournier’s gangrene is usually diagnosed clinically, and imaging is used to support the diagnosis, assess the extent of the necrosis, and aid in surgical planning. Computed tomography (CT) is the primary imaging modality to diagnose Fournier’s gangrene, usually after symptoms are severe. 1 Sonography may be used to diagnose early stages of Fournier’s gangrene and to differentiate it from intrascrotal pathology or benign cellulitis. 4 The following case report discusses the disease process and sonographic findings of Fournier’s gangrene.
Case Report
A middle-aged man with a history of morbid obesity and renal calculi presented to the emergency department with hematuria, bilateral flank pain, and a red, swollen scrotum. A 2-cm open wound in the left perineum was noted on physical examination. Laboratory results showed elevated white blood cell count. Computed tomographic images through the abdomen and pelvis, following a renal stone protocol, showed a nonobstructing left nephrolithiasis as well as a left ureteral calculus. Fat infiltration and gas were visualized in the left groin region, consistent with necrotizing fasciitis (Figure 1). A scrotum and contents sonogram was ordered to further evaluate the extent of the necrotizing fasciitis to the perineum and scrotum, which had not been included in the CT imaging.

Axial CT image of the pelvis demonstrating fat infiltration and foci of gas (arrows) in the left groin region.
Sonographic evaluation of the scrotum was done using a Philips iU-22 ultrasound system (Philips Medical, Bothell, Washington, USA) with a 12-MHz linear array transducer. Both testicles were normal in size and echotexture, with no intratesticular masses. Both epididymides and testicles displayed normal vascularity with color Doppler. The left spermatic cord was enlarged to 3.44 cm in thickness (Figure 2). Marked skin thickening and edema were visualized, with the right and left scrotal walls measuring 1.70 cm and 1.82 cm, respectively (Figure 3). A moderate amount of subcutaneous air was visualized in the left inguinal region and scrotum (Figures 4 and 5), which corresponded to the gas seen on the prior CT scan. These findings were consistent with Fournier’s gangrene.

Sagittal gray-scale image of the left spermatic cord demonstrating marked thickening to 3.44 cm.
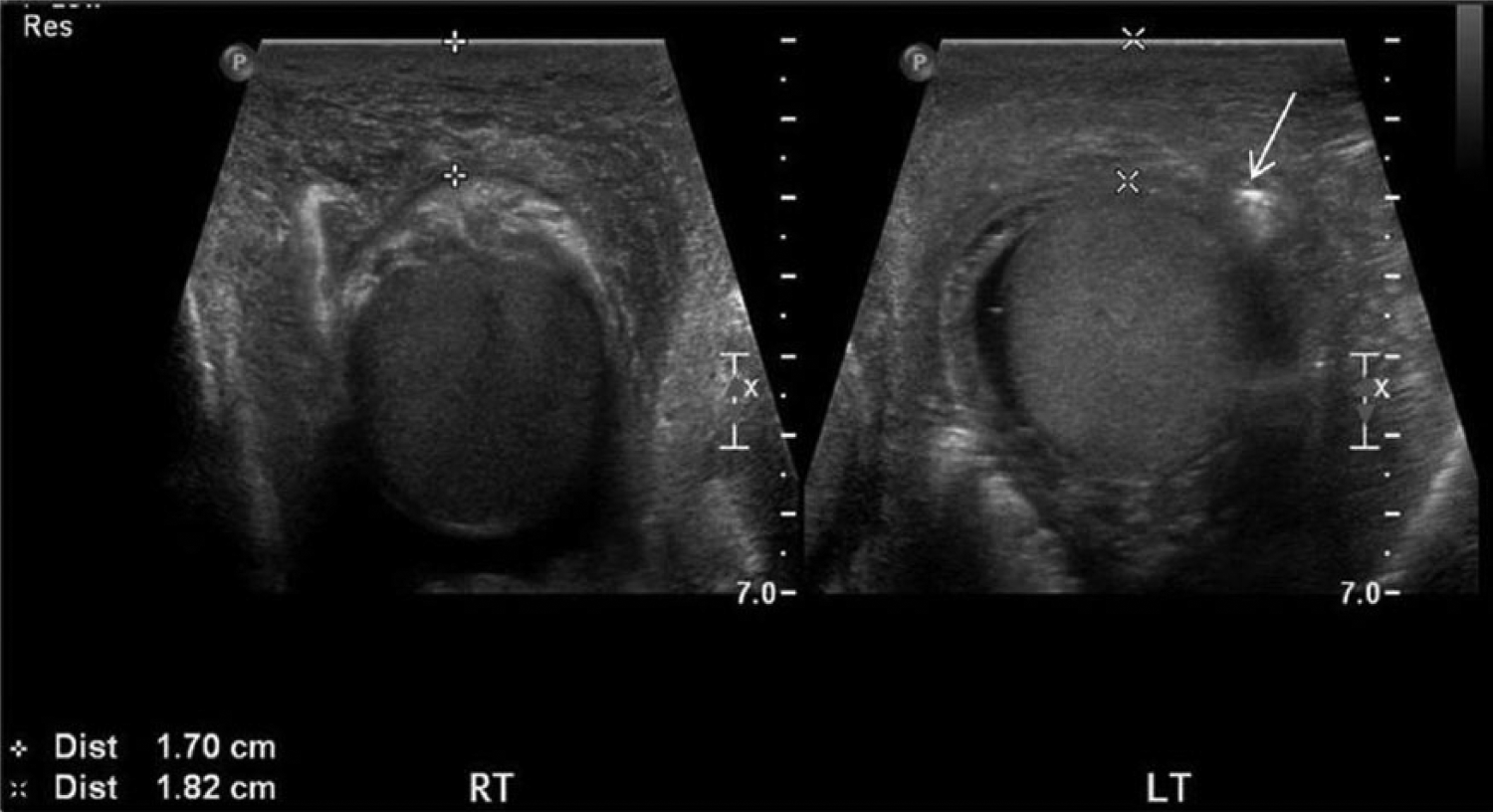
Dual transverse gray-scale images of the right (RT) and left (LT) testicles showing scrotal wall thickening. The left scrotal wall also displays a hyperechoic focus (arrow), which represents subcutaneous air.
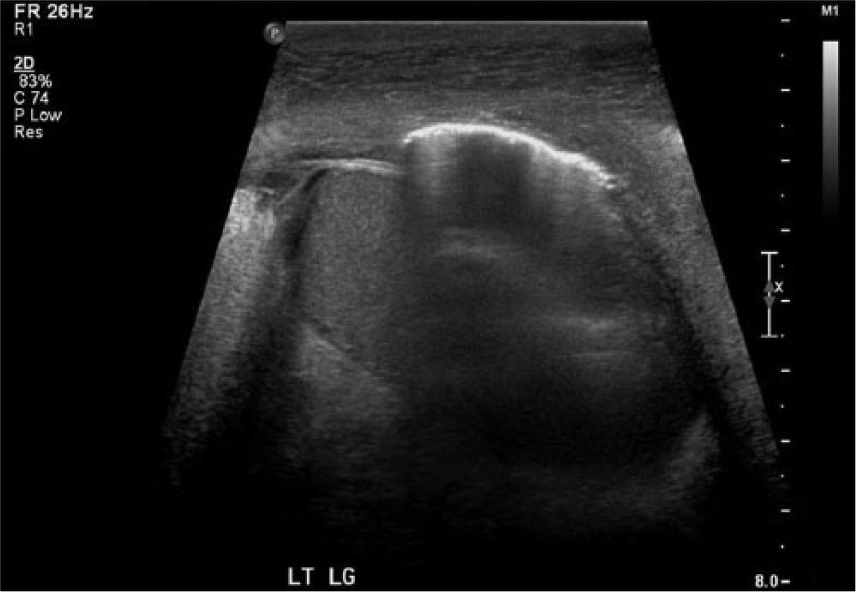
Sagittal gray-scale image of the left testicle demonstrating hyperechoic foci with reverberation artifact and “dirty” shadowing from air within the scrotal wall.

Transverse gray-scale image of the inferior left testicle demonstrating air within the scrotal wall.
A surgical consult was recommended because of the potentially lethal course of this disease process. Surgery was done that drained, irrigated, and debrided purulent material from the scrotum and perineum. Debridement vacuum therapy was the decided method of treatment following the procedure. Postoperatively, the patient was closely monitored for 2 weeks before being discharged from the hospital.
Discussion
Fournier’s gangrene is, in most cases, caused by a multi-organism infection. Escherichia coli, Bacteroides, streptococcus, staphylococcus, clostridium, and klebsiella are the most common types of bacteria that cause Fournier’s gangrene. 3 Bacteria tend to ascend from an external site of trauma near the scrotal or perineal area.5 –7 These organisms cause the formation of thrombi within blood vessels, which eventually leads to tissue ischemia and death.5 –7 About 500 to 1000 cases of Fournier’s gangrene are diagnosed each year in the United States.5,7 This potentially fatal disease process particularly affects patients with an underlying condition or suppressed immune system that makes them susceptible to infection. 8 Diabetes mellitus and chronic alcohol abuse are the 2 most common comorbidities of Fournier’s gangrene.1,8 –11 Men are 10 times more likely to acquire Fournier’s gangrene; however, women and children can also be affected.4,6
Patients may present with pain and fever even before any external cutaneous lesions are visible. Recognizable signs and symptoms are typically seen 5 to 7 days after onset of the disease. 12 Common clinical signs are bullae and crepitus. Bullae are air- or fluid-filled round prominences along the skin surface, while crepitus is a crackling and popping sound heard with palpation of the skin secondary to the presence of air in the subcutaneous tissue. The affected area may have a strong odor caused by bacteria in the necrosis. With sequentially increasing severity, tenderness, bronze skin, tense edema, erythema, bullae, ecchymotic skin lesions, blisters, painless black ulcers, and grey necrotic tissue are common scrotal skin appearances with the progression of Fournier’s gangrene. Laboratory tests for a patient with Fournier’s gangrene typically demonstrate marked leukocytosis. 13
Fournier’s gangrene begins locally and results in the spread of inflammatory bacteria. Infection spreads rapidly through subcutaneous tissue along anatomical fascial planes at a rate of 2 to 3 cm per hour unless surgical intervention occurs. 14 Fournier’s gangrene is usually diagnosed clinically and is considered a surgical emergency.4,7 Mortality rates of Fournier’s gangrene are commonly reported between 25% and 35% even after surgical intervention, and there is an increase when there is a delay in diagnosis. 2 If the anorectal area is involved, the necrosis travels deep into the pelvis, infecting the spermatic cord and the perineum of the genitalia. Testicular involvement is extremely rare due to the protective tunica vaginalis and its separate blood supply arising directly from the aorta. If there are signs of necrotic testes, abdominal spread should be suspected.
A scrotal sonogram is often the first imaging examination ordered for patients presenting with scrotal and pelvic pain. There are numerous advantages in utilizing sonography for the diagnosis of Fournier’s gangrene. Sonography can detect Fournier’s gangrene early before symptoms are severe. A scrotal sonogram can identify subcutaneous air that will distinguish between Fournier’s gangrene and cellulitis as well as evaluate for intrascrotal pathology. Sonography allows reproducibility of the images and permits visualization of any other residing pathology. Portability of sonography allows for patient comfort and safety. 3 Recognition of the sonographic findings of Fournier’s gangrene is crucial to early diagnosis and treatment. It is important for sonographers to remember that a patient with Fournier’s gangrene may be in severe pain and every effort should be made to ensure patient comfort and safety throughout the duration of the examination.2,7,15
A high-frequency (8 MHz-15 MHz) linear array transducer should be selected to visualize the scrotum and contents. For the severely edematous scrotum, however, a lower frequency transducer may be necessary. 16 Typical sonographic findings include scrotal wall thickening and hyperechoic foci with “dirty” shadowing and reverberation artifact, indicating subcutaneous air. Subcutaneous air in the scrotum is considered the hallmark image in diagnosing Fournier’s gangrene, due to its presence before crepitus can be appreciated on physical examination. 9 A reactive hydrocele can be present on the affected side. The epididymides and testes are usually normal in size and echotexture due to their separate blood supply. Enlargement of the spermatic cord is characteristic in progressive infectious and inflammatory processes of the scrotum. Cine loops are an especially helpful tool and should begin from where the air is first visualized and proceed through the subsequent anatomy. Comparison images should also be used to visualize differences in scrotal wall thickening.3,14 –16 Computed tomography is often the imaging modality of choice for Fournier’s gangrene, usually after it is suspected clinically when symptoms like bullae and crepitus are noted. Asymmetric fascial thickening, fluid collections or abscess, fat stranding, and subcutaneous air can be demonstrated by CT. 4 Computed tomography also is helpful in surgical planning, as it may locate the source of infection and the extent of spread along the fascial planes. 3 Prompt diagnosis and treatment of Fournier’s gangrene are imperative. For the best possible outcome, antibiotic use should be started immediately, and surgical treatment should be performed as soon as possible after diagnosis. In order to remove all of the necrotic tissues, exploration and surgical debridement are required.1,4,5,11 A vacuum-assisted wound closure device is most commonly used postoperatively to reduce the amount of dressing changes and edema. 12 Without surgical treatment, Fournier’s gangrene is likely to be fatal. Sepsis and multi-organ system failure are the most common causes of death.1,2,7 –10
Conclusion
Fournier’s gangrene is a rapidly progressive infection with high mortality if not surgically treated. Sonographers must recognize the risk factors, clinical symptoms, and sonographic findings of Fournier’s gangrene to aid in the prompt diagnosis of this potentially lethal disease process. Early detection of Fournier’s gangrene with the use of sonography improves patient treatment and outcomes.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.