
Abstract
Situs inversus totalis is a rare condition of the organs being transposed within the abdominal and chest cavities. The cause of situs inversus is unknown, but it is a recessive trait. Complete situs inversus may be associated with other malformations, such as levocardia, dextrocardia, and Kartagener syndrome; congenital heart disease may be present in some cases. The case presented describes a patient with situs inversus totalis with detection of liver metastases diagnosed by 2D sonography, computed tomography, and biopsy.
Complete situs inversus results from the transposition of the visceral organs and main vessels within the chest and abdomen. The heart is located to the right of midline, along with the aorta, while the liver and gallbladder are located on the left side. 1 The internal arrangement of the viscera can be described as the “mirror image of normal,” and the organs are located on the contralateral side of the body. While situs can be determined in vivo of a fetus with an obstetric sonogram, recognition of those with undiagnosed situs inversus is important to reduce misdiagnosis and understand the location of pathology located in the visceral organs. In adults, laterality disorders are most often found as an incidental finding from imaging studies of unrelated pathology. 2
Case Report
An elderly woman presented to the emergency room with complaints of abdominal pain and left upper quadrant pain for 1 week. When asked about her symptoms, she denied nausea, vomiting, chills, or fever in accordance with her pain. She stated that she had difficulty controlling her blood sugar and had recently been diagnosed with diabetes type II. She had a history of left flank pain, along with a hiatal hernia. Prior computed tomography (CT) studies suggested a situs inversus anomaly (Figure 1). An abdominal sonogram was ordered to assess the area of pain. The examination was done with an iU22 ultrasound machine (Philips Ultrasound, Andover, Massachusetts) with a 5-MHz curved array probe.
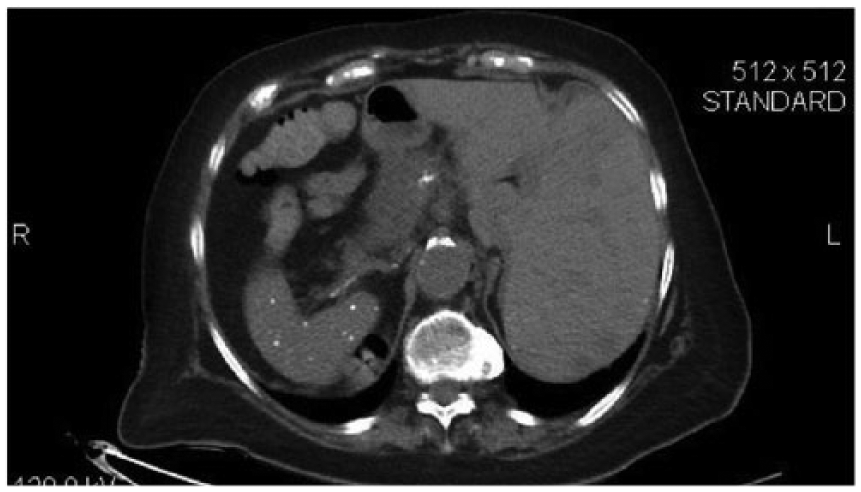
Abdominal computed tomographic image in the axial plane shows the liver on the left side of the body and the spleen on the right, suggestive of situs inversus. Note that the liver had a number of low-density regions throughout, suggesting metastases. Additionally, the image shows the granulomatous nature of the spleen.
The sonogram showed reversal of the aorta and inferior vena cava within the abdominal cavity, as well as the liver and gallbladder located on the left side. Multiple heterogeneous hypoechoic masses were seen throughout the liver parenchyma. The largest of these measured approximately 2 cm (Figure 2). Color Doppler imaging showed increased blood flow around the lesions. The gallbladder was shown to have sludge of midlevel echogenicity and an increased wall thickness (Figure 3). No pericholecystic fluid was seen. The spleen was shown to be granulomatous in appearance but was ruled out as a normal variant (Figure 1). The kidney had two components with two ureters noted. Crossed renal ectopia was seen in the lower right quadrant of the abdomen (Figures 4 and 5). The first and second components of the kidney measured 7.2 × 3.7 cm and 9.2 × 3.5 cm in the anteroposterior projection, respectively.
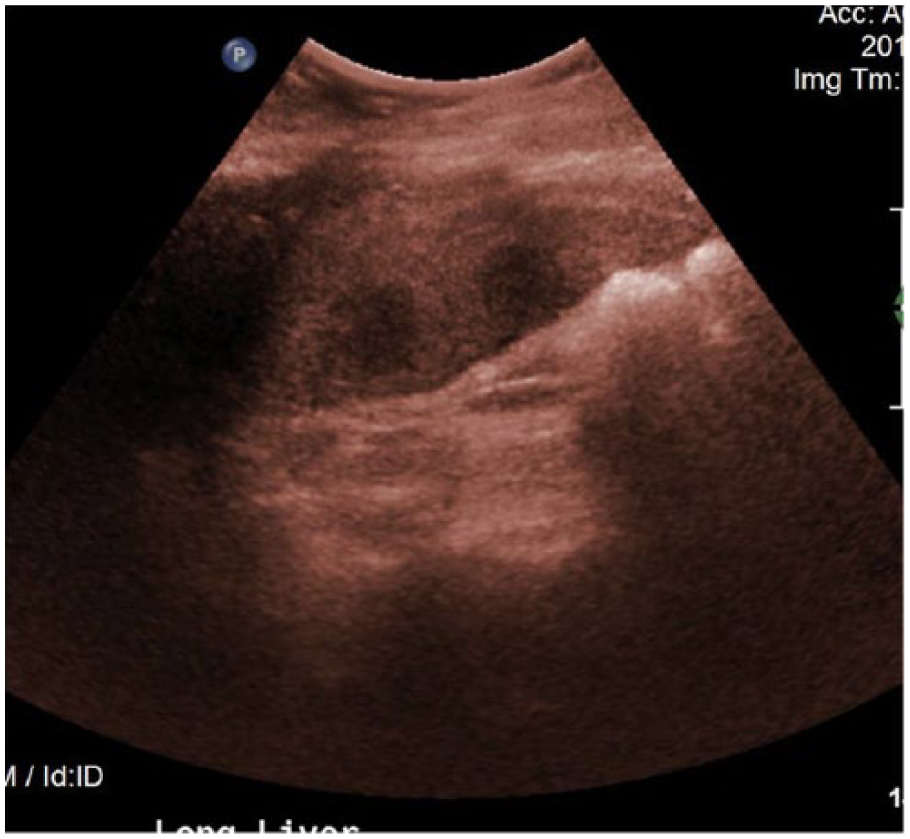
Longitudinal colorized gray-scale sonographic image (used to highlight the borders of the lesions seen) of the inferior portion of the liver shows several hypoechoic areas suggesting metastatic disease.
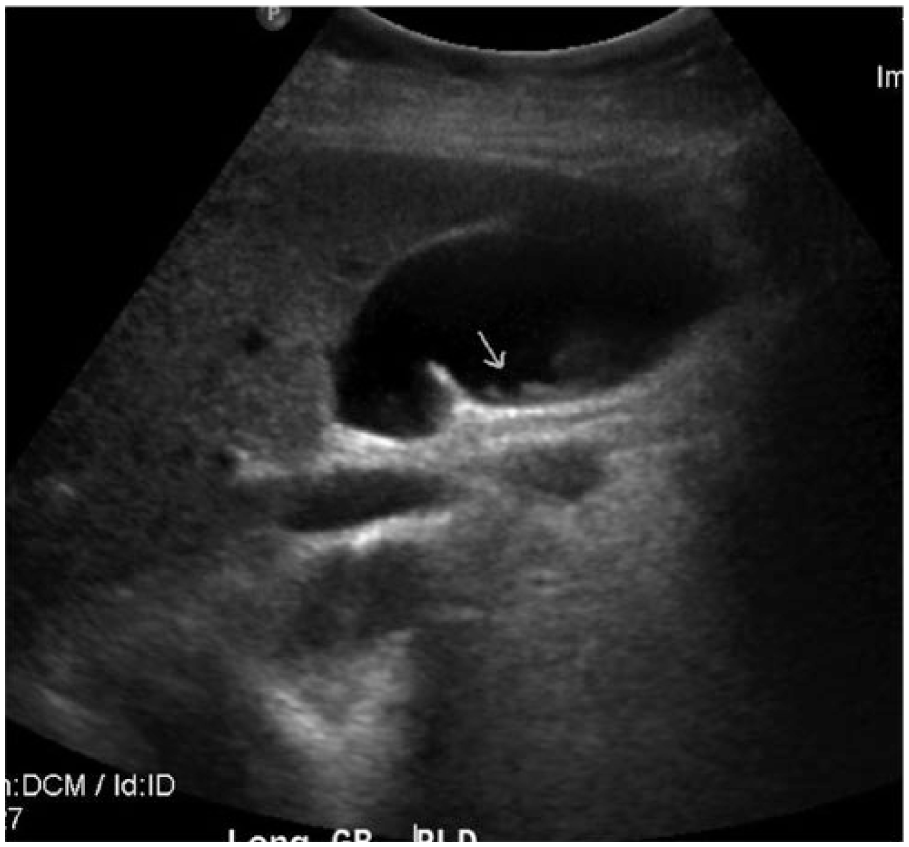
Longitudinal gray-scale sonographic image of the gallbladder in right lateral decubitus shows midlevel echoes secondary to sludge in the gallbladder (arrow).
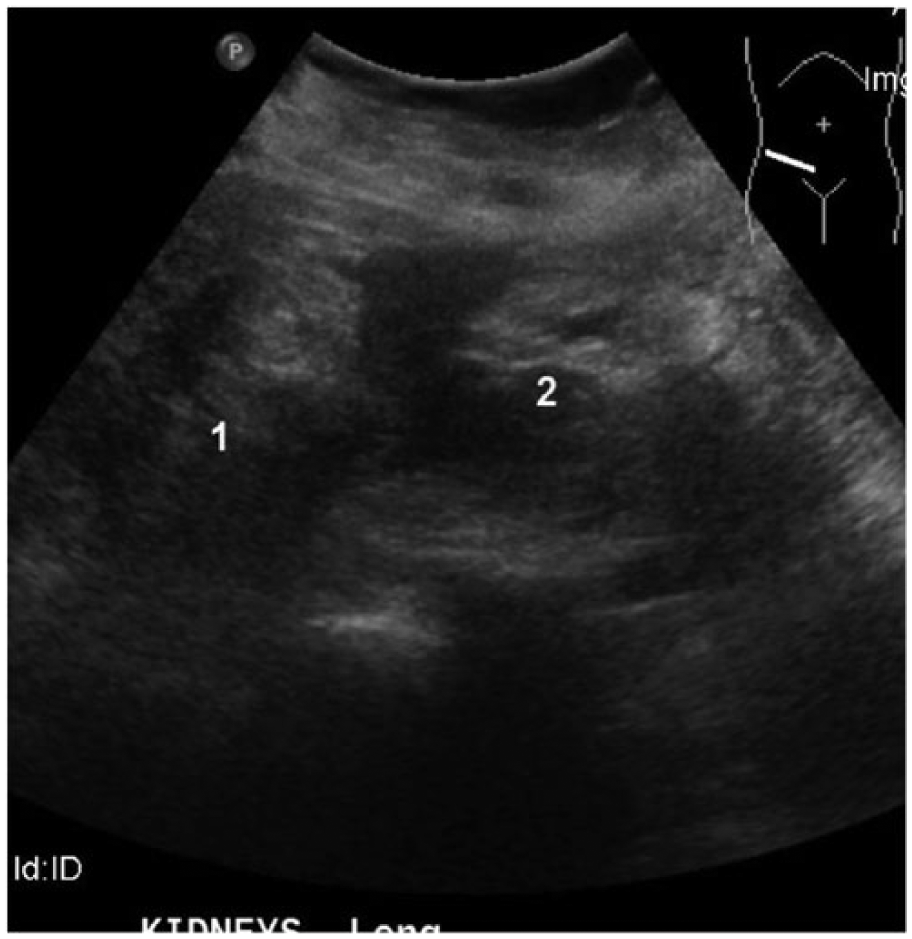
Longitudinal gray-scale sonographic image shows crossed fused renal ectopia in the midplane. Two kidney components were identified, labeled 1 and 2.

Cross-sectional abdominal computed tomography image shows a unilateral kidney on the right side, suggestive of crossed fused renal ectopia.
The interpretation of these studies concluded that the lesions seen throughout the liver were evident of multifocal hepatic metastatic disease. Because the patient did not have a history of cancer, a sonographically guided liver biopsy was ordered for further identification of the lesions. The biopsy was unremarkable, and the patient tolerated the procedure fairly well. The pathology report suggested that the lesions within the liver were adenocarcinoma of the pancreatobiliary, gastric, or ovarian system. A follow-up sonogram and CT were indicated to find the source of the metastases. The patient was scheduled for a colonoscopy and upper gastrointestinal examination to rule out gastric cancer.
Discussion
Complete situs inversus is a rare structural anomaly occurring in 0.01% of the population.3,4 It is a condition in which the internal organs of the abdomen and thorax are a mirror image of normal body position. Situs inversus tends to affect males more than females and has been found often to be familial. 5 The cause of situs inversus is not well understood, but it is recognized as a recessive condition and can be traced to early embryogenesis, when normal laterality of organs is determined in the third week of gestation. 6 Most cases may remain undiscovered until adulthood, depending on the severity or abnormalities present. 7 While no treatment is available for situs inversus, individuals affected still experience the same longevity of life, depending on the severity of symptoms. 3
Situs inversus can be divided into two categories: situs inversus totalis and situs inversus with levocardia. The patient in this case presented with situs inversus totalis, indicated by the heart pointing to the right side of the body and by complete reversal of the viscera in her abdomen. The rarer of the two, situs inversus with levocardia describes the complete reversal of viscera in the abdomen, but the heart has a left-sided apex. Almost all patients who have situs inversus with levocardia have congenital heart disease, while those with situs inversus totalis have only a 2% to 5% chance of having congenital heart disease. 4 In addition, Kartagener syndrome can be present—a type of primary ciliary dyskinesia of chronic sinusitis, bronchiectasis, and situs inversus. 5 Fifty percent of individuals with primary ciliary dyskinesia have Kartagener syndrome. Anomalies of the skeleton, spleen, and other abdominal organs have been associated with both types of situs inversus. 6 This can include polysplenia, asplenia, annular pancreas, horseshoe kidney, or diaphragmatic hernia.7,8
As well as situs inversus, crossed renal ectopia was noted on the sonogram and CT in the patient presented. Crossed fused renal ectopia occurs when the ectopic kidney travels across midline to lie on the opposite side of its intended location in the body. 9 Between the 4th and 8th weeks of gestation, the ureteric bud and metanephric blastema fail to fuse due to overbending and rotation of the caudal portion of the embryo. This results in the ureteric bud merging with the contralateral tissue.10,11 The incidence of crossed fused renal ectopia is 1 in 1300 to 1 in 7500. 11 Most crossed fused renal ectopia cases involve the left kidney crossing over to the right, as seen in this case.9,10 Sonography can play an important role in the diagnosis of this rare anomaly by showing the abnormal arterial and venous supply and diagnosing complications such as hydronephrosis and urolithiasis. 11
In a study by Galiatsatos et al. in 2006, 12 a retrospective study of 41 reports from 1980 to 2005 suggested that those with laterality disorders are at a higher risk for certain cancers. The authors found a number of primary cancers in patients with complete situs inversus, with the most common reported being renal cell carcinoma, gastric adenocarcinoma, and hepatocellular carcinoma. The patient in this case had a sonographic-guided liver biopsy, which suggested that the lesions could be one of the primaries listed above. There is no current evidence that situs inversus predisposes individuals to cancer, but further research is needed to confirm this potential connection.12,13
Surgical intervention can be dangerous if the patient has not had any prior studies to confirm situs inversus. Imaging studies and examination of this anomaly can prevent an incorrect diagnosis or severe complication prior to surgery. 4 Real-time abdominal sonography readily demonstrates the presence or absence of splenic tissue on the left side and shows the reversal of the abdominal aorta and inferior vena cava by color and spectral Doppler evaluation. The position of the liver, gallbladder, and vessels below the diaphragm can be readily evaluated.4,14 Chest radiography can be useful in identifying laterality disorders by focusing on the position of the heart in the chest. CT or magnetic resonance imaging can help visualize structures when further evaluation is necessary. Each imaging technique can help answer questions about specific anatomy in those with situs inversus totalis or other laterality disorders. 14 The use of a variety of imaging techniques improves recognition of situs inversus before invasive procedures take place.2,14 Recognition of this anomaly is important for physicians and imaging technologists to understand the arrangement of viscera inside the body to facilitate efficient diagnosis and treatment.
Conclusion
Situs inversus is a rare anomaly that may be an incidental imaging finding in patients who present with other pathology. The case presented relied heavily on imaging techniques to make the diagnosis and provide accurate results for patient management. Technical advances in sonography, CT, and other radiologic imaging techniques have greatly improved the ability to characterize and recognize anomalies to properly diagnose and treat patients with laterality disorders. It is important for all parties involved to understand the unique arrangement of anatomy in situs inversus patients to provide the best treatment and prevent delays in the surgical management of pathology.
Footnotes
Acknowledgements
We thank Allison Curry, RDMS, RVT, Dr Johnson Underwood IV, Dr Christopher Formen, Sharlette Anderson, RDMS, RDCS, RVT, and Christina Florido for their assistance, support, and guidance while preparing this case study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.