
Abstract
Hemangiomas are benign vascular tumors caused by an increase of blood vessels lined with endothelium. Diagnostic imaging such as sonography, computed tomography (CT), and contrast-enhanced magnetic resonance imaging (CE-MRI) can be used to detect hepatic hemangiomas, which are typically noted as incidental findings. However, in cases where hepatic hemangiomas demonstrate atypical appearances, this may suggest a possible malignancy. In such instances, a liver biopsy may be necessary for pathologic confirmation. A case is provided of a large hepatic mass that was initially detected on CT and further evaluated with sonography. Sonographic evaluation revealed characteristics suspicious for possible malignancy, including highly enlarged size, heterogeneous echotexture, and lobular contour. A biopsy ultimately determined the mass to be a cavernous hepatic hemangioma. The atypical sonographic appearance of the hepatic hemangioma in this case is worthy of consideration such that sonographers and the interpreting physician are aware of various presentations of this pathology.
Hemangiomas can be either capillary or cavernous depending on their microscopic makeup and location. Normally, capillary hemangiomas can be found in the skin or other subcutaneous tissues and are likely to resolve. Under a microscope, these tumors will appear to have small vessels that resemble capillaries. 1 Cavernous hemangiomas are more often seen in deeper structures, such as the liver, and are less likely to resolve. 1 Microscopically, cavernous hemangiomas are seen as larger cavities filled with blood. Hepatic hemangioma, a type of cavernous hemangioma, is the most common benign tumor of the liver, with an incidence rate of about .4% to 20%. 2 Most hepatic hemangiomas are solitary, hyperechoic, and homogeneous masses with well-defined borders that measure less than 3 cm. 3 However, these characteristics can change with increased size. Large hepatic hemangiomas can become heterogeneous, hypoechoic, and isoechoic due to necrosis, which can make them difficult to diagnose. 3 The case presented demonstrates the atypical appearance of a large hepatic hemangioma, which required liver biopsy to confirm the ultimate diagnosis, which positively impacts the patient’s outcome.
Case Report
A 45-year-old Caucasian male reported for a right upper quadrant sonogram and provided a history of renal failure as well as an abnormal abdominal computed tomogram (CT) performed at an outside facility. The patient reported no previous history of abdominal surgeries. The non-contrast abdominal CT, performed 8 days prior to the sonogram, was conducted as part of a pre–kidney transplant evaluation, due to kidney failure. The incidental findings of that CT examination were a large questionable hepatic mass as well as multiple enlarged pelvic, inguinal, and retroperitoneal lymph nodes. The questionable hepatic mass encompassed nearly the entire right lobe of the liver, measuring 17.2 × 11.1 × 13.7 cm. The mass was described as hypoattenuating with centrally located necrotic areas and peripheral areas of hyperattenuation. Based on these findings, a right upper quadrant sonogram was recommended to further evaluate the hepatic mass.
The sonogram was performed using Philips EPIQ 5G ultrasound equipment and an iU22 C5-1 5 MHz curvilinear array transducer (Philips Ultrasound, Bothell, Washington). The pancreas was not well imaged due to patient body habitus and presence of bowel gas. The right kidney had a normal sonographic appearance, with no masses. The gallbladder wall appeared thickened, measuring 6.6 mm, but no other biliary system abnormalities were noted (Figure 1). Sonographic evaluation of the liver showed fatty infiltration with a large, solitary, hyperechoic mass within the right lobe of the liver. The mass appeared heterogeneous with slightly lobular borders and measured 12.4 × 12.1 × 11.6 cm (Figures 2 and 3). Color Doppler evaluation demonstrated no significant hypervascularity (Figure 4). No significant posterior shadowing or enhancement was noted on the imaging study. The thickened gallbladder wall appearance was theorized to be due to a secondary reaction of chronic acalculous cholecystitis or the adjacent liver process.

Transverse gray-scale sonogram of the gallbladder showing gallbladder wall thickening thought to represent a possible secondary reaction of chronic acalculous cholecystitis or the adjacent liver process.

Longitudinal gray-scale sonogram of the liver showing a hyperechoic, lobular mass in the right lobe measuring 12.4 cm in length and 11.6 cm in height.

Transverse gray-scale sonogram of the liver showing a hyperechoic, lobular mass in the right lobe measuring 12.1 cm in width.

Longitudinal duplex sonogram of the liver demonstrating Doppler flow in the hepatic mass.
Based on the somewhat suspicious sonographic and CT characteristics displayed by the hepatic mass and enlarged lymph nodes, a liver biopsy was recommended to accurately diagnose the pathology and determine if the patient was a suitable candidate for renal transplant surgery.
A CT-guided biopsy of the hepatic mass was completed 10 days after the sonogram. Before the biopsy, CT noted the mass as measuring 17 × 11 × 14 cm (Figure 5). The biopsy used a lateral intercostal approach that traversed normal appearing hepatic tissue in route to the mass. Under CT guidance, a 17-gauge introducer needle was advanced into the mass, and four 18-gauge cores were obtained (Figure 6). The post-procedure CT image demonstrated peri-hepatic blood, which measured up to 10 mm in thickness (Figure 7). Frequent vital signs and hemoglobin levels were obtained to ensure patient stabilization.
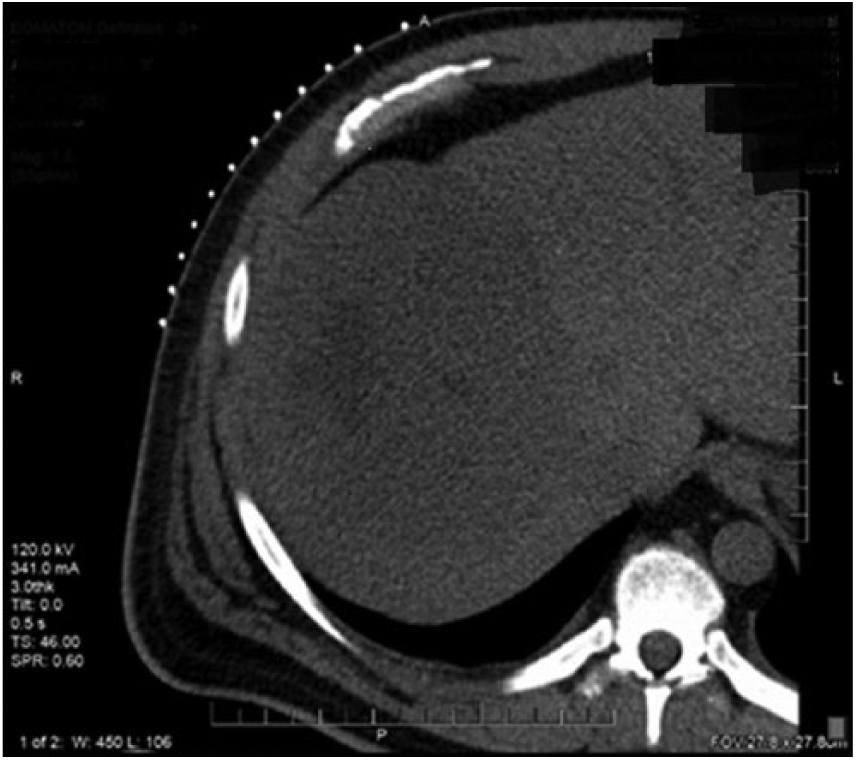
Axial computed tomogram without contrast of the abdomen showing a large hypoattenuating mass in the right lobe of the liver immediately before biopsy.

Axial computed tomogram without contrast of the abdomen showing the presence of the biopsy needle within the questionable hepatic mass.
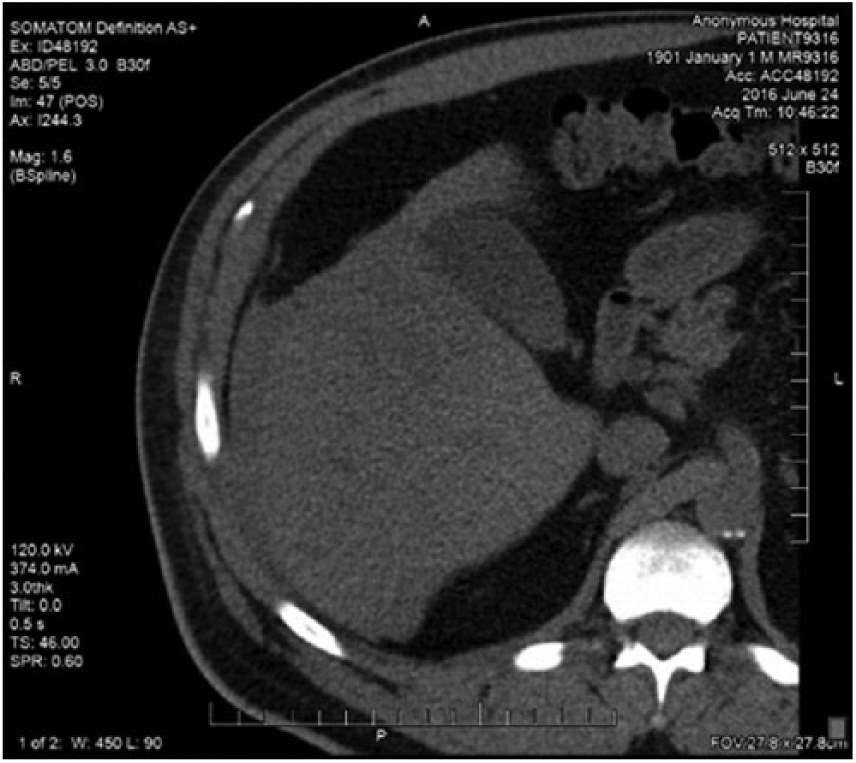
Axial computed tomogram without contrast of the abdomen showing the presence of peri-hepatic blood immediately after biopsy.
Four hours post-biopsy but before results were available, another CT was performed for surveillance of the peri-hepatic hemorrhage. The amount of blood was found to be overall unchanged, but heterogeneity of the blood was noted (Figure 8). Two hours after the follow-up CT, biopsy results were made available. Initial assessment of the gross specimen was noted as blood and hepatocytes with no malignancy seen on the touch preps. Microscopic examination found benign dilated vascular spaces lined by flattened endothelial cells, focally surrounded by hypocellular fibrous stromal tissue, resulting in the diagnosis of benign liver tissue with changes most consistent with cavernous hemangioma.

Axial computed tomogram without contrast of the abdomen still showing the presence of peri-hepatic blood noted 4 hours after biopsy.
Discussion
Hepatic hemangiomas are the most common benign liver tumor, being found in 20% of reported autopsy cases. 4 The cause of these relatively common lesions is still unknown. 2 They consist of clusters of blood-filled cavities that are lined with endothelial cells. Usually hepatic hemangiomas are fed by the hepatic artery. 2 However, they are not considered true neoplasms since they are lesions filled with vascular networks. Larger hemangiomas do have the potential to mimic more serious, malignant liver pathology such as hepatocellular carcinoma (HCC) as larger hepatic hemangiomas often present with variable echo patterns. 3 The large majority of hepatic hemangiomas do not cause the patient to have any symptoms and are normally discovered incidentally. Sometimes, though, large hemangiomas can cause hepatomegaly, which can result in some discomfort. A very large hemangioma may even cause nausea and vomiting, along with other digestive problems, but this is unlikely. 2 Other complications may include inflammatory processes, intra-tumoral hemorrhage, and compression of surrounding structures (eg, bile ducts, portal veins, and the inferior vena cava). The overall complication rate for hepatic hemangiomas varies from 4.5% to 19.7%. 5 Hemangiomas can fit in different classes depending on size. Small hemangiomas measure from a couple millimeters to 3 cm. Medium hemangiomas are those that measure up to 10 cm. Giant hemangiomas measure over 10 cm. 2
Overall incidence rates for hepatic hemangiomas fall between .4% to 20% of the total population, 2 but there are multiple factors that can increase the risk for developing hepatic hemangioma. Advancing age with an initial diagnosis range between 30 and 50 years can be a risk factor. Women are also more likely to have a hepatic hemangioma with a ratio of 4.5 to 1 compared to men at 5 to 1. The use of steroids may increase the development of a hepatic hemangioma. The use of oral contraceptives by women along with multiple pregnancies can also cause problems with preexisting hemangiomas. 2 Estrogen is thought to play a role in hemangioma enlargement, 6 but this has never been proven. 7
Sonographers should have a thorough understanding of the typical and atypical sonographic appearances of hepatic hemangiomas so that an accurate diagnosis of hepatic lesions is achieved. Typical sonographic characteristics, which are displayed by about 80% of hepatic hemangiomas, include solitary, smaller than 3 cm, location in posterior segment of the right hepatic lobe, homogeneous, hyperechoic, well-defined margins, and little to no flow on color Doppler.3,4 Hepatic hemangiomas may also present with posterior enhancement on a sonogram. Other than size, the case presented fits most of the typical characteristics of a cavernous hepatic hemangioma. As mentioned previously, smaller (less than 3 cm) hemangiomas are more often seen with the other typical characteristics. Atypical appearance most commonly results with increased size, often demonstrating a variety of echo patterns ranging from hyperechoic, isoechoic, to hypoechoic and appearing heterogeneous and lobular. These atypical characteristics may lead to misdiagnosis as the appearance can closely mimic malignant neoplasms, such as HCC. 3 HCC can appear as large, hyperechoic to hypoechoic, and with hypoechoic lesions throughout. 3 Other atypical appearances that may present with hepatic hemangiomas that can sometimes make a definitive diagnosis challenging include echogenic border and calcifications. One of the more common atypical appearances of a hepatic hemangioma is an echogenic border. These types of hemangiomas have an internal echo pattern that is usually partly hypoechoic. 8 Some reports have stated that 40% of all hemangiomas could have this atypical appearance. 8 Hepatic hemangiomas may also present with the atypical appearance of calcifications. This is quite rare in hepatic hemangiomas and is more common in gastrointestinal and retroperitoneal hemangiomas. 9 Hepatic hemangiomas may often be found with adjacent abnormalities, furthermore making diagnosis challenging. An additional abnormality that can be encountered is the sonographic evaluation of the fatty infiltrated liver. Although a fatty infiltrated liver is a common finding among patients, this has the potential to change the typical appearance of embedded lesions. With sonography, a hepatic hemangioma may appear hyperechoic to hypoechoic, with posterior enhancement, and with a hypoechoic border. 10 Around 20% of hemangiomas are hypoechoic on sonogram due to the increased echogenicity in fatty livers. 5 This can simulate other lesions like metastasis and HCC.
The benign lesion differential diagnoses for a hepatic hemangioma includes focal nodular hyperplasia (FNH) and hepatic adenoma. 3 Both may present as hyperechoic; however, FNH may also present as hypoechoic or isoechoic with a comparable size range to hepatic hemangiomas. FNH may also appear as an associated lesion, almost always appearing in women who have previously used oral contraceptives. 11 Hepatic adenomas can have variable internal echo patterns, ranging from hypoechoic to hyperechoic, similar to larger hepatic hemangiomas. However, a hypoechoic halo surrounding hepatic adenomas may be demonstrated and help differentiate them from hemangiomas. The malignant differential diagnosis for hepatic hemangiomas includes HCC, hypervascular metastases, and cholangiocarcinoma. 9 As mentioned previously, HCC tumors can present with a range of sonographic appearances. This tumor can range from hyperechoic to hypoechoic and may have multiple hypoechoic lesions througout. 3 Hypervascular metastases may have an echogenic border and rapidly filling characteristics. 9 Cholangiocarcinoma may present as heterogeneous. 9
Sonography can help differentiate between the various hepatic pathologies when all sonographic characteristics are carefully considered. This includes echogenicity, through transmission, texture, size, shape, and vascularity. Sonography is considered one of the best imaging modalities to diagnose typical hepatic hemangiomas. It has been reported to be more reliable than CT, especially with regards to smaller hemangiomas. 3 Sonography has a sensitivity of 94.1% and specificity of 80% for hemangiomas under 3 cm. 2 However, as this case demonstrated, larger hemangiomas are often difficult to accurately characterize and diagnose based solely on imaging findings, in which case liver biopsy may be performed to ensure accurate diagnosis. Although biopsy is not recommended, due to the vascular nature of hemangiomas, a percutaneous biopsy may be safely performed provided certain measures are adopted. This includes the use of a fine needle (18 or 20 gauge), avoidance of more than 2 needle insertions, and trying to traverse normal parenchyma on the needle course.12,13 It is vital for sonographers and interpreting physicians to familiarize themselves with the atypical appearances of hepatic hemangiomas. Knowledge of such characteristics could lead to a decrease in the number of liver biopsies performed if an accurate diagnosis can be established based on the results of multiple imaging modalities.
Other common imaging modalities used to diagnose hepatic hemangiomas include CT, contrast-enhanced CT (CE-CT), and contrast-enhanced MRI (CE-MRI). A less commonly used imaging examination is scintigraphy, which has a sensitivity of 78% and an accuracy of 80% when diagnosing hepatic hemangiomas. 14 With CT, the hemangioma typically appears as a well-defined hypoattenuating, nodular, homogeneous lesion. 4 With lesions larger than 5.0 cm in diameter, a lack of homogeneity is usually observed as a result of the presence of nonvascular areas of necrosis, fibrosis, or hemorrhage. 15 On a CE-CT, typical hemangiomas demonstrate peripheral nodule enhancement with progressive homogeneous filling toward the center of the lesion. 2 The fill-in pattern presented by the contrast agent will be isoechoic to the aorta, which has been noted to provide a 100% specificity rate. 16 This patient, however, was unable to receive a CE-CT due to renal failure. Even with CE-CT, hepatic hemangiomas still have the possibility of showing malignant tendencies such as hypervascularity. Atypical appearance seen on CT include rapidly filling hepatic hemangiomas. This is the immediate enhancement on arterial-phase CT. Adjacent abnormalities seen with CT include a fatty infiltrated liver and arterial-portal shunts. With nonenhanced CT, the lesion may be hyperattenuating relative to the fatty liver or may not be seen. 9 Arterial-portal shunts are commonly found with hepatic malignancies but can sometimes be seen in cases of hepatic hemangiomas.17,18 An arterial-portal venous shunt can be detected with helical CT or dynamic CE-MRI. 9
Hepatic hemangiomas on MRI usually appear well defined, homogeneous, hypointense on T1-, and hyperintense on T2-weighted images. 2 The hyperintensity on T2 sequences is one of the most reliable findings in the diagnosis of hepatic hemangiomas. 19 A threshold of 112 microseconds of T2 relaxation time results in 92% accuracy, 96% sensitivity, and 87% specificity for distinguishing hemangiomas from metastases. 20 Other studies have shown MRI to have a specificity and sensitivity of 98% as well as an accuracy of 99%. 21 On T2-weighted images, both hepatic hemangiomas and malignancy can still appear similar. 2 Atypical appearances on MRI include rapidly filling hepatic hemangiomas and hyalinized hepatic hemangiomas. This is the immediate enhancement on CE-T1–weighted MR imaging, which makes distinction from other hypervascular tumors difficult. 22 An example of another hypervascular tumor that “rapidly fills” includes islet cell metastases. 9 Accurate diagnosis in these cases is made with delayed-phase CT or MRI. This is because hemangiomas will remain hyperattenuating, whereas hypervascular metastases will not. 9 Hyalinized hepatic hemangiomas is another atypical appearance. Hyalinized hemangiomas have been noted as representing an end stage of hemangioma involution. 9 Hyalinization of a hemangioma changes its radiologic features, making diagnosis before biopsy nearly impossible. 9 Examination usually reveals extensive fibrous tissue and destruction of vascular channels. 23 Hyalinized hemangiomas usually present as hypovascularized and hyperintense at T2-weighted images. 23 Percutaneous biopsy is indicated in these types of cases. 4 Due to the overlap of benign and malignant imaging characteristics that can be displayed on sonography, CT, and MRI, it is essential that a definitive diagnosis be made in an effort to provide an accurate diagnosis and expedite the patient’s outcome.
A newly FDA-approved sonographic technique that may have prevented a biopsy in this case is contrast-enhanced ultrasound (CEUS). CEUS includes the injection of microbubble agents intravenously, which can then be imaged during the sonogram. Contrast in the liver can be seen during the arterial phase 10 to 20 seconds after injection and lasts 35 to 40 seconds during that phase. 24 Contrast fills the portal system during the portal phase and lasts 2 minutes. 24 The remaining observation time is termed the late phase. The contrast is then metabolized by the liver and expelled by the lungs with no risk of nephrotoxicity because it does not affect renal function. 24 The main use of CEUS in the liver is to differentiate between malignant and benign masses. Typical benign characteristics of CEUS include continuous contrast uptake with hyper to isovascular appearance compared to normal liver parenchyma. 24 Malignant lesions will typically display microbubble washout with a hypovascular appearance. 24
Typical CEUS characteristics of a hepatic hemangioma include spherical enhancement in the peripheral area of the lesion in the arterial phase with centripetal fill in. 24 In about half of the cases, the fill-in pattern will nearly complete during the late phase. The echogenicity will remain hyper to isovascular. 24
If left untreated, there are no data supporting a possible malignant transition from a benign hepatic hemangioma. Treatment is not typically necessary, and the lesion will be followed every 6 months or annually to evaluate for growth or significant change. If symptoms present or if there is rapid growth in size, surgical treatment may be considered. 2
The most common treatments include surgical resection (segmental or enucleation) and embolization. Surgical resection can be done in a minimally invasive manner with laparoscopy or robot surgery. 2 The removal of an entire hepatic lobe is not typically necessary. Embolization includes obliterating arterial blood supply to the tumor, which can reverse tumor growth. With both of these treatments, risk of postoperative morbidity is minimal. The hepatic hemangiomas do not normally reoccur. The long-term success rate is good for surgical resection but not well studied for embolization. 2
Conclusion
Typical sonographic appearance of hepatic hemangiomas may be described as solitary, smaller than 3 cm, location in posterior segment of right hepatic lobe, homogeneous, hyperechoic, well-defined margins, and little to no flow on color Doppler. Atypical appearance may be larger size, hypoechoic, isoechoic, heterogeneous, and lobular. This case study demonstrated a giant atypical appearing hepatic hemangioma that showed characteristics suspicious for malignancy, which resulted in liver biopsy for pathologic confirmation. In an effort to decrease the number of unnecessary invasive biopsies, sonographers and interpreting physicians alike must be familiar with the typical and atypical imaging characteristics of hepatic hemangiomas to allow accurate diagnosis and decrease the risk for the patient.
Footnotes
Acknowledgements
The authors thank Lesa Langlotz, RDMS, RVT, and Dennis Luetkemeyer, MD, for their assistance with this case study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.