
Abstract
Takayasu’s arteritis (TA) is a rare nonspecific inflammatory disease of unknown cause predominantly affecting the aorta and its main branches, coronary arteries, and pulmonary arteries of young females. Diagnosis of TA is typically achieved through computed tomography angiography (CTA) or magnetic resonance angiography (MRA), with sonography often used as a tool for surveillance of disease progression following diagnosis. A case of previously diagnosed TA is presented that demonstrates the effective use of sonography to monitor the progression of the disease with serial examination. The use of CTA and MRA allowed for accurate initial diagnosis, whereas sonography proved to be an effective diagnostic surveillance tool for proper tracking of the disease and its clinical manifestations. Increased sonographer awareness of TA including the clinical manifestations and sonographic characteristics associated with progression of the disease can improve patient outcomes in this potentially life-threatening disease.
Introduction
Takayasu’s arteritis (TA) is a form of systemic vasculitis mainly affecting the aorta and its large branches. 1 The disease typically originates in the large branches of the aorta, such as the subclavian, common carotid, and coronary arteries, and then progresses distally along the vessel path. The typical age of onset of TA is the second or third decade of life, and it is nine times more prevalent in females than in males. 2 Sonography, computed tomography angiography (CTA), and magnetic resonance angiography (MRA) are imaging modalities that can be used to properly diagnose TA and monitor changes associated with the progression of the disease. This case describes a patient with TA originating in the right and left subclavian arteries, which was diagnosed 4 years prior by CTA. To assess the progression of the disease, serial sonographic examinations were used to annually evaluate the carotid and upper extremity arteries to detect changes in blood flow, compared with previous examinations. Sonographic assessment was effective in demonstrating progression of the disease into the right and left axillary arteries, supporting its use as a surveillance tool for monitoring the advancement of TA.
Case Report
A 66-year-old Caucasian female originally presented to her physician for evaluation, reporting symptoms including hypertension, dizziness, low-grade fever, and cough. The patient also reported bilateral upper extremity weakness and left upper extremity claudication. Upon examination, the nurse was unable to auscultate a pulse in order to obtain a blood pressure in the patient’s upper extremities bilaterally. At that time, the patient underwent a CTA scan that demonstrated narrowing of the right and left subclavian arteries (Figures 1 and 2). There was no evidence of significant atherosclerosis or other possible causes for the arterial narrowing. These findings, along with the patient’s symptoms, led to the diagnosis of Takayasu’s arteritis. Upon diagnosis, the patient began a treatment plan that consisted of multiple oral medications including prednisone and methotrexate. The prednisone was prescribed to be taken daily, serving as an anti-inflammatory, to prevent the body from releasing substances that cause inflammation in the vessel walls affected by the disease. The methotrexate was prescribed to be taken weekly, serving as an immunosuppressant, which also acts as an anti-inflammatory when treating vasculitis. The addition of methotrexate to prednisone is used to treat TA when the disease does not respond to the use of steroids alone or when the dose of steroids must be reduced. 3
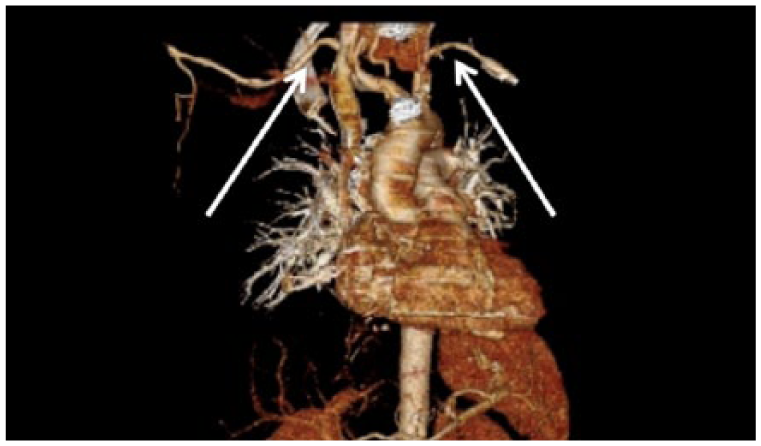
Three-dimensional reconstructed CTA image showing narrowing of the right and left subclavian arteries taken at the patient’s original examination when the diagnosis was made (arrows).
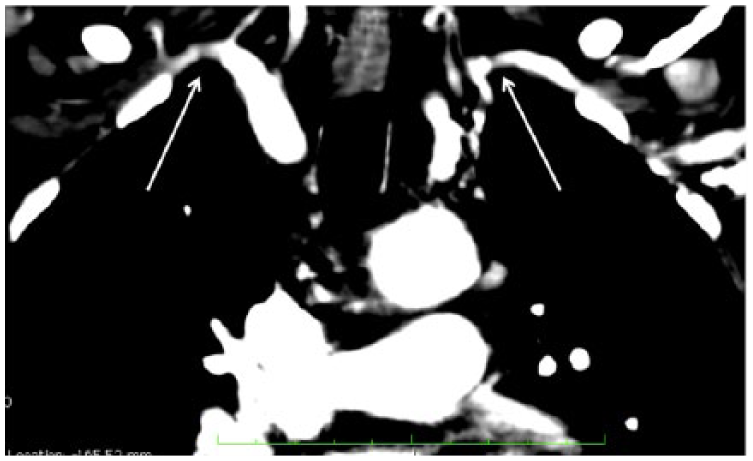
Coronal CTA image of the chest showing narrowing of the right and left subclavian arteries taken at the patient’s original examination when the diagnosis was made (arrows).
The patient presented to the sonography department for a carotid duplex sonogram and a bilateral duplex sonogram of the upper extremity arteries 3 years after her initial diagnosis. The patient had received both examinations annually, since being diagnosed 3 years prior, to evaluate the progression of the disease. Since the patient started medication for the treatment of Takayasu’s arteritis, the examinations performed annually had all been within normal limits and shown no progression of the disease. Sonography was performed using a Philips HD15 ultrasound system with a L12-3 broadband linear array transducer (Philips Ultrasound, Bothell, WA). The carotid duplex sonogram was within normal limits with no significant atherosclerosis or stenosis visualized in the internal, external, or common carotid arteries bilaterally. The bilateral duplex sonogram of the upper extremity arteries demonstrated normal blood flow in the right and left subclavian arteries, and no narrowing was detected. The right axillary artery demonstrated turbulent flow with a PSV measuring 185 cm/s (Figure 3). The right axillary artery spectral waveform appeared monophasic with the presence of spectral broadening. The right brachial, radial, and ulnar arteries were visualized and appeared within normal limits. The waveforms of the right radial and ulnar arteries appeared triphasic. The PSV of the left axillary artery measured 157 cm/s (Figure 4). The left brachial, radial, and ulnar arteries were visualized and appeared within normal limits. The waveforms of the left radial and ulnar arteries appeared triphasic. Based on the findings of these examinations, sonographic follow-up was to continue annually to monitor the progression of the disease.
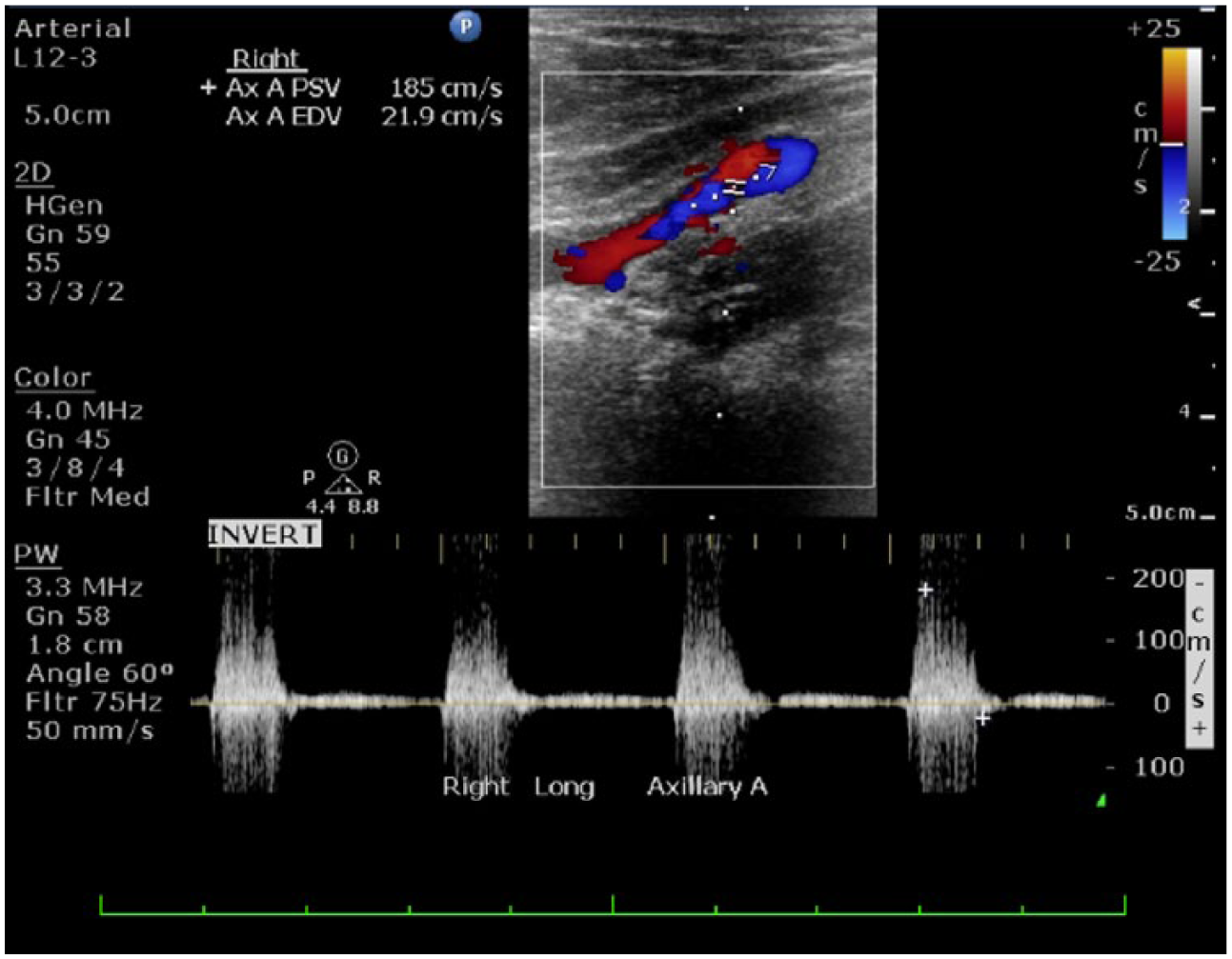
Longitudinal duplex sonogram from patient’s annual upper extremity sonogram 3 years after diagnosis showing turbulent flow of the right axillary artery with a PSV measuring 185 cm/s.
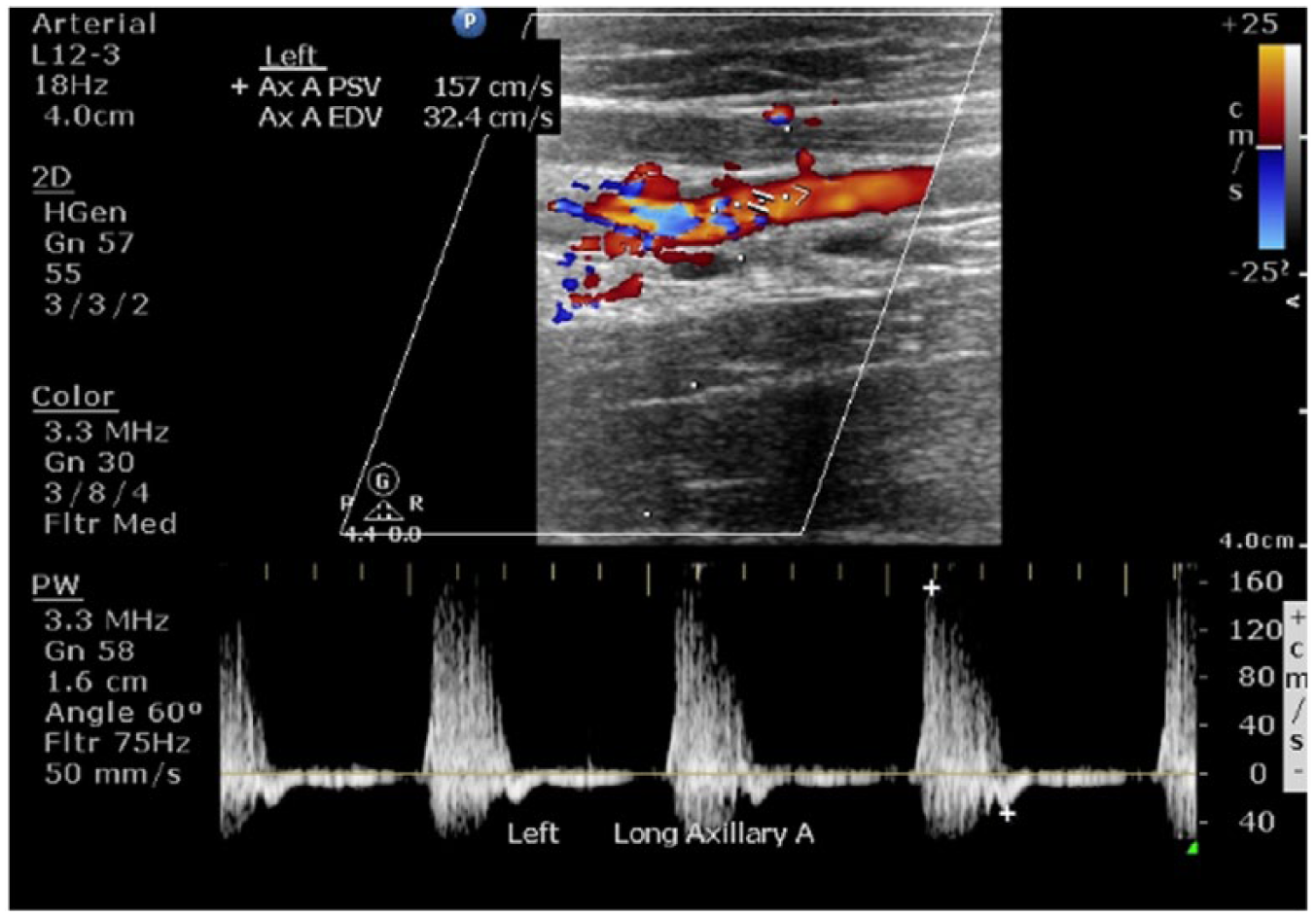
Longitudinal duplex sonogram from patient’s annual upper extremity sonogram 3 years after diagnosis showing the sonographic assessment of the left axillary artery with a PSV measuring 157 cm/s.
One year following, the patient presented to the same sonography department 4 years after her initial diagnosis for her annual follow-up carotid duplex sonogram and bilateral duplex sonogram of the upper extremity arteries. The patient was asymptomatic at the time of the examinations. Although the patient was asymptomatic, it was recommended that she follow-up annually to evaluate for any progression of the disease, since there was a risk of the disease progressing from the subclavian arteries and causing narrowing and possible occlusion in distal arteries. The carotid duplex sonogram was within normal limits. Both the right and left common carotid arteries were patent with no stenosis noted and minimal plaque visualized (Figures 5 and 6). No abnormalities of the internal, external, or common carotid arteries were visualized bilaterally. The bilateral duplex sonogram of the upper extremity arteries again demonstrated normal blood flow in the right and left subclavian arteries as a result of treatment. The right axillary artery demonstrated turbulent flow with a PSV measuring 411 cm/s (Figure 7). The right axillary artery spectral waveform appeared monophasic with the presence of spectral broadening. The right brachial, radial, and ulnar arteries were visualized and appeared within normal limits. The waveforms of the right radial and ulnar arteries appeared triphasic. Sonographic evaluation of the left axillary artery also demonstrated turbulent flow as well as spectral broadening, with a PSV measuring 203 cm/s (Figure 8). The left brachial, radial, and ulnar arteries were visualized and appeared within normal limits. The waveforms of the left radial and ulnar arteries appeared triphasic. The velocities of both axillary arteries had significantly increased when compared with the PSV of the right and left axillary arteries documented 1 year prior (Figures 3 and 4). Based on the respective increases in axillary artery peak systolic velocities and evidence of increasing flow disturbance when compared with the examination performed 1 year prior, the right axillary artery was diagnosed with approximately 70% to 80% stenosis and the left axillary artery was diagnosed with approximately 50% to 69% stenosis. These findings were thought to represent the sequelae of Takayasu’s arteritis.
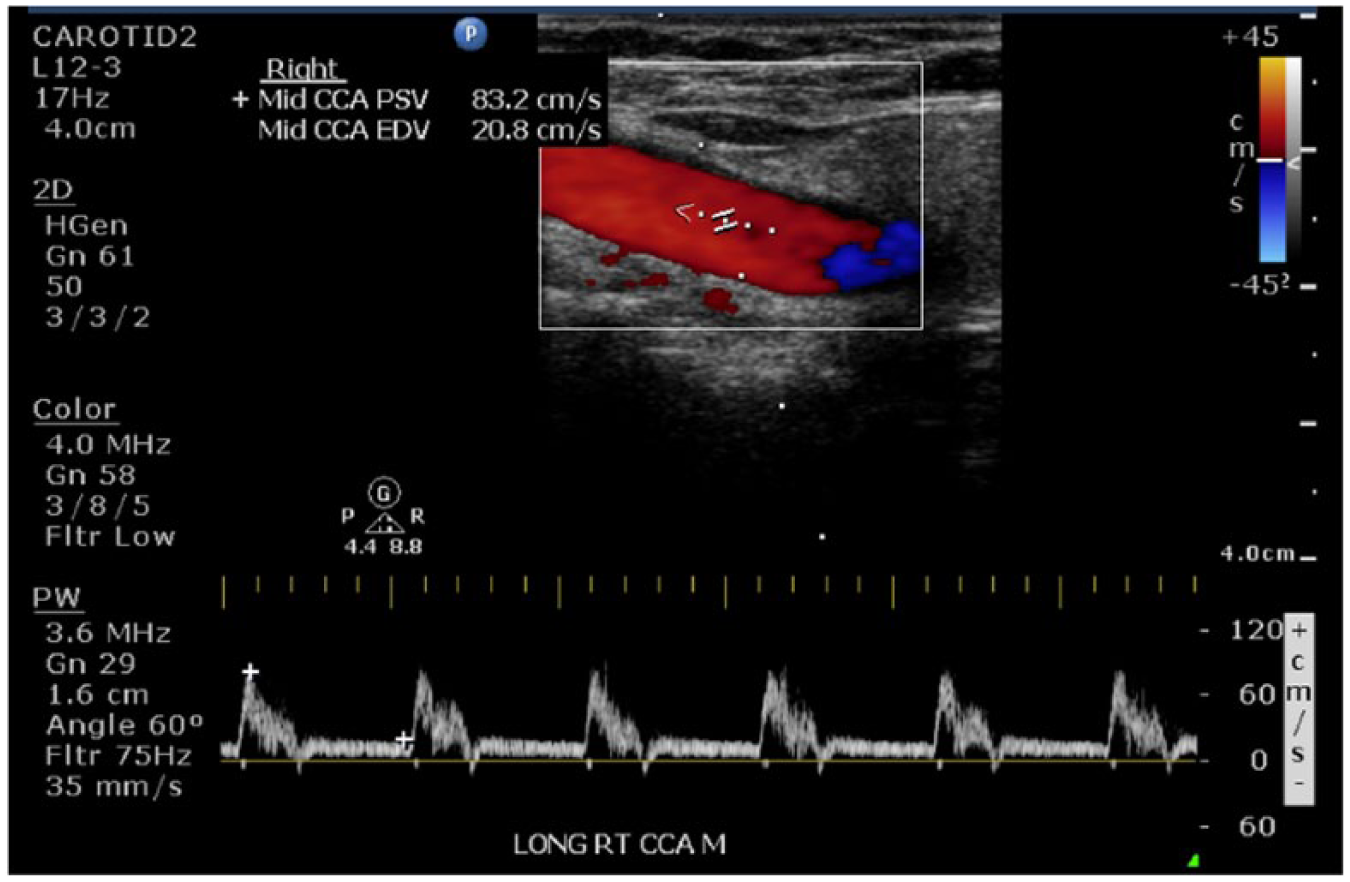
Longitudinal duplex sonogram from patient’s annual carotid sonogram 4 years after diagnosis showing a normal right common carotid artery with a PSV measuring 83 cm/s.
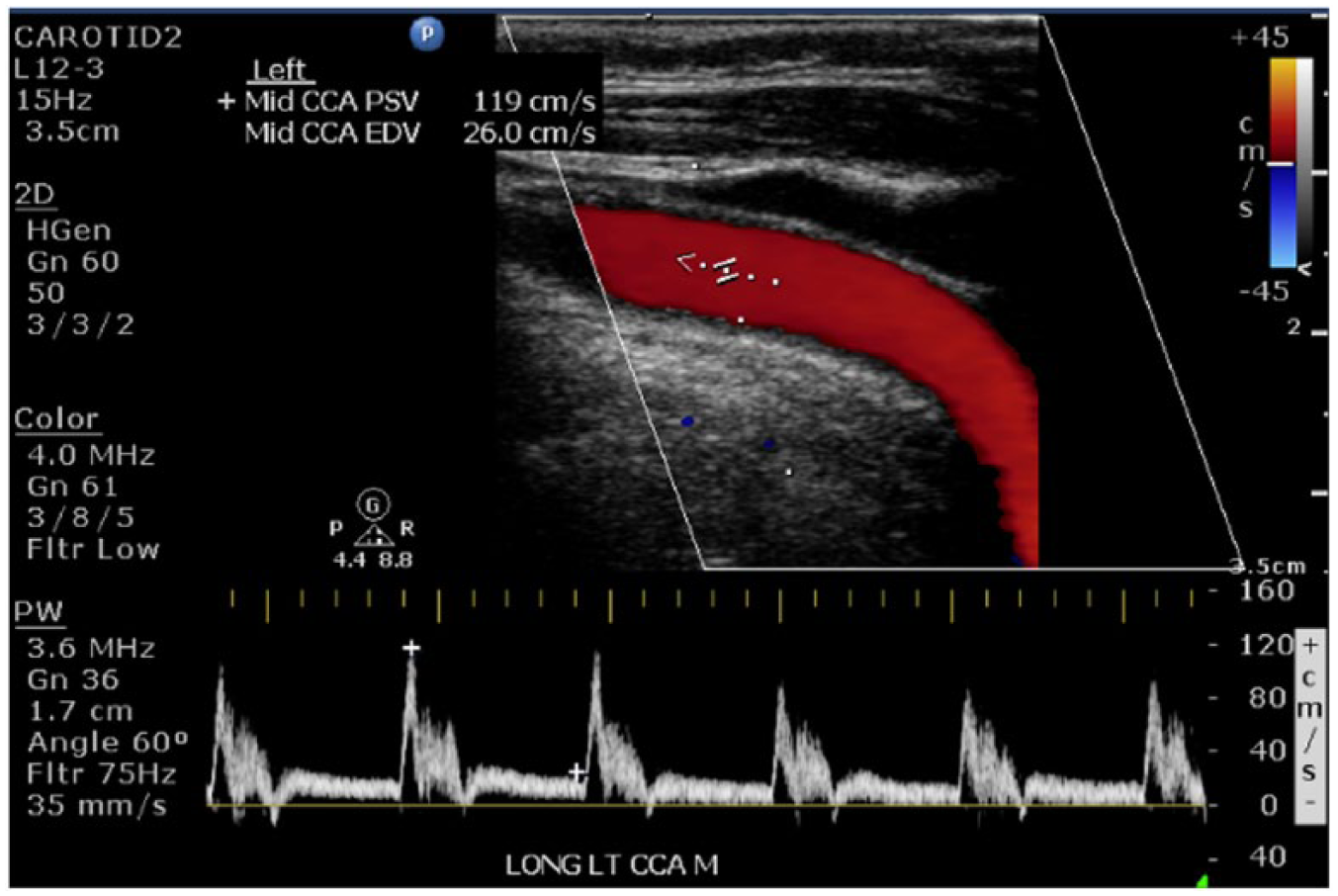
Longitudinal duplex sonogram from patient’s annual carotid sonogram 4 years after diagnosis showing a normal left common carotid artery with a PSV measuring 119 cm/s.
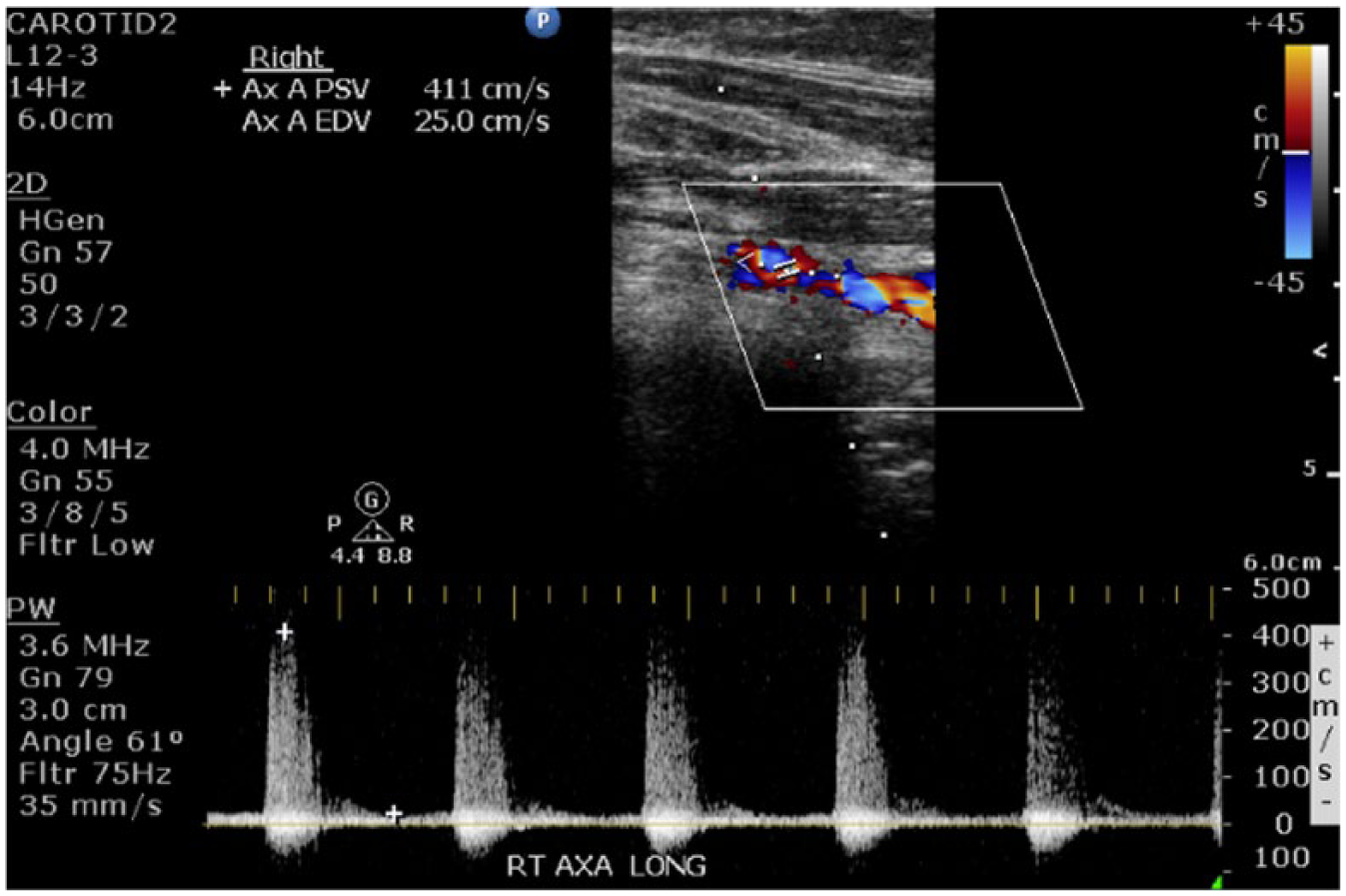
Longitudinal duplex sonogram from patient’s annual upper extremity sonogram 4 years after diagnosis of the right axillary artery showing turbulent flow on color Doppler and presence of stenosis on spectral Doppler, with a PSV measuring 411 cm/s.
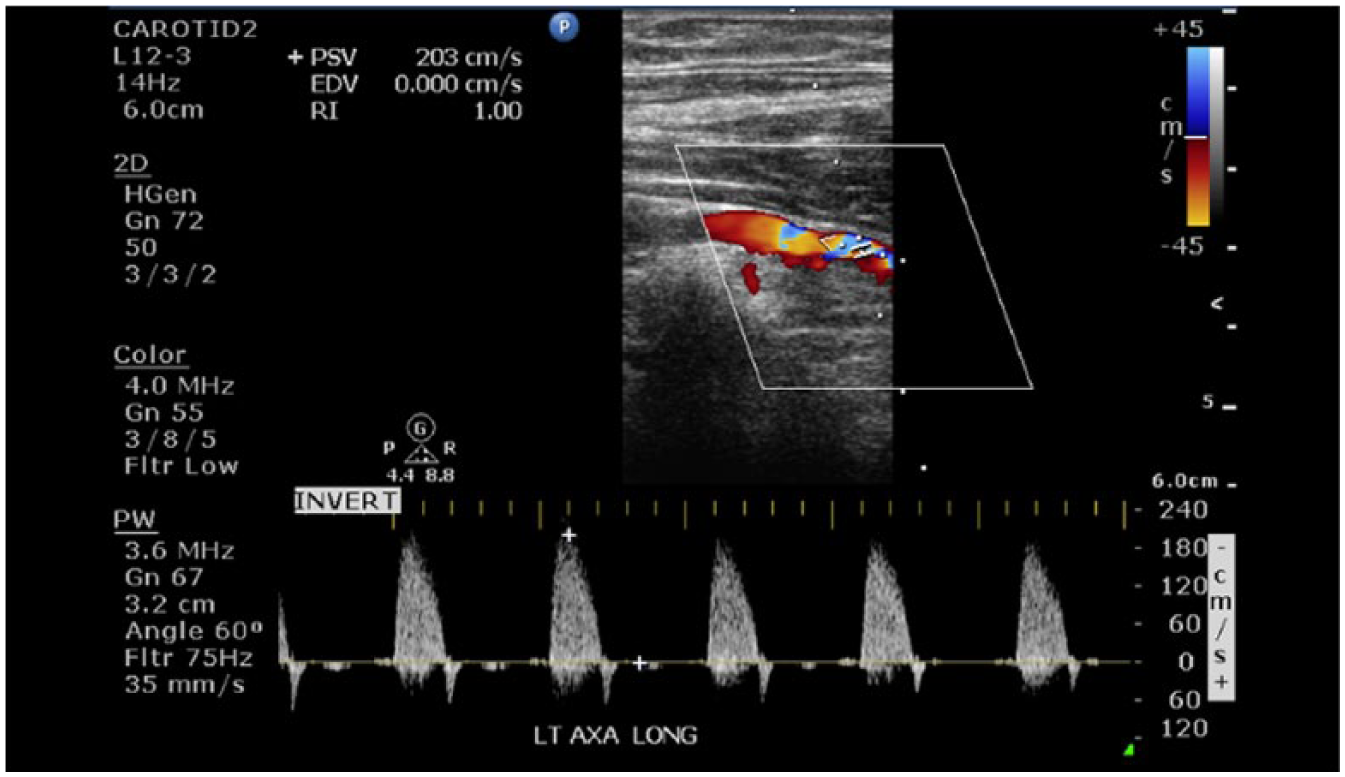
Longitudinal duplex sonogram from patient’s annual upper extremity sonogram 4 years after diagnosis of the left axillary artery showing turbulent flow on color Doppler and presence of stenosis on spectral Doppler, with a PSV measuring 203 cm/s.
Based on the sonographic findings, follow-up with CTA or MRA was recommended to obtain additional details regarding the progression of disease in order to alter the patient’s current treatment plan as appropriate. The patient chose to seek treatment at a different facility; therefore, no further follow-up information was available.
Discussion
Takayasu’s arteritis is a rare nonspecific inflammatory disease of unknown cause predominantly affecting the aorta and its main branches, coronary arteries, and pulmonary arteries of young females. 3 Over time, the inflammation in branches of the aorta results in narrowing and possible occlusion of the main arteries and their branches. Arteries affected by severe stenosis may be narrowed to such an extent that normal arterial pulsations cannot be felt, which is why TA is often referred to as “pulseless disease.” In addition to narrowing and occlusion of the arteries, the patient is also at risk for developing aneurysms as a result of the inflammatory process, which can weaken the arterial wall, causing them to enlarge and become aneurysmal.1,3
Although the etiology of the disease is unknown, the chronic inflammation of the large arteries is thought to be caused by a T-cell–mediated reaction against the components of the vessel walls.3–5 This reaction is an immune response that is produced when T cells attack foreign antigens and secrete lymphokines that initiate the body’s immune response. 6 In most cases, this response is important in defense against pathogens, but for Takayasu’s arteritis, it is an unnecessary response that attributes to inflammatory disease. The annual incidence of TA ranges from 0.4 to 2.6 cases per million in different countries, with the highest prevalence rate reported in Japan. The prevalence of TA in Japan is 40 cases per million, compared with 4.7 to 8.0 cases per million in other countries.7–15 The typical age of onset of TA is the second or third decades of life, and it is nine times more prevalent in females than in males.2,7,16 This case demonstrates a rare, atypical presentation of TA, as the patient is not of Japanese descent and did not show symptoms until shortly before her diagnosis at the age of 66, much later than the typical age of onset.
The most common inflammatory symptoms of the disease include low- or high-grade fever and fatigue. Due to the subtle nature of the symptoms, the disease often goes without diagnosis for a long period of time, or the patient is never properly diagnosed. 3 Other common presentations of TA include limb claudication, contrasting limb blood pressure/pulses, hypertension, and dizziness. 2 The manifestations of TA typically appear in two stages. In the first stage, systemic symptoms including fever, fatigue, weight loss, headaches, myalgia, and arthralgia may present. Months to years later, in the second stage of the disease, vascular-related symptoms associated with ischemia are limb claudication, neurological symptoms, arterial bruits, decreased or absent peripheral pulses, and aneurysmal development. 17
The prevalence of TA in North America is estimated to be 2.6 cases per million annually, but because the disease often remains undiagnosed, this statistic may be underestimated. 18 The implications of TA can be life threatening, as the stenosis, occlusion, or dilation of affected vessels can result in end-organ ischemia, infarction, and dysfunction. For this reason, early diagnosis and proper surveillance of the disease is vital, which is ultimately reliant on clinician awareness of the disease and its consequences. Likewise, effective use of diagnostic tests to detect the disease and determine proper treatment may allow the progression of the disease to be slowed by alleviating the underlying vascular inflammation. 19 The gold standard to identify the narrowing and occlusion of the aorta and its main branches is angiography. The detection of arterial lesions has been immensely improved through the use of CTA and MRA. As of 2014, there have been no reports of biological markers specific to assist in the diagnosis of TA. 1 Positron emission tomography and duplex sonography can be used for surveillance but are not the standard for diagnosing TA. 2 This case confirms this principle, as CTA provided the initial diagnosis, and serial sonographic examination was used to monitor the progression of the disease.
The delayed diagnosis of TA can be attributed to its rarity and possible lack of awareness within the medical community. 18 It has been demonstrated that only 33% of TA patients had legitimate symptoms and that only 20% had fever either at the origination of the disease or in its active stage.19,20 Although the life expectancy of patients with TA is predicted to be low, the prognosis of this disease has been dramatically improved by the introduction of glucocorticosteroids and immunosuppressants. 1 High-dose steroids are typically prescribed to patients presenting with systemic symptoms indicating the presence of inflammation. These symptoms include fever, fatigue, and chest or back pain. Within a few days of treatment, many patients are relieved from systemic symptoms. When steroids are not effective, conventional immunosuppressive agents are added to the glucocorticosteroids. These agents include methotrexate, mycophenolate mofetil, azathioprine, tacrolimus, cyclophosphamide, and others. 3 A study conducted to assess the effectiveness of the medicinal treatment of TA reported that 75% of patients treated with prednisone and methotrexate develop new vascular lesions upon follow-up. 20 Therefore, although medicinal treatment can diminish the initial symptoms and effects of the disease, progression of TA is commonly reported, which demonstrates the need for serial sonographic follow-up evaluation.
Half of patients diagnosed with TA will progress to a stage requiring one or more surgical procedures, despite available medicinal treatment. 2 A study conducted to assess the effectiveness of surgical treatment of TA revealed that restenosis was observed in 13.5% of patients diagnosed with TA in a median time of 11 months after surgery. 20 Since restenosis is common, surgical revascularization should be executed only after careful consideration.
Conclusion
Takayasu’s arteritis is a rare vascular disease affecting major arteries, most commonly in young women. It is accompanied by a variety of nonspecific clinical symptoms that often make it difficult to diagnose in its early stages. This case report demonstrates a rare, atypical case of TA that was diagnosed in an older woman and validates the effectiveness of sonography in the surveillance of the disease. The prompt sonographic detection of vascular changes associated with the progression of TA is important and potentially alters treatment and prognosis. Therefore, increased sonographer awareness of TA has the potential to improve diagnostic confidence and accuracy in this rare, potentially life-threatening disease.
Footnotes
Acknowledgements
The authors thank Ashley Wibbenmeyer, RDMS, Cathy Wichert, RDMS, RVT, and Jessica Deneke, RT(R), for their guidance and assistance in obtaining information for this case report.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial assistance for the research, authorship, and/or publication of this article.