
Abstract
The most common acute abdominal disorder in the pediatric population appears as a telescoping of the bowel, resulting in either intermittent or complete obstruction. Intussusceptions transpire as the bowel prolapses into a more distal bowel segment and is propelled forward. A case is presented of multiple small bowel intussusceptions, pneumatosis, intraperitoneal fluid, and pericardial effusion. Sonography initially visualized the obstructions, along with multiple other indicators of an abdominal disorder. The use of computed tomography followed to provide a more comprehensive view of the child’s abdomen. Each imaging technique revealed new aspects of the abdominal disorder and concluded in the diagnosis of celiac disease. This case supports the idea that small bowel intussusceptions should not be disregarded as insignificant incidental findings but rather should alert sonographers to further investigate for evidence of celiac disease.
Intussusception occurs when the bowel telescopes upon itself, causing an intermittent or complete obstruction. Although the cause is nonspecific, most intussusceptions are associated with an antecedent upper respiratory tract infection or inflammation of lymphoid tissue near the ileocolic region. 1 While 90% of intussusception cases involve the ileum folding into the cecum at the ileocecal valve, it is also possible to have an ileoileal obstruction or an intussusception located exclusively within the colon. 1 Each type often presents in a similar clinical manifestation, including failure to thrive, abdominal distention, gastrointestinal bleeding, diarrhea, or nonspecific abdominal pain. 2 A significant 80% of intussusception cases transpire before the age of two years. 3 Sonography is the imaging modality of choice in the detection of intussusception due to its sensitivity and specificity. For prevention of recurrence, the lead point and type of intussusception should be investigated. Lead points can vary from gastrointestinal abnormalities to systemic pathologies, including celiac disease. Many small bowel intussusceptions are often ignored as unremarkable, but they can be indicators of other processes like celiac disease. 4 Sonography should be considered beneficial in the process of recognition and documentation of such incidental findings. Left undiagnosed and untreated, celiac disease creates irritation and inflammation within the bowel mesentery that can prompt obstruction in the form of intussusceptions. 4 The correlation between celiac disease and small bowel intussusception is a relatively new concept that has been rarely reported in the literature, yet it can be highly advantageous for the patient in respect to timely relief. Due to the benefits from a quick diagnosis, it is crucial that sonographers are aware of this connection to know when to look for signs of the linked pathology. 4 Recognizing small bowel intussusception as a possible prompt to investigate for evidence of celiac disease could support an earlier diagnosis. It not only could prevent future bowel obstructions but also improve the patient’s quality of care.
Case Report
A 1-year-old Caucasian girl presented to the sonography department for a complete abdominal sonogram. The patient’s mother and maternal grandmother reported noticing abdominal distention and diarrhea for the prior month. The family also noticed an increase in crying fits, which they attributed to teething pain. There was no laboratory work or previous imaging completed. Sonography was performed using a GE Logiq E9 (GE Healthcare, Pasadena, CA) with a 9-MHz curvilinear array transducer.
The abdominal ultrasound revealed three separate small bowel intussusceptions suspected to be obstructing intermittently. One was in the periumbilical region, with a transverse diameter of 1.6 cm; the next was in the left lower quadrant, with a transverse diameter of 1.8 cm (Figure 1); and the third was found in the right lower quadrant, with a transverse diameter of 1.8 cm (Figure 2). The sonogram also showed segments of bowel wall thickening, with pneumatosis of the bowel wall both within and without the intussusceptions (Figure 3). Intraperitoneal fluid was located in the right and left upper quadrants and the cul-de-sac. A small pericardial effusion was noted (Figure 4). The liver appeared normal in size and echotexture, measuring 8 cm in length. The bile duct, gallbladder, pancreas, and kidneys all appeared within normal limits for the patient’s age.
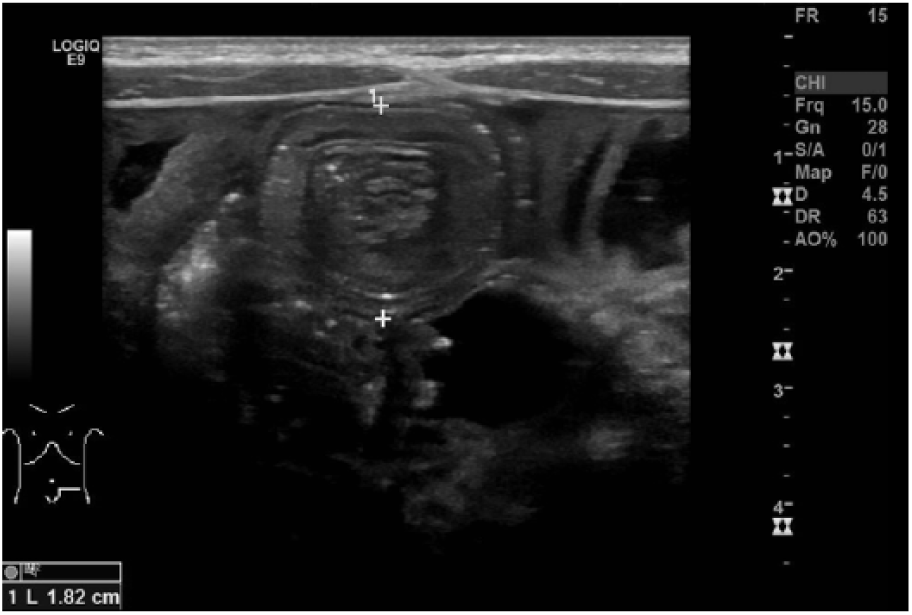
This is a transverse gray-scale sonographic image of the left lower quadrant demonstrating an intussusception measuring 1.82 cm in anterior-to-posterior diameter.
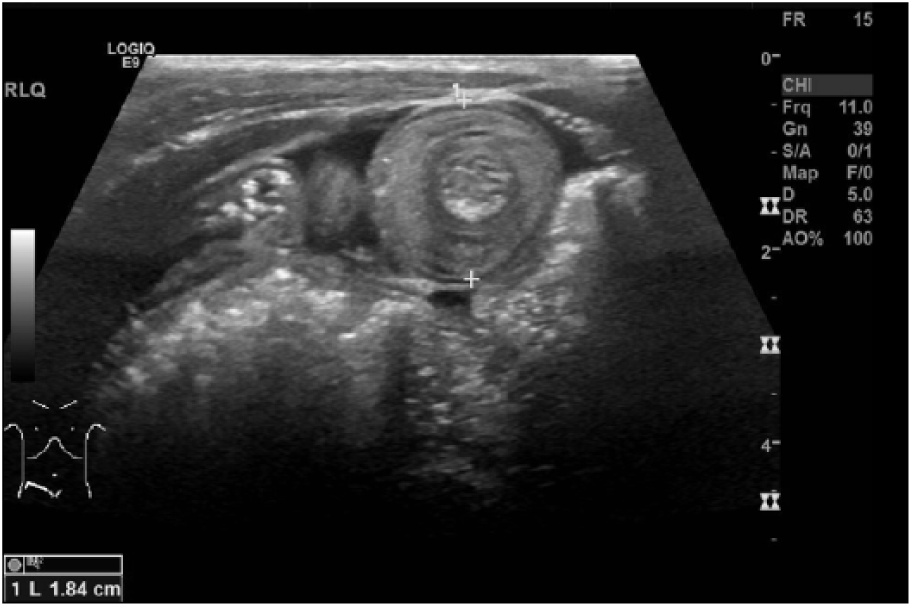
This is a transverse gray-scale sonographic image of the right lower quadrant demonstrating an intussusception measuring 1.84 cm in anterior-to-posterior diameter.
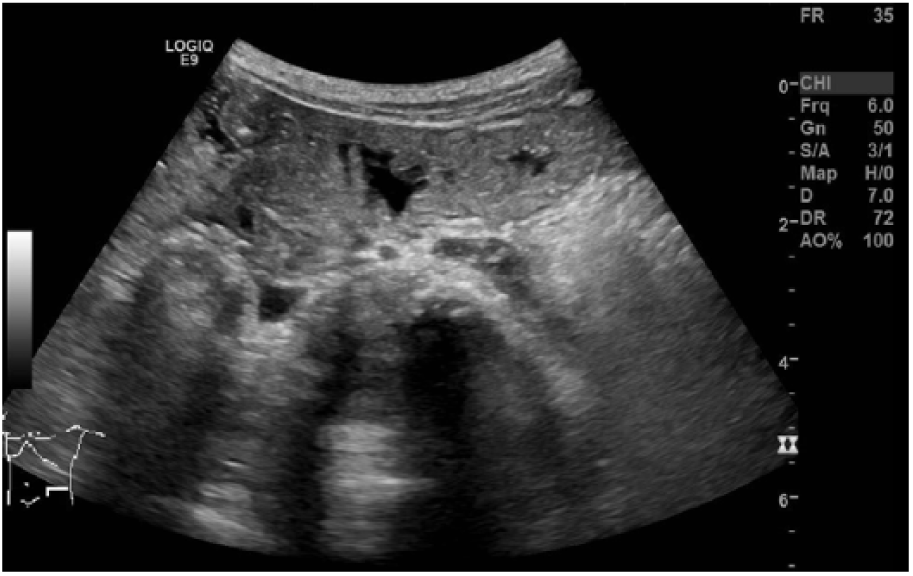
This is a transverse gray-scale sonographic image of the left lower quadrant demonstrating pneumatosis and small bowel wall thickening. (Orange indicates pneumatosis; blue arrow indicates bowel wall thickening.)
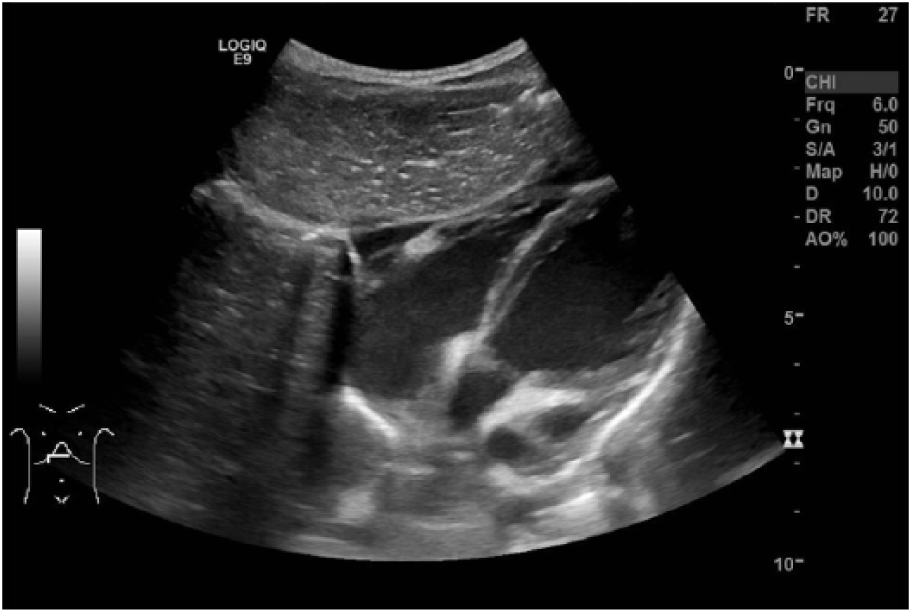
This is a transverse gray-scale sonographic image of the epigastric region demonstrating a pericardial effusion indicated by the arrow.
The abnormal findings in the sonogram prompted a computed tomogram (CT) of the abdomen and pelvis with and without contrast, to be completed later in the day. The CT findings displayed soft tissue densities surrounding the superior mesenteric vessels (Figure 5), which raised concern for an infiltrative process such as lymphoma or leukemia. The CT corroborated the sonographic findings of the intussusceptions, bowel wall thickening, pneumatosis, and pericardial effusion. Due to the additional pathology surrounding the intussusceptions, a pathologic connection was suspected but unknown. To further investigate the etiology of the intussusceptions, the patient was referred to the hematology and oncology departments in speculation of the soft tissue densities around the superior mesenteric vessels. There, the patient underwent a magnetic resonance imaging (MRI) and positron emission tomogram (PET), which concluded the absence of a malignancy. Laboratory tests were drawn as a concern for an adrenal mass; homovanillic acid (HVA) was within normal limits, and vanillymandelic acid (VMA) was slightly elevated. Both HVA and VMA are tested from a urine specimen to screen for catecholamine-secreting tumors, such as neuroblastoma, pheochromocytoma, and other neural crest tumors. 4 While the HVA level was normal, the VMA elevation was of uncertain clinical significance because levels are known to fluctuate with dietary intake. Due to the nature of the intussusceptions, originating in the small bowel, they reduced spontaneously hours after the patient’s first CT, which was deduced by their absence on the MRI. Based on the laboratory and imaging findings, the hematologists determined that the cause of the intussusceptions and associated abdominal abnormalities was celiac disease. In response to this diagnosis, the patient’s caregivers were advised to place her on a gluten-free dietary plan. For follow-up treatment, the hematologists recommended repeat urine HVA/VMA in one month and CT with contrast in two months to more accurately evaluate the superior mesenteric vessels along with the bowel. Despite the recommendations, the patient did not return for her appointments, and there is concern about parental compliance with the treatment plan.
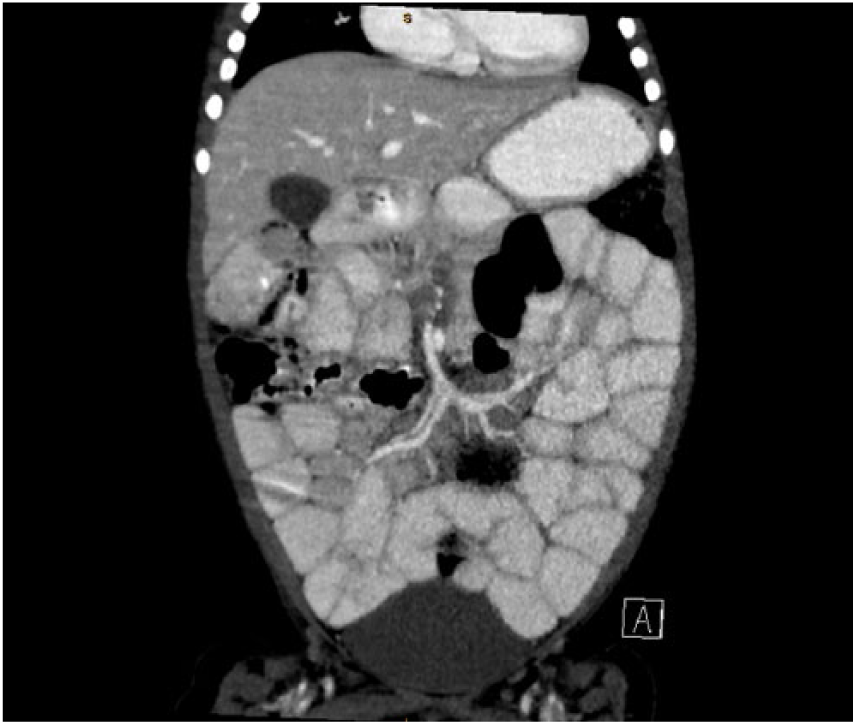
A coronal computed tomography image demonstrating soft tissue densities surrounding the superior mesenteric artery and superior mesenteric vein, indicated by the arrows.
Discussion
This case demonstrates the connection between celiac disease, a systemic abdominal condition, and small bowel intussusception, a condition often thought to be clinically insignificant. The inflammatory changes in the bowel wall associated with celiac disease act as precursor to forming intussuceptions.2,4 Although these findings are often transient, they still have an underlying cause that can indicate pathology, which should be investigated. Intussusception is a bowel obstruction created by a portion of the bowel wall prolapsing into a distal segment of the bowel. The pediatric population is most commonly affected by this process and often presents with abdominal distention, pain, vomiting, and bloody stools. 3 In cases of intussusception involving either small or large bowel, the occlusion of the bowel passageway has damaging repercussions. In addition, this could result in an inability of semifluid partially digested food and digestive secretions (chyme) to pass through the intestines, resulting in possible bowel ischemia if an intervention is not provided. The accurate classification of intussusception is crucial to diagnose so that the proper treatment can take place. If the intussusception is ileocolic, therapeutic reduction by a fluoroscopy air contrast enema is the most common plan of treatment. Failure to reduce the obstruction requires surgical intervention. 1 Due to the nature of the obstruction, immediate attention is necessary to negate the potential for intestinal necrosis, which increases the risk of severe complications and possible fatality. Idiopathic small bowel intussusceptions are more common than ileocolic intussusceptions and have the ability to resolve on their own, making them considerably less emergent. These cases are often caused by benign lymph node hyperplasia, abnormal bowel wall motility, bowel wall thickening, or impaction of secretions. 1 Underlying gastrointestinal abnormalities or discrete precursors that could lead to small bowel intussusceptions are often visualized with CT or MRI due to their ability to penetrate the bowel gas and create a global anatomical image. Visualization of these often transient abnormalities by sonography is dependent on their detection and documentation by the sonographer. Diagnostic precursors include pathologies such as Meckel diverticulum, duplication cyst, cystic fibrosis, or celiac disease. 2 Although intussusceptions are generally found in children ages six months to years years, children approximately three to eight years old with Henoch-Schonlein purpura (HSP) also have an increased risk of developing these intestinal obstructions, proving to be another cause. 1 HSP is an autoimmune disease that is the most common form of vasculitis in children. 1 Affecting 8 to 20 children per 100,000 annually, HSP has symptoms involving the skin, joints, intestines and kidneys. 5 The inflammation formed within vessel walls has the ability to create focal lead points for intussusceptions and further complicate HSP. 5
Sonography displays changes in the bowel wall, peristalsis, and vascular perfusion, deeming it an efficient imaging modality for evaluating intussusceptions. These unique small bowel obstructions often measure less than 3 cm anterior to posterior (AP) in the transverse plane, displaying the layers of bowel wall telescoped within each other. 1 The sonographic appearance of intussusception is described as a target or pseudo-kidney sign, causing the obstruction to stand out from the adjacent normal bowel. The sonolucent outer ring represents the edematous enfolded loop of the intussusceptum, with the echogenic central area representing the compressed mucosa. 1 Any other visualized rings within the obstruction are believed to be additional bowel wall layers condensed upon each other. Other commonly imaged structures can be dilated loops of obstructed proximal bowel or free peritoneal fluid. 1 When conducting a sonographic examination on a suspected area of intussusception, color and power Doppler should be used to indicate possible regions of bowel ischemia. 6 If bowel ischemia is present, areas of decreased blood flow should be demonstrated. Power Doppler is used to guarantee the absence of blood flow as it has an increased sensitivity to slow flow compared to color Doppler.
Pneumatosis intestinalis (PI), or air in the bowel wall, commonly occurs in conjunction with intussuception. 5 The inflammation and constriction of the bowel wall associated with intussusceptions cause the accumulation of intramural gas that is benign to the bowel. When the bowel wall is visualized, PI appears sonographically as echogenic foci within the bowel wall. Clinically, PI is associated with nausea, vomiting, and abdominal pain. PI is not considered a surgical emergency unless coexisting ischemia or perforation has occurred. 7 In addition to the intramural gas, bowel wall thickening is often visualized simultaneously with intussusceptions due to inflammation and irritation from the occluded bowel lumen. Abdominal inflammation is rarely limited to one area and can be caused by the development of systemic abdominal disease. As demonstrated in this case, celiac disease is one of various pediatric abdominal diseases that have been linked to intussusceptions, particularly those located within the small bowel.
Celiac disease is a chronic inflammatory autoimmune disease of the small intestine, produced by an intolerance to gluten products. This intolerance causes an increased susceptibility to damage of the small bowel mucosa and produces clinical symptoms such as diarrhea, iron-deficiency anemia, and dyspepsia. 8 While celiac disease exists in approximately 1% of the global population, half of affected people do not show the classic gastrointestinal symptoms and go undiagnosed. 9 Celiac disease is most commonly diagnosed through blood work, yet with the increased awareness of its correlation to small bowel intussusceptions, sonography could become a new tool in the diagnostic process. Other diagnostic modalities have also been deemed useful for evaluating atrophy of the bowel wall often marked by celiac disease. These include capsule endoscopy, CT enterography, and MRI enterography or enteroclysis. 10 Despite the limitations of sonography due to bowel gas, it has also been used to image correlated findings present in this abdominal disorder. In patients with celiac disease, free abdominal fluid, increased peristalsis, and pericardial effusions have been observed. 8 Other studies describe enlarged mesenteric lymph nodes, increased bowel wall thickness, small bowel dilatation, and an increased intraluminal fluid content present in celiac patients. 8 Interestingly, these same associated findings can be observed in small bowel intussusceptions. Despite this association, there is a deficiency in the literature regarding the use of sonography to evaluate for celiac disease in pediatric patients who present with intussusception symptoms. There is also a deficiency in the recognition of small bowel intussusceptions as a reason to further investigate the abdomen. Small bowel obstructions are often regarded as transient findings with little clinical significance. Meanwhile, small bowel intussusceptions can be an indication of celiac disease and therefore should no longer be ignored. 2
Due to the lack of early diagnosis early and the prevalence of gluten in the normal diet, intussusceptions are far more common among children with undiagnosed celiac disease. 4 The classic symptoms of celiac disease generally begin between 6 and 18 months of age when the child is generally introduced to foods containing prolamines. 9 Celiac disease is associated with symptoms that are comparable to those found with intussusceptions due to the similar irritation and disruption they cause to the bowel. These include impaired growth, chronic diarrhea, abdominal distention, and unhappy behavior. 11 While intussusceptions are often seen in the pediatric population, the root cause of celiac disease may go undiagnosed, which causes prolonged symptoms until the child’s diet is changed. The average time it takes to diagnose celiac disease in both children and adults is 3 to 11 years in the United States. 12 Sonographers can play a key role in improving this rate by addressing the possible gastrointestinal disorder when more obvious conditions, such as intussusception, arise in patients. Upon recognition of an intussusception, the sonographer should examine the bowel further to look for common sonographic indications of celiac disease, such as thickened bowel wall in areas not involved in the intussusception, mesenteric lymphadenopathy, and free peritoneal fluid. 8 This would provide more information about the bowel to support suspicion of systemic abdominal disease and prompt further workup to define the underlying diagnosis. Despite the desire to diagnose celiac disease as early as possible, this disorder can also manifest in middle-aged adults. The two most common peaks in incidence of presentation are in childhood and in the fourth and fifth decades of life, specifically between 46 and 48 years.9,13 Similarly, intussusceptions are not limited to the pediatric population and can also cause similar symptoms in adults. Intussusception is rare in adults but is associated with the symptom of abdominal pain (78% of cases 14 ) or as an incidental finding (22% of cases 14 ). Interestingly, in a 2016 article from the World Journal of Gastrointestinal Surgery, intussusception was described as the initial manifestation of celiac disease in 57% of cases in American adults. 7
In patients of any age who exhibit this association of pathologies, various treatment options are available. In the presence of an ileoileum intussusception, early reduction by an image-guided enema (either air or a water-soluble contrast) may be indicated to prevent bowel infarction. 2 However, not all cases of intussusception must be immediately reduced as some small bowel occlusions can resolve on their own within minutes of detection. If the intussusception does not spontaneously resolve during the ultrasound examination, some researchers suggest a repeat sonographic examination within 45 minutes. 2 Another way to determine the necessary treatment plan is to evaluate the measurement of the bowel occlusion. If the intussusception measures larger than 3.5 cm in the anterior-to-posterior dimension, it is more likely to require intervention by enema or laparoscopic surgery. Conversely, if the intussusception measures less than 3.5 cm in the anterior-to-posterior dimension, it is likely to resolve spontaneously. 2 No matter the path of resolution, it is crucial to determine the cause or lead point to prevent more intussusceptions from occurring.
The management of celiac disease is usually consistent among all patients. A lifelong commitment to a gluten-free diet (GFD) is the most immediate change. Some patients also experience an associated lactase deficiency secondary to damage to surface epithelial cells, so it is recommended to avoid dairy products as well. 9 While the body adjusts to a GFD, patients are suggested to take a gluten-free multivitamin to combat the vitamin B deficiency often associated with GFD. Alternative treatment options include a gluten-degrading enzyme, ingested orally, that accelerates gluten digestion in the gastrointestinal tract. 9 Although managing celiac disease requires a significant lifestyle adjustment, patients can live healthy, productive lives despite the condition.
Conclusion
Celiac disease continues to disrupt the lives of both pediatric and adult populations. Due to celiac disease’s systemic abdominal presence, the likelihood of secondary pathologic processes occurring increases. As presented in this case, intussusceptions can be seen in the presence of celiac disease. Therefore, sonographers should be informed about the appearance of intussusception and associated processes like celiac disease. Sonography plays a vital role in detecting intussusception and is used due to its improved technology, portability, cost-effectiveness, and lack of ionizing radiation. Sonography allows the sonographer to evaluate common signs of intussusception such as the target sign of the bowel wall, free peritoneal fluid, and decreased vascular perfusion. 1 Sonography can also evaluate key features of celiac disease, including increased bowel wall thickness, free peritoneal fluid, and enlarged mesenteric lymph nodes. 8 If a small bowel intussusception is visualized during an abdominal sonogram, and an immediate lead point such as Meckel diverticulum, cystic fibrosis, or a polyp is not detected, celiac disease should be a differential consideration to implement more comprehensive patient care. 2 Sonographers can play a role in the early diagnosis of celiac disease by recognizing the association between small bowel intussusception and celiac disease, prompting a thorough examination of the bowel for further findings that support the consideration of celiac disease as an underlying cause of the intussusception.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.