
Abstract
Small bowel obstruction (SBO) secondary to intussusception of Meckel’s diverticulum (MD) is a rare cause of acute abdominal pain that may warrant urgent surgical treatment. Volvulus or intussusception of the small bowel with presence of MD as the lead point is the most commonly reported etiology of Meckel’s related obstructions. We report an interesting case of a small bowel obstruction caused by the intussusception of an MD within its own lumen. The case involves a 30-year-old male who presented to the emergency room with acute, severe abdominal pain with an abdominal computed tomography (CT) showing a distal high-grade SBO. Decision was made to take the patient to the operating room urgently due to his clinical examination and radiologic imaging, specifically CT scan. Diagnostic laparoscopy was performed and subsequently converted to an exploratory laparotomy, which revealed the intussuscepted MD with focal necrosis into the distal small bowel causing an SBO. A segmental small bowel resection with hand sewn primary anastomosis was performed. The case presents an interesting challenge in deciding when to take a patient with an SBO to the operating room versus initial conservative management and what the treatment should be if an MD is encountered. In addition, the case emphasizes the importance of history and physical exam findings in coordination with radiologic imaging in helping to make appropriate decisions in a timely manner for operative vs conservative management of an SBO. It reminds us that, Meckel’s diverticulum, although less commonly the cause of a small bowel obstruction in the adult population, needs to be on the differential diagnosis and we need to have a high clinical suspicion for this possibility to ensure appropriate treatment in a timely manner.
Introduction
Meckel’s diverticulum (MD), a persistent remnant of the omphalomesenteric duct, is the most common congenital anomaly of the small bowel. 1 MD was originally described in 1598 by Fabricius Hildanus, but was ultimately named after Johann Friedrich Meckel, who established its embryonic origin in 1809. 2 The remnant most commonly occurs on the antimesenteric border of the ileum and is characterized as a true diverticulum, containing all layers of the bowel wall. The estimated prevalence in the general population is approximately 2%, with a male:female predominance of 2:1. The vast majority of MD are asymptomatic. Studies have reported the incidence of symptomatic MD to be approximately 16% over the course of a lifetime, with most complications arising by 2 years of age. 2 MD most often include one of two types of ectopic tissues, gastric (71%) or pancreatic (12%). 3 Symptomatic patients commonly present with gastrointestinal bleeding from small bowel ulcerations due to ectopic gastric acid secretion within the MD, diffuse abdominal pain from inflammation, or intestinal obstruction from volvulus or intussusception of the small bowel with MD as the lead point. Other mechanisms of Meckel’s-related obstructions are torsion, herniation (Littre’s hernia), inflammation, or inversion of the MDs. Although the literature does report cases of all the above as causes of small bowel obstructions (SBO) due to MD, these cases are infrequent, making it important to have a high suspicion when presented with a patient with a small bowel obstruction. There are a few case reports of SBO secondary to intussusception of MD reported within the last decade, all of which occurred in the 20–35 age range and all posed a diagnostic dilemma on initial presentation due to unclear etiology of SBO. 14 We present an interesting case report of a small bowel obstruction caused by intussusception of an MD with operative management.
Case report
A 30-year-old male with significant history of an uneventful open left inguinal hernia repair at 8 years old presented to the emergency room with severe, persistent abdominal pain for 12 hours. The patient reported nausea and 10 episodes of non-blood stained, non-bilious vomiting since waking from the pain, with associated obstipation. Last flatus or bowel movement was reported to be 1 day prior. His physical examination was notable for diffuse abdominal tenderness and mild distention. In regard to his previous inguinal hernia surgery, he had a very small well healed barely visible scar in the left lower quadrant of his abdomen without any acute skin changes or evidence of inguinal hernia. Vitals and laboratory tests were unremarkable on presentation. Chest and abdominal XR’s were performed which showed dilated loops of small bowel without evidence of free air or lung pathology. These findings were nonspecific for a direct cause of the dilated loops of bowel and additional imaging was warrented. Computed tomography (CT) imaging showed a distal high-grade SBO with multiple dilated loops of small bowel throughout the abdomen measuring up to 3.5 cm in diameter. There was also mild ascites seen in the right lower quadrant and pelvis, along with a lucency within a distended loop of small bowel in the medial right pelvis that was unable to be fully characterized (Figure 1). On re-examination of the patient, he continued to have persistent diffuse abdominal pain with voluntary guarding and rebound, which was new from previous examination. Patient was scheduled for urgent surgical intervention after initial management in the emergency room with intravenous fluid resuscitation and nasogastric tube placement demonstrated minimal improvement in symptoms along with worsening abdominal examination. At this time, our working diagnosis was an SBO, concerning for a possible closed loop obstruction.
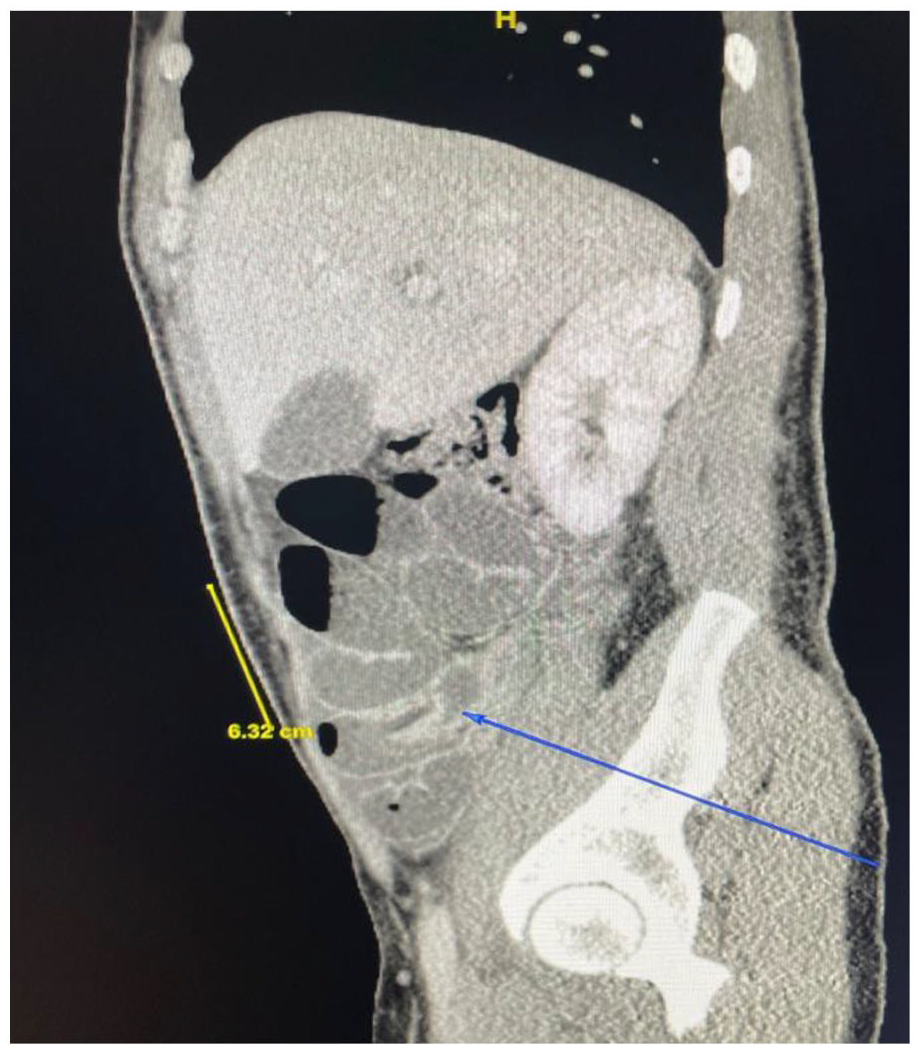
CT imaging with distal high-grade SBO with multiple dilated loops of small bowel throughout the abdomen measuring up to 3.5 cm in diameter. There is mild ascites seen in the right lower quadrant and within the pelvis along with a lucency within the distended loop of the small bowel in the medial right pelvis that was unable to be fully characterized, which is demonstrated by the blue arrow above.
Patient was taken to the operating room, preoperative prophylactic antibiotics were given and diagnostic laparoscopy was performed, which revealed mucoid ascites throughout the abdomen and what appeared to be an area of intussusception in the right lower quadrant. Efforts to mobilize or reduce the intussusception were unsuccessful, and the decision was made to convert to an exploratory laparotomy. A midline laparotomy incision was made and upon entering the abdomen dilated loops of small bowel were noted and carefully traced to the apparent intussusception in the terminal ileum. On reduction of the intussuscepted bowel, there was a very large diverticulum with necrotic terminal end (Figure 2). An intussuscepted, focally necrotic Meckel’s diverticulum in the distal ileum was identified to be the cause of the acute SBO (Figure 3). A segmental small bowel resection with hand sewn primary anastomosis was performed. The segmental resection with the MD is shown in Figure 4 for reference. The patient tolerated the procedure well and discharged home on postoperative day 4. At follow-up in the office 2 weeks later, we reviewed his pathology, which noted a segment of small bowel containing Meckel’s diverticulum remarkable for pancreatic acinar tissue and the patient reported doing well with return to baseline activity.

Invagination of MD into adjacent small bowel prior to reduction.

Reduced MD with focal necrotic region and hemorrhagic edema.

Segmental resection of small bowel including MD.
Discussion
It is estimated that close to 350,000 patients per year in the United States will present to the hospital with an SBO. 4 Most commonly in the United States, SBOs will be caused by adhesions from previous surgeries, followed by hernias, neoplasms, or inflammatory bowel disease. Cardinal symptoms of patients presenting with SBO are described as abdominal pain, nausea/vomiting and constipation. 5 According to a retrospective study examining the cardinal features of SBOs, they were found to have a low sensitivity and specificity, but relatively high positive predictive value (PPV). 5 Due to this analysis, it may not be sufficient to make clinical determinants for treatment based on symptoms alone and therefore adjunct tests may help to determine management. In addition, these findings help to establish the importance of looking at the whole patient at the time of presentation and not delaying decision making as this study also found the morbidity was 13.8% and mortality was 3.4% in the studied population of all cause SBO patients presenting to a hospital setting with cardinal symptoms. 5 Here we present a case of a small bowel obstruction caused by the intussusception of a Meckel’s diverticulum in a young male with minimal medical or surgical history. Adult intussusception represents approximately 1% of all SBOs, and it is estimated that only 1%–4% of those intussusceptions that present as an intestinal obstruction are due to a Meckel’s diverticulum. 6 Despite this less common etiology of an SBO, it is important to entertain the possibility of this diagnosis, especially in the adult population. In addition, it is important to consider the presentation of MD in general when determining an appropriate differential diagnosis and treatment plan for a patient presenting with signs and symptoms of an SBO.
Meckel’s diverticula are characteristically found approximately 2 feet from the ileocecal valve, but can occur anywhere along the midgut. 3 Painless gastrointestinal (GI) bleeding is the most common presentation due to the greater predominance for ectopic gastric tissues within the MD; however, this is not always the case. Our patient was found to have pancreatic acinar tissue within his MD. Although less frequently found in MD, it is not surprising to find pancreatic tissue in the intestinal tract due to the close proximity of the embryonic pancreatic buds and the foregut during development. It is estimated that 70%–90% of ectopic pancreas occurs in the upper gastrointestinal system, which does support the finding of ectopic pancreatic tissue in an MD. 7 In the general population, diagnosis of an MD with ectopic pancreatic tissue is a difficult diagnosis and a presentation of GI bleeding without cause is usually the reason for workup and eventual diagnosis, but is not the only presentation written about in literature and obstructive symptoms have been reported. Our patient did not present with GI bleeding, but instead with obstructive symptoms. He had one abdominal surgery as a child for an open left sided inguinal hernia, but otherwise did not have significant abdominal pathology to report. It is important to note that most MD presenting without the classical symptom of painless GI bleeding are found incidentally and once found, the most important question that needs to be addressed is what is the appropriate treatment. There is no literature to support any difference in management based on the ectopic tissue type found in an MD to alter management.
Our patient presented with an SBO with signs of focal peritonitis and without clinical improvement after resuscitation. At the time of presentation, there was no clear evidence of an MD, but there was radiographic imaging of intussusception, most likely being contributory to the clinical symptoms. The decision was made to operate without a clear and specific diagnosis of the cause at that time, but due to the clinical examination of the patient, including focal peritonitis, in conjunction with workup. Initially, the case was started laparoscopic as the patient was hemodynamically stable to undergo laparoscopic surgery and without specific reason to limit tolerance of pneumoperitoneum. There was significant dilated bowels within the abdomen, which made exploration and mobilization difficulty. Ultimately, the decision was made to open and perform an exploratory laparotomy due to inability to appropriately mobilize the intussuscepted bowel, which produced a clear cause of the obstruction. The question then was to determine what was the best management and treatment of MD once diagnosed.
It has been argued that reduction of an intussuscepted bowel itself may be adequate in treating intussusception as long as the tissue is viable, and it can be determined that the cause of the intussusception or lead point is benign. 8 Whether this is done clinically, by frozen or by permanent section was not discussed in literature and this is not described as the standard approach in practice. In most literature, the accepted treatment modality for an MD is diverticulectomy or segmental resection, as the risk of recurrence remains significant after reduction alone. 9 We chose to perform a segmental resection for multiple reasons. Our patient had a focal area of necrosis within the intussuscepted bowel, which required removal. In addition, the identified diverticulum was large, warranting a cumbersome diverticulectomy with a large opening into the bowel. The large opening would have required additional closure either hand sewn or stapled and would have had the potential for an increased risk of stricture formation. There are mixed reviews on a standard of treatment for MDs; however, both diverticulectomy and segmental resection appear to be safe treatment modalities with high patient tolerance.9,10
The role of radiologic imaging in the management of patients who present with acute abdominal pain and are subsequently diagnosed with an SBO is an additional topic to be discussed in this case. Our patient had a CT scan demonstrating a high-grade distal SBO, dilated distal bowel loops up to 3.5 cm and ascites in the pelvis. The CT scan itself was critically examined, but it was the patient’s clinical examination and history in coordination with the CT scan that prompted urgent operative intervention. This prompts the question of the reliability of CT scans for the diagnosis of SBOs and their usefulness in determining surgical intervention needs. In general, multidetector CT scans are reported to have a 95% sensitivity and specificity for the diagnosis of a high-grade SBO, defined by radiologic terms as having no gas or fluid in the bowel distal to the site of obstruction with small bowel diameter > 2.5 cm proximal to the obstruction. 11 However, they are also often described as having less accuracy with less visual clues in predicting partial SBOs and complications of SBOs, such as ischemia. A recent systematic review and meta-analysis found that the sensitivity and specificity for diagnosis of an SBO on CT scan were 91% and 89%, respectively, for diagnosis of ischemia 82% and 92%, and for diagnosis of a transition point 92% and 77%. 12 In the systematic review, study limitations included a potential timing bias as the authors did not fully examine the time intervals between the index studies and primary outcomes for the patients, which is significant in patient care. Our patient was peritoneal on examination and clinically warranted an urgent operation without improvement after appropriate resuscitation. His CT scan did demonstrate concerning findings, but it was the combination of the clinical symptoms, radiologic imaging and lack of improvement in clinical status that led to transfer to the operating room. In addition, the systematic review study primarily analyzed retrospective studies without criteria for contrast-enhanced versus unenhanced studies, which could be discussed as a limitation when analyzing the results compared with standard practice often with contrast enhanced studies if possible. Despite the limitations described above, overall, the systematic review and meta-analysis found the accuracy for an SBO on CT scan, in regard to diagnosis, ischemia and transition point, to be significant. This significance maintains that a CT scan can be a useful adjunct to our diagnostic capabilities, especially concerning radiologic signs defined as bowel wall thickening > 3 mm, whirl sign, fluid in mesentery or pelvis, pneumatosis, venous gas and abnormal bowel wall enhancement arise. 11
In summary, the reliability of CT scan alone for diagnosing SBO remains to be questioned, but when used with high clinical suspicion and in reference to clinical presentation, it has proven to be a positive addition to clinical decision making. The overall decision for operative intervention in a patient with intussusception presenting with signs and symptoms of an SBO should include the history, physical examination, labs and radiologic studies combined together to give an overall clinical picture of the patient at the time of evaluation. Furthermore, the diagnosis of MD as the cause for intussusception at time of operative diagnosis should be treated with a systematic thought process to first reduce the intussusception, determine viability of the tissue and treat with diverticulectomy or segmental resection. This management of intussusception secondary to Meckel’s diverticulum having a definite indication for diverticulectomy or segmental resection has gained consensus throughout the literature and in clinical application at this time in practice.13,15
Conclusion
We present an interesting case of a 30-year-old male with sudden, acute onset abdominal pain found to have an intussusception of Meckel’s diverticulum causing a small bowel obstruction. The issue was identified early and the patient’s continued guarded clinical status prompted expeditious transit to the operating room for segmental bowel resection and primary anastomosis with subsequent full recovery. This case emphasizes the importance of a complete clinical picture in the decision making process for further management of SBO cases. It reminds us that Meckel’s diverticulum, although less commonly the cause of intussusception resulting in SBO in the adult population, needs to be on the differential diagnosis and a high clinical suspicion for operative intervention in a timely manner should be maintained.
Footnotes
Acknowledgements
The authors acknowledge the continued opportunities for patient care at Stonybrook Southampton Hospital.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.