
Abstract
Primary small bowel tumours are very uncommon accounting about 1% of all gastrointestinal tumours. Intestinal lipomas are a rare entity of benign tumours with an incidence at autopsy ranging from 0.04% to 4.5%, most being asymptomatic. Complications such as obstruction, haemorrhage, intussusception and perforation might demand invasive management. Among these, intussusception is the most rare complication of intestinal lipomas. Here, we present a case of intussusception in a 52-year-old female with a large intramural lipoma of the ileum.
Keywords
Introduction
Intussusception is defined as the invagination of a proximal bowel segment into the lumen of an adjacent distal segment. Since its first description in 1674, it is considered a disease of early childhood.1,2 However, about 5% of intussusception is present in adults and causes 1%–5% of intestinal obstruction in this adult population with equal prevalence in male and female. 3 While childhood intussusception is considered idiopathic in 90% of the children, a mechanical cause can be find in adult intussusception in over 90% of the patients. 4 Intestinal lipomas are one of the rare reasons for intussusceptions. 5 Hellström 6 first described intestinal lipomas in 1906 as a rare disease with an incidence at autopsy ranging from 0.04% to 4.5%. Lipomas can be found throughout the intestines. They are encountered in 75% in the colon and in less than 25% in the small intestine. They are the second most common benign small bowel tumours after leiomyomas. Their localisation in the small bowel is the ileum in 50% of the patients. They originate in the submucosa in 90% of the patients and usually are solitary (85%–89%). Usually, lipomas are asymptomatic but may give rise to symptoms related to their size and localisation. Symptoms are the result of intussusception, intestinal obstruction, volvulus and haemorrhage.7–9 The peak age of disease is in the sixth to seventh decade of life. Because of its rare prevalence and unspecific symptoms, the diagnosis is challenging. We report the case of an intestinal lipoma complicated by intussusception in a 52-year-old female.
Case
A 52-year-old female patient with past medical history of open appendectomy, a uterus myomatosus and a borderline disorder presented with complaints of unspecific abdominal pain and intermittent diarrhoea at our hospital in December 2017. When presenting at the emergency department, she was first triaged to the colleagues of internal medicine because of chronic and unspecific symptoms. The patient described intermittent abdominal cramping and unusual soft stool over the last 3 months. She had lost 4 kg weight during this episode. The patient reported that she actually felt hungry but was anxious eating something because she feared abdominal pain. In addition, she was suffering from nausea and repetitive vomiting during the last week. She described no urgency, dysuria or haematuria. At the time of presentation, she was menstruating. A haemoccult test conducted by her general physician (GP) was positive for occult bleeding. Previous blood tests showed a microcytic anaemia. Therefore, the GP treated her for an iron deficiency–related anaemia without determining the serum ferritin levels. No further examinations or diagnostic tests had been induced. Due to the borderline disorder, she regularly takes medicaments such as serotonin reuptake inhibitors (trazodone 150 mg/d, paroxetine 20 mg/d and zolpidem 10 mg/night).
On clinical examination, we found a 52-year-old obese patient with a body mass index of 33 kg/m2 in a good general condition with normal blood pressure (145/76 mmHg) and heart rate (101/min). She presented afebrile with 36.2°C and had a normal oxygen saturation of 98% under room conditions. Beside mild umbilical pain on palpation, the abdominal examination and auscultation was normal. Digital rectal examination showed no mass or bleeding.
Therefore, the following investigations were performed: laboratory findings showed microcytic hypochromic anaemia of 108 g/L, normal blood white cells of 9 g/L (range 4.5–11 g/L) and a CRP of 20 mg/L (range < 10 mg/L). Urine analysis was positive for blood and leucocytes. We ordered a computed tomography (CT) scan of the abdomen and pelvis with triple contrast to investigate the unspecific symptoms. The CT showed an obstructive fatty lesion of the ileum with dilatation of the oedematous adjacent bowel causing intussusception and consecutive mechanical ileus (Figure 1). There were no signs of bowel ischaemia. The surgery was scheduled.

(Coronar section): Abdominal computed tomography showing an obstructive fatty lesion of the ileum with dilatation of the oedematous adjacent bowel causing intussusception and consecutive mechanical ileus. There were no signs of bowel ischaemia.
We decided to perform a diagnostic laparoscopy first. Patient received single-shot intravenous antibiotics with cefuroxime 1.5 g and metronidazole 500 mg. As the ileus was mild, we created the capnoperitoneum with the Verres needle uneventfully up to 12 mmHg. We placed a 12 mm versaport umbilical. Two 5 mm ports were placed under vision one in each site of the lower abdomen. The laparoscopy showed a clear fluid in the right abdomen. The bowels were normal in colour and appearance. No adhesions were obvious. As we knew from the CT scan that the problem was in the ileum, we put the patient in trendelenburg position. Revision of the small bowel showed the invagination in the right lower abdomen. Except the local free fluid, the abdomen was clean.
In a next step, we performed the desinvagination of total 30 cm of small bowel until reaching the pediculated basis of the endoluminal tumour shown in Figure 2. In order to perform a segmentectomy of the ileum containing the endoluminal tumour, we performed a small laparotomy of 4–5 cm umbilical. The alexis laparoscopic wound protector and retractor (entry size small) was inserted. The ileum could be easily moved to extra-abdominal and non-oncologic resection of an 8 cm segment containing the palpatory soft tumour was performed. The resected specimen was sent for histopathology (Figure 3). Finally, an end-to-end anastomosis with PDS 4.0 in running suture technique was done and the mesentery was closed again. The laparotomy was closed with a PDS-loop in Everett technique; skin closure was performed with absorbable suture. The surgery lasted 50 min and the patient was admitted to the normal ward. The postoperative progress was totally uneventful; patient received no antibiotics and was discharged at home without any symptoms on postoperative day 6.
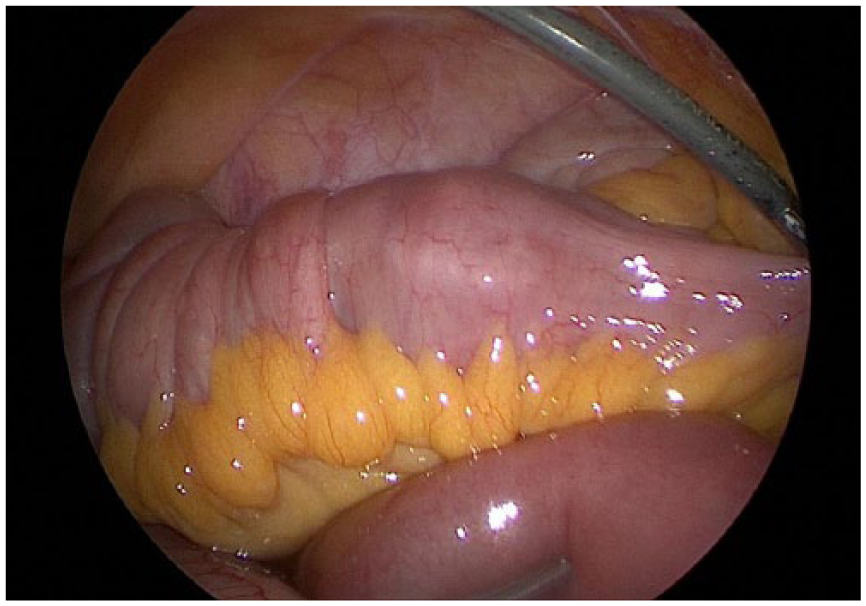
In the right lower abdomen, the ileocolic region was located. The terminal ileum appeared thickened and oedematous. In total, 30 cm of ileum was invaginated caused by a large and on palpation soft endoluminal tumour. Carefully desinvagination was performed with the microfrance.

Histopathological analysis of the tumour showed an 8 cm big intramural lipoma with ulcerative alterations of the adherent mucosa of the ileum. There was no sign of malignancy.
Discussion
Intussusception in adults is very rare with an incidence of two to three cases per population of 1,000,000 per year. 10 When it is found in adults, the cause is usually secondary to a pathologic lead point within the bowel due to altered normal peristaltic movements. 4 Neoplasms such as lipomas are the most common reason of adult intussusception. Lipomas are more common in the colon (75%) than in the small intestine (<25%). They are the second most common benign small bowel tumours after leiomyomas. Their usual localisation in the small bowel is the ileum in 50% of the cases. The peak age of disease is in the sixth to seventh decade of life. They originate in the submucosa in 90% of the cases and usually are solitary (85%–89%). Size may range from 1 to 30 cm. Usually, asymptomatic they can give rise to symptoms related to their size and localisation. 75% of those greater than 4 cm are symptomatic. The symptoms are the result of intussusception, intestinal obstruction, volvulus due to subserosal lipoma and haemorrhage due to ulcerations of the overlying mucosa caused by direct pressure from the lipoma or the intussusception itself.7–9 In contrast to the acute presentation of childhood intussusception, the adult type usually has a subacute or chronic onset. Less than 20% present with acute bowel obstruction. A palpable abdominal mass is present in only 7%–42% of the cases.3,9 Intermittent intussusception due to the lipoma may cause non-specific symptoms and carry a further challenge for diagnosis. 11 In adults, intussusception usually presents with intermittent abdominal pain, nausea, vomiting, constipation, melena or even weight loss. 12 In our case report, the patient had a very mild clinic. The laboratory findings showed anaemia and our patient also described similar unspecific symptoms. In the literature, occult haemorrhage and intermittent intussusception are the most frequent clinical findings. The psychiatric background of the patient in our case report made the interpretation of the clinical findings difficult and might delay the diagnostic tests. The information of colic pain and altered stool, the presence of appetite but fear of eating because of vomiting, pain and the anaemia were reasons for the CT of the abdomen for further examination.
Preoperative diagnosis is difficult due to the variability of the clinical presentation. According to the literature, only 39.1%–44.4% of lipomas as the underlying disease are diagnosed pre-operatively. 13 CT scan is the imaging of choice: radiological finding is a mass lesion, representing a thickened segment of the bowel and the tumour with low density equal to fat. CT scan can also give indirect signs of bowel ischaemia like free fluid and fluid or gas collection in the intestinal wall. CT has a specificity of 100% and sensitivity of up to 87% in adults.14,15 In our case, CT showed the typical characteristics of a lipoma without further complications.
The localisation of intussusception in the gastrointestinal tract is also important: colo-colonic intussusception is in >70% caused by a malignancy. 3 Neoplasia is also a leading lesion in 57% in the small bowel but malignancy here is less frequent (30%). Seventy percentage of adult small intestine intussusception is caused by benign entities. 13 In our case report, the fatty lesion was located in the terminal ileum. No pathologic lymph nodes were detected in the CT scan. In the laparoscopy, the mesentery of the adherent bowel segment was soft and not altered. The tumour on palpation was also soft. Due to these findings, we decided to perform a non-oncologic segmental small bowel resection.
In the literature, there is no consensus on whether laparoscopy can be applied to adult intussusception with respect of safety and efficacy.16,17 In the present case, we selected laparoscopy for the following reasons: the patients clinical condition was good. Clinically and radiologically, the bowel was not distended too much so that a laparoscopic approach was still possible and safe. There were no signs of ischaemia of the bowel segment. Except an open appendectomy, patient did not undergo previous surgery; thus, the probability of intra-abdominal adhesions was low. Intra-operatively, the affected bowel segment of our patients appeared short with a mild image of an ileus. We did not need to perform a conversion to laparotomy. There are other case reports described where an open surgery was necessary because preoperative findings suggested the necessity of large resection such as hemicolectomy. 18 Another reason for laparotomy was a large tumour and the high probability of malignancy due to localisation in the colon. 19
Conclusion
This case report focuses on the difficulties of diagnosing adult intussusception on time. Appropriate alertness and proper investigations are important and needed for prompt diagnosis and treatment to ensure the best possible postoperative outcome. CT scan is the imaging of choice with a high sensitivity and specificity. Surgical resection is the treatment for intussusception in adults as there is nearly always an underlying tumour. The severity of ileus, radiological signs of malignancy, localisation of the tumour, length of the affected bowel and patient’s condition should be considered when choosing the type of surgical access to the abdomen. We hope through sharing our approach and experience that other physicians will keep this rare differential diagnosis in mind when treating patients with chronic abdominal pain in the emergency department.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for her anonymised information and accompanying images to be published in this article. A copy of the written consent is available for review on request.