
Abstract
Placement of a nasointestinal ileus tube or long tube for gastrointestinal decompression is a new and effective treatment for small bowel obstruction. Such tubes are associated with very few adverse effects. However, several cases of intussusception caused by a nasointestinal ileus tube have been reported. No general diagnosis or treatment guideline has been established for such a complication. We herein present three cases of intussusception caused by nasointestinal ileus tube placement along with a literature review that summarizes some important clinical characteristics of nasointestinal ileus tube-induced intussusception. A diagnosis of intussusception should be considered if severe abdominal pain and distension recur after insertion of a nasointestinal ileus tube. Computed tomography may assist making the diagnosis, especially in patients with typical features such as the “Target sign,” “Glasses sign,” or “Mickey Mouse sign.” Although nasointestinal ileus tube-induced intussusception is rare, clinicians should give more attention to the risk of this complication.
Keywords
Introduction
Placement of a nasointestinal ileus tube for gastrointestinal decompression is a new treatment for small bowel obstruction (SBO). The nasointestinal ileus tube commonly used in our institution is a hydrophilic ileus tube (CLINY double-balloon type; Create Medic Co., Ltd., Tokyo, Japan). This 18-Fr tube is 300 cm in length and contains three channels and two balloons. Side holes in the distal end of the tube are present for negative pressure and decompression. A 350-cm-long guide wire is used with this tube (Figure 1). Several studies have shown that nasointestinal ileus tube decompression is successful in 80.0% to 91.6% of patients with adhesive SBO.1–3 The nasointestinal ileus tube can relieve the intestinal edema and obstruction by enteral decompression. This procedure has been confirmed to be a simple, safe, and minimally invasive approach. Adverse effects are uncommon, such as throat injury or obstruction or rupture of the tube, and its clinical use is associated with no serious problems. 4 However, five cases of intussusception caused by nasointestinal ileus tube placement have been reported since the 1980s.5–8 The symptoms of intussusception caused by nasointestinal ileus tube placement are usually so atypical and uncommon that no general treatment guideline has been established for this type of intussusception. Nevertheless, nasointestinal ileus tubes are being applied increasingly more routinely for adhesive SBO. We herein present three cases of intussusception caused by nasointestinal ileus tubes in our single center to establish clinically available characteristics for diagnosis and treatment.
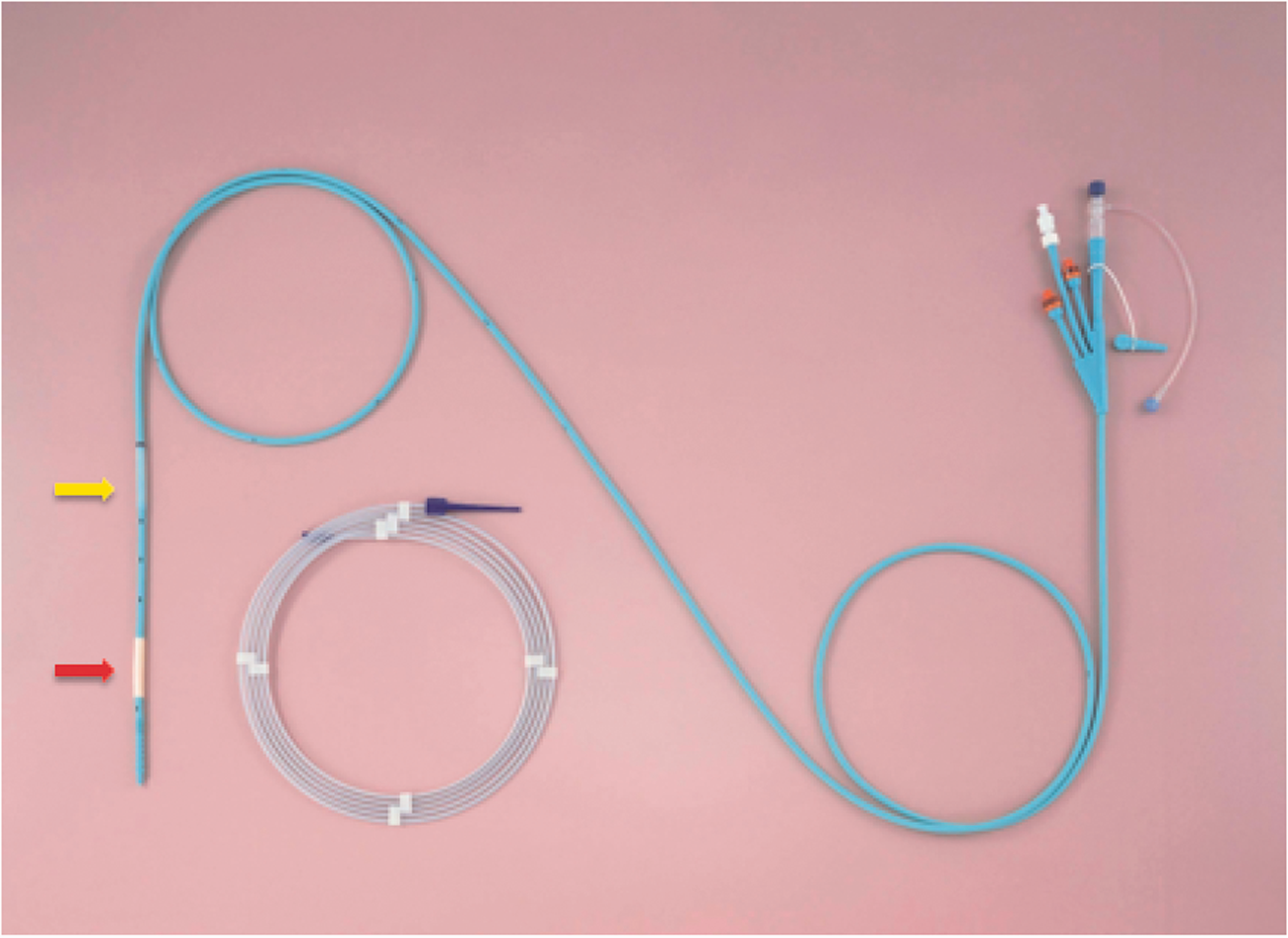
Image of the nasointestinal ileus tube. The 18-Fr tube is 300 cm in length and has three channels and two balloons. The yellow arrow indicates the posterior balloon, and the red arrow indicates the anterior balloon.
Case presentation
Case 1
A 74-year-old man presented to our emergency department on 23 May 2017 because of a 1-month history of recurrent abdominal bloating with pain. He had undergone radical total cystectomy and bladder reconstruction with the ileum for bladder cancer 2 months previously. Physical examination revealed no abdominal signs. Laboratory tests showed a white blood cell count of 10.6 × 109/L, C-reactive protein level of 26.9 mg/L, and albumin level of 26.8 g/L. Computed tomography (CT) showed a partial intestinal obstruction. The patient’s abdominal pain was relieved after nasointestinal ileus tube insertion 5 days later but recurred again after 2 days. Another CT examination showed a “Target sign,” which suggested antegrade intussusception in the proximal jejunum (Figure 2(a)). We removed the water from the anterior balloon and pulled the tube out by about 50 cm. The patient’s abdominal pain was relieved 1 day later. The nasointestinal ileus tube was removed 20 days later, and the patient was discharged 22 days after admission.

Images of Case 1. (a, b) Contrast-enhanced computed tomography showed an intussusception around the ileus tube. The intussusception resembled a target in the image (yellow arrow in image (a)).
Case 2
A 41-year-old woman complained of recurrent abdominal pain for 1 month, which had become aggravated for 1 week before presentation. She was admitted to the hospital on an emergency basis on 25 March 2013. Physical examination indicated slight tenderness around the umbilicus with no rebound tenderness. Laboratory test results were normal. A CT scan suggested SBO. Her abdominal pain was relieved after insertion of a nasointestinal ileus tube. She was able to ingest a liquid diet after 3 days, but abdominal distension occurred 5 days later. An imaging examination with water-soluble contrast showed an intestinal obstruction (Figure 3(a)). CT showed an intussusception in the ileum resembling a pair of glasses (Figure 3(b)). We performed a laparotomy 10 days later, and an antegrade intussusception was found in the ileum approximately 100 cm from the ileocecum. Three tumors were observed in the ileal wall after restoring the intussusception; the largest of the three tumors was 3 cm in diameter. The tube was positioned across the intestinal passage of the intussusception (Figure 3(d), (e)). The pathological diagnosis of the tumors was mesenchymoma. The patient recovered well and was discharged 9 days after the operation.

Images and intraoperative photos of Case 2. (a) Water-soluble contrast showed an intestinal obstruction. (b, c) Computed tomography showed an intussusception in the ileum. The intussusception resembled a pair of glasses in the image (yellow arrow in image (b)). (d) An antegrade intussusception was found in the ileum about 100 cm from the ileocecum (yellow arrow). (e) Three tumors were found in the ileal wall; the largest was about 3 × 3 cm (yellow arrow).
Case 3
A 45-year-old man was admitted to the hospital on an emergency basis for a 3-day history of abdominal pain in May 2017. He had a 10-year history of Crohn’s disease and had been medically treated for about 4 years; he was unsure of the name of the drug. Physical examination indicated abdominal distention with neither tenderness nor rebound tenderness. Laboratory examinations showed a C-reactive protein level of 49 mg/L. Tumor markers and other laboratory test results were within the normal ranges. We inserted a nasointestinal ileus tube 2 days later. The tube moved downward 200 cm after 3 days. His abdominal pain and distension were relieved. However, he developed critical abdominal pain again 4 days later. Physical examination showed an intestinal pattern in the abdomen with tenderness and rebound tenderness. Bloody drainage from the nasointestinal ileus tube was observed (Figure 4(a)). CT showed an intussusception and intestinal volvulus (Figure 4(b), (c)). We performed an emergency laparotomy and found an antegrade intussusception of the ileum about 170 cm from the ileocecum, and part of the ileum had twisted 180 degrees. An approximately 100-cm-long section of necrotic ileum was found. The tip of the tube was located inside the necrotic intestinal passage. A fistula was also present between the ileus and sigmoid colon. We removed the necrotic ileum and performed a partial ileostomy and colostomy. He recovered well and was discharged 20 days after the surgery.

Clinical presentation of Case 3. (a) An intestinal pattern was observed in the abdomen (yellow arrow), and liquid blood drained from the ileus tube (red arrow). (b, c) Computed tomography showed an intussusception and intestinal volvulus (yellow arrow in image (b)).
Discussion
Placement of a nasointestinal ileus tube is recommended as the initial treatment for benign adhesive bowel obstruction and is widely used in the clinical setting. 9 Nasointestinal ileus tube-related intussusception is rare. Several case reports have described jejunostomy tube-induced intussusception, but fewer cases of intussusception caused by a nasointestinal ileus tube have been published. Four recent reports have described five cases of intussusception induced by a nasointestinal ileus tube5–8 (Table 1).
Summary of cases of intussusception induced by nasointestinal ileus tube.

F, female; M, male; CT, computed tomography.
Several possible mechanisms of jejunostomy tube-induced intussusception have been proposed. Folds of the small intestine can telescope over the long tube, and the tip of the feeding tube can act as the leading point and drag the proximal segment over the distal segment during a peristaltic wave.10,11 Reduced fatty tissue (e.g., omentum, mesentery) allows free movement of the intestine. 11 However, the mechanism of nasointestinal ileus tube-induced intussusception is not clear because of the rarity of this condition. One theory of nasointestinal ileus tube-induced intussusception is that folds of the small intestine may telescope over the long tube because of ongoing propulsive peristalsis over a severely dilated proximal intestine. 7 Asymmetric peristalsis of the intestinal wall in the presence of a bowel obstruction may also lead to intussusception. 6 We propose that the anterior balloon of the nasointestinal ileus tube might act as a leading point to drag the bowel.
The symptoms of intussusception induced by a nasointestinal ileus tube are usually the same as the symptoms of bowel obstruction, such as vomiting, abdominal pain, and distension. 6 Consequently, intussusception is easily ignored or misdiagnosed. As in our three cases, the onset of ileus tube-induced intussusception frequently occurs during the progression-free interval. When symptoms of bowel obstruction reappear during this interval, intussusception should be considered. The location of the intussusception is usually in the proximal jejunum, most frequently near the anterior balloon of the tube.5,6 When the obstruction is caused by the intestinal wall lesion itself and not a parenteral factor, intussusception is prone to appear as the tube advances, which may be due to asymmetric peristalsis. 7
Water-soluble contrast X-ray and CT examinations are helpful for making a correct and timely diagnosis. Multidetector CT is well suited to delineate the presence of the disease and provides valuable information about the site of the intussusception, the intestinal segments involved, and the extent of the intussuscepted bowel. Moreover, multidetector CT can demonstrate complications of intussusception such as bowel wall ischemia and perforation, which necessitate prompt referral for surgery. 12 Three typical CT imaging signs of nasointestinal ileus tube-induced intussusception are the “Target sign,” “Glasses sign,” and “Mickey Mouse sign” (Figure 5(a)–(c)). These signs indicate different severities of nasointestinal ileus tube-induced intussusception.
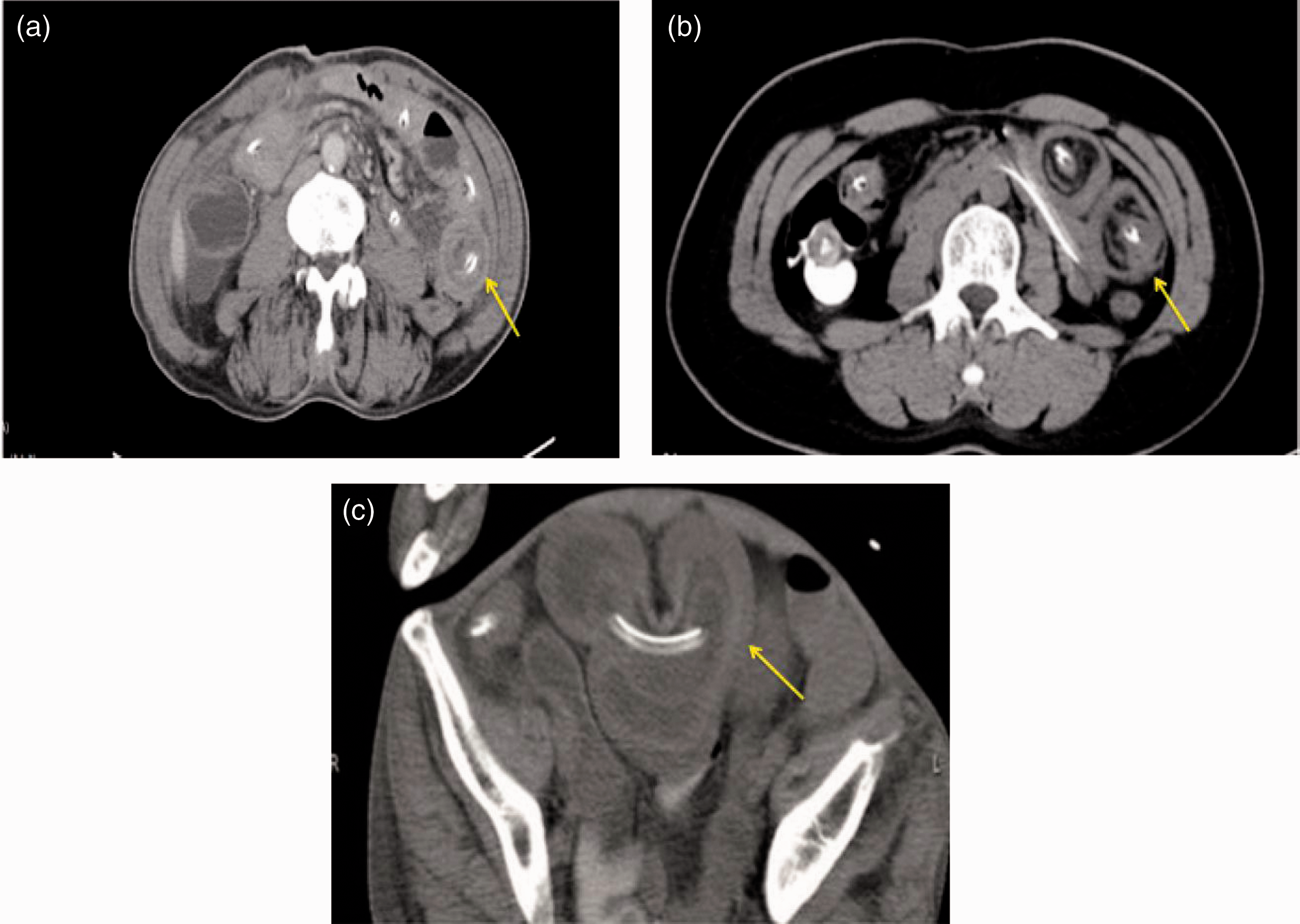
Summary of three typical computed tomography imaging signs of nasointestinal ileus tube-induced intussusception. (a) Target sign. (b) Glasses sign. (c) Mickey Mouse sign 7 .
According to the literature and our experience, the severity of intussusception with the “Target sign” should be the mildest. It can usually be relieved after pulling out the tube and needs no surgery, leading to a relatively better prognosis. In the first case, CT showed the “Target sign”, and the patient’s symptoms were not severe. We achieved successful reduction by simply pulling out the tube. The “Glasses sign” often indicates a longer duration of telescoped intestine, which may be more severe than the “Target sign”. A Mickey Mouse-shaped invagination often suggests the most severe type of intussusception. Clinicians should be on alert for a large segment of intestinal volvulus exhibiting the Mickey Mouse sign. 7 An intussusception with the “Glasses sign” or “Mickey Mouse sign” is difficult to restore and often requires surgical intervention. Laparotomy, and often intestinal resection, is usually needed if the diagnosis of intussusception is established. 7 One reason may be the atypical symptoms of the intussusception, and another may be lack of awareness of this rare complication. Earlier diagnosis and intervention lead to better outcomes. Eisen et al. 13 stated that small bowel intussusception should be reduced only in patients in whom a benign diagnosis has been made preoperatively or in patients in whom resection may result in short gut syndrome. Patients with undetermined bowel obstruction with no history of previous laparotomy should undergo resection without reduction because of the incidence of associated malignancy. 14 In Case 2 of the present series, preoperative CT revealed no tumors, but mesenchymomas were found in the ileum during the operation. It is sometimes difficult to distinguish small tumors in patients with intestinal obstruction because of the swollen, thickened intestinal wall on CT images. The presence of a tumor likely increases the risk of intussusception.
We have several recommendations to prevent this kind of complication. First, determine whether any lesions are present in the intestine before inserting the tube. Second, improve the care of the tube, including the rate of water injection into the anterior balloon, drainage volume, and length of tube advanced into the intestine. Third, dynamically observe the patient’s symptoms and signs.
Conclusion
The diagnosis of nasointestinal ileus tube-induced intussusception is difficult because the symptoms are not typical and are usually similar to those of the primary disease. A diagnosis of intussusception should be considered if severe abdominal pain and distension recur after inserting the nasointestinal ileus tube. CT may help to achieve the diagnosis, especially in the presence of typical features such as the “Target sign”, ”Glasses sign”, or “Mickey Mouse sign”. Intestinal resection is probably needed for these high-risk patients; however, the indications for surgical intervention are difficult to determine and should be studied in future research. Although nasointestinal ileus tube-induced intussusception is uncommon, clinicians should give more attention to the possibility of this complication. Early diagnosis by CT is mandatory to prevent disease progression to severe complications of ileus tube-induced intussusception such as bowel necrosis and to improve the clinical outcome.
Footnotes
Acknowledgment
We gratefully acknowledge Dr. Shuai Wang for helping to review this paper.
Consent
Written informed consent was obtained from the patients or their legally authorized representatives regarding use of their clinical information. All analyzed data were anonymous.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics
This study was approved by the Human Research Ethics Committee of The Fourth Affiliated Hospital of Zhejiang University School of Medicine (Approval No. K20190041).
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.