
Abstract
Subungual exostosis is a rare solitary benign osteocartilaginous tumor that arises from the tuft of the distal phalanx beneath the nail. Because of its multiple clinical presentations, it is commonly underdiagnosed, resulting in delayed diagnosis and inadequate treatment. This report provides results from a 6-year retrospective study. All patients with a sonographic diagnosis of subungual exostosis confirmed surgically were selected. The data came from a series of 19 patient cases. Only 15.7% were clinically suspected. The median age was 21 years, and 63% were females. The sonographic findings were nail dystrophy, distal onycholysis, abnormal nail incurvation, subungual space enlargement, and the presence of hyperechogenic subungual image with acoustic shadowing that continued until the phalanx surface. Sonography provides an excellent diagnostic method for subungual exostosis, with findings that are pathognomonic.
Subungual exostosis, also known as “Dupuytren’s exostosis,” was described for the first time in 1817.1,2 It is a rare solitary benign osteocartilaginous tumor that arises from the tuft of the distal phalanx beneath the nail.1–5 Even though this can occur at any age, about 50% of cases occur during the second or third decade of life, and the other half occur in patients older than 40 years, 2 being the most frequent ungual tumor in young patients. The lesion is mostly found in the dorsomedial region of the affected phalanx 4 and manifests clinically by alteration of the overlying nail or the periungual soft tissues.1,2 Subungual exostosis of the fingers is less common, with fewer than 60 cases reported in the literature. 2
The etiology of subungual exostosis is unknown. However, trauma or chronic infections in the lesion area have been suggested as possible causes.1,2,4,5 It was previously considered as a variant of osteochondroma but is currently recognized as a different entity with its own clinical and histopathologic characteristics. 4 In histology, the lesion consists of a nucleus of mature trabecular osseous tissue with a capsule of proliferating fibrocartilaginous tissue,1,5 while osteochondromas are capped by hyaline cartilage. 1 In exostosis, bone is formed directly from fibrous tissue, whereas in osteochondromas, it is derived from endochondral ossification. 1
Clinically, subungual exostosis has multiple presentations, appearing frequently as a painful mass with elevation and deformation of the nail bed, which can be associated with inflammatory changes of the periungual soft parts.1,4,6 Subungual exostosis can resemble other dermatologic entities,7,8 and in some reports, 44% to 80% of the cases were initially misdiagnosed as subungual wart, squamous cell carcinoma, fibroma and pyogenic granuloma, onychocryptosis, cysts, glomus tumor, and malignant melanoma.2,4,7
Subungual exostosis can present with alterations of the nail plate as a clamp nail or hyperkeratosis or onycholysis, simulating onychomycosis. It can also debut as onychocryptosis, and there may even be an absence of nail dystrophy and present only as pain. Given the multiple clinical presentations, it is usually underdiagnosed, which leads to delayed diagnosis and inadequate treatment.1,2,9–11 From the dermoscopic point of view, some features that could help clinical suspicion have been recently published: vascular ectasia, hyperkeratosis, and ulceration. However, a radiologic study usually confirms the diagnosis. 12
Most textbooks and reports describe findings on radiographs and only recently in ultrasonography (US) and magnetic resonance imaging (MRI). 4 The objectives of this study are to describe high-resolution US signs frequently found in subungual exostosis that allow the radiologist and sonographer to suspect this entity when such findings are identified.
Materials and Method
This retrospective study was approved by the Institutional Board Review and granted a waiver for informed consent. A soft-tissue US database was reviewed during a 6-year period for patients referred to the radiology department for high-resolution US, with a clinical ungual/subungual finding.
All patients with a US diagnosis of subungual exostosis were selected. The inclusion criteria were a subsequent radiologic study of the digit in the archives and histologically confirmed diagnosis.
The examinations were performed with Philips (iU22 or Epiq model) or Toshiba Aplio i800 ultrasound equipment. High-resolution linear (24-5 MHz, 18-5 MHz, and 17-5 MHz) transducers were used for imaging. In most cases, a gel pad interface was also needed, interposed between the transducer and the skin surface, to prevent excessive compression. Images were retrieved from a picture archiving and communication system (Agfa IMPAX), and US findings were reviewed retrospectively by two experienced radiologists (with 10 and 25 years of experience performing US, respectively) who provided a consensus appraisal of these findings. Nail dystrophy, onycholysis, abnormal nail incurvation, subungual space enlargement, and the presence of hyperechogenic subungual image with acoustic shadowing that continues until the phalanx surface were evaluated.
All electronic archives, follow-up images, and histologic findings of the patients were retrieved from the electronic medical records. Frequency descriptors are presented.
Results
Nineteen cases were identified; 16 (84.2%) were referred by dermatologists. Twelve patients were female (63%), with an average age of 22 years, ranging from 9 to 46 years old. The initial clinical diagnoses were soft-tissue tumor or nail bed cyst (12 cases), wart versus tumor (3 cases), trauma (1 case), suspicion of foreign body (1 case), and suspicion of exostosis (3 cases). Therefore, in 15.7% of the cases, the diagnosis was clinically suspected (directly or indirectly; Figure 1).

Patient referred to sonographic examination with suspicion of subungual tumor.
On clinical presentation, the frequency order of the compromised toe corresponded to the first toe in 15 cases (79%), second toe in 3 cases (16%), and third toe in 1 case (5%).
The US findings on the nail plate included nine patients with hyperkeratosis or nail dystrophy, seven with distal onycholysis, seven with alteration of the ungual incurvation and greater obliquity of the nail, and two cases with normal ungual images (Figure 2). When the subungual space was analyzed, an increase in the thickness of the subungual space could be seen in 17 of 19 patients (89%), an asymmetric increase of the subungual space in 13 of 19 patients (68%), and the presence of hyperechoic subungual images with acoustic shadowing that lays in continuity with the bone surface of the distal phalanx in 19 of 19 cases (100%; Figures 3–5). Alteration of the nail root was not demonstrated in any patient.
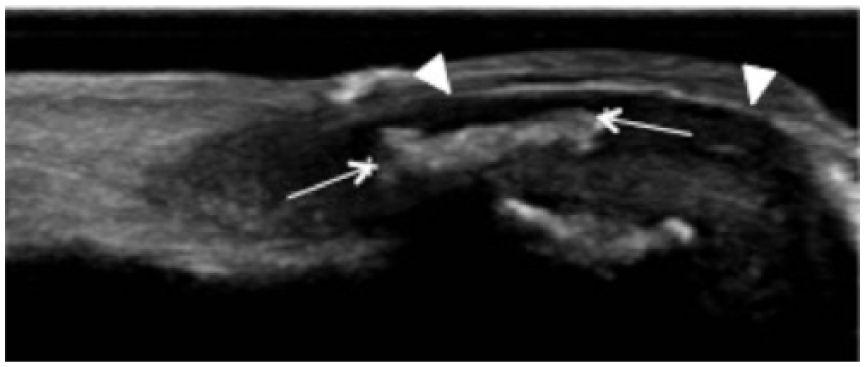
Sonography demonstrated a hyperechogenic subungual image with acoustic shadowing (arrows) in contact with the cortical bone surface, concordant with exostosis. The nail surface was slightly uplifted (arrowheads), and the subungual space was enlarged.
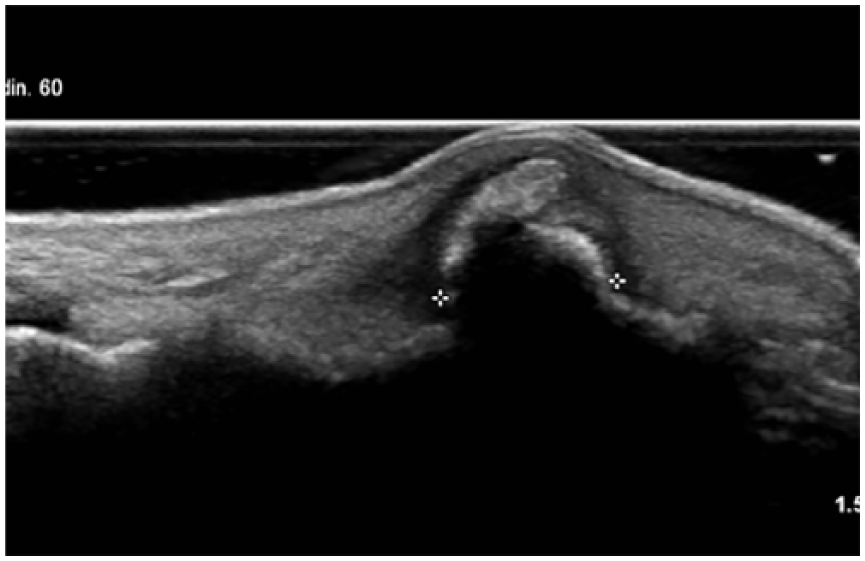
Hyperechogenic subungual sonographic image that continued with the phalanx bone surface.
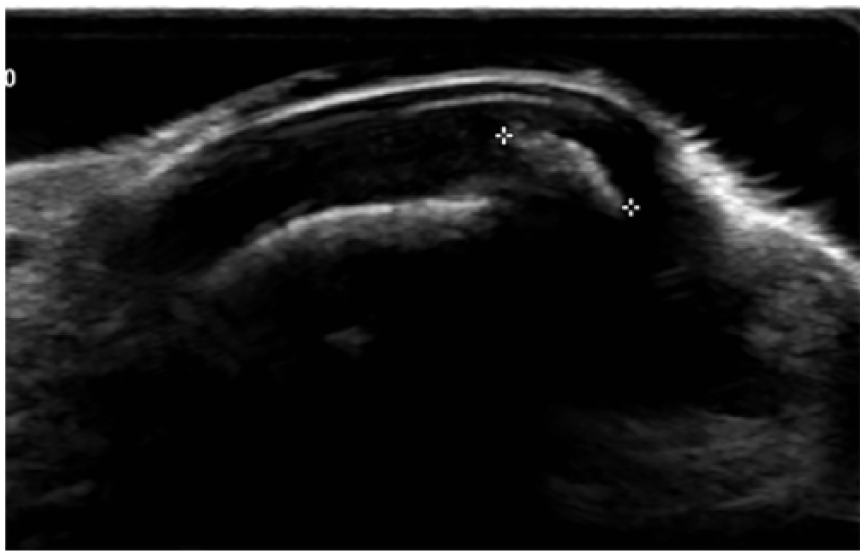
A transverse sonographic view that demonstrates asymmetric subungual space, with irregularity of the nail surface in the exostosis side.
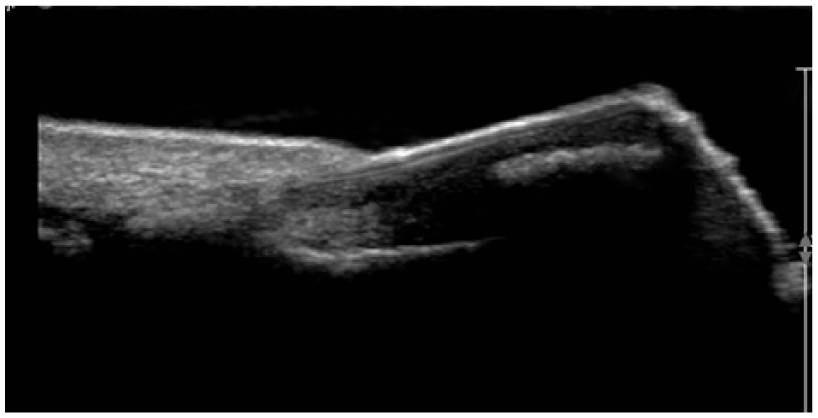
A longitudinal sonographic view that demonstrates an echogenic subungual exostosis and normal shape and obliquity of the nail.
In all patients, after the US diagnosis, a radiographic study was requested with frontal, lateral, and oblique projections of the affected digit.
When the radiographic projections were analyzed separately, the lesion was seen in a frontal projection in 15 of 19 patients, in lateral projection in 17 of 19 patients, and in oblique projection in 16 of 19 patients. In all cases, the lesion was demonstrated in at least two projections.
In 9 of 19 cases, the projection that best represented the lesion was the lateral, and in 8 of 19 cases, it was the oblique projection (Figure 6).
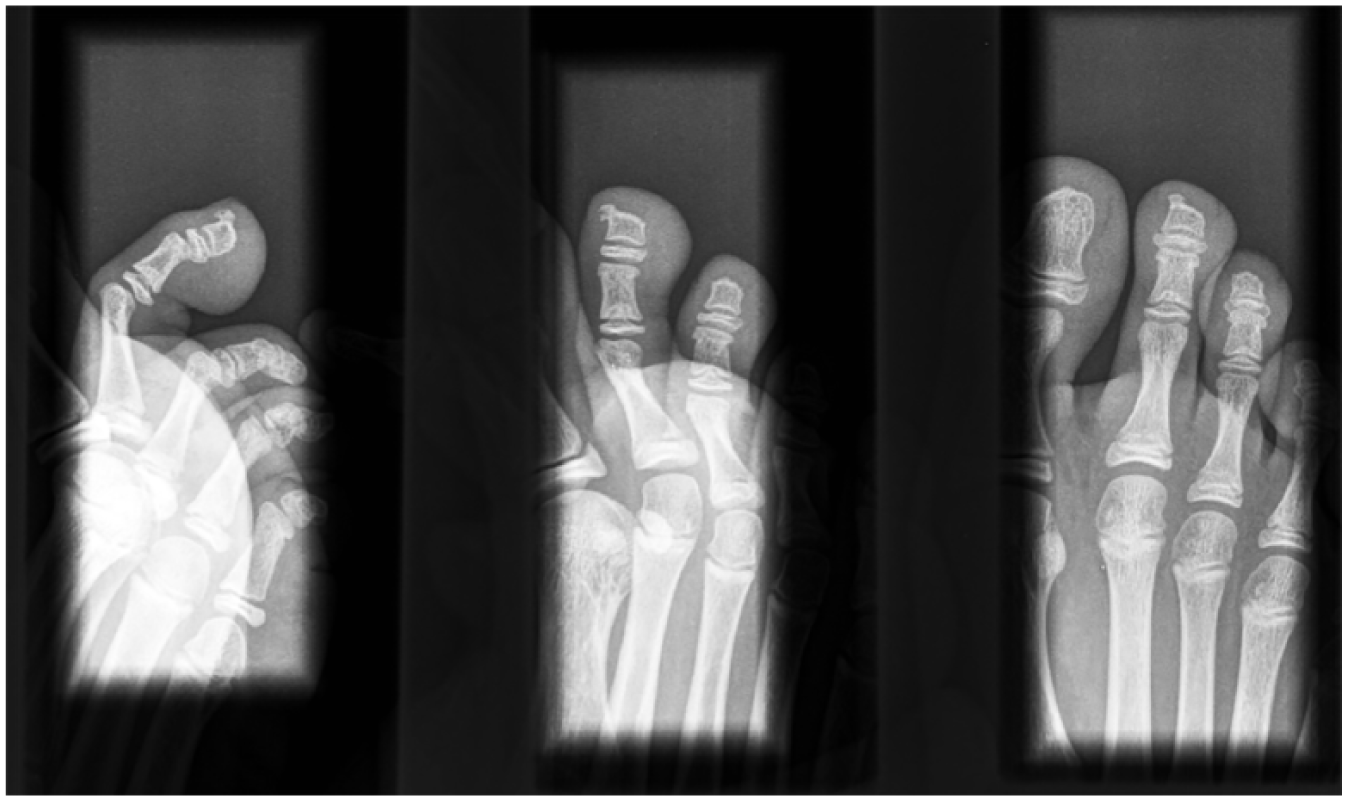
Lateral (L), frontal (F), and oblique (O) radiographic projections of the first toe. The subungual exostosis is best identified in the lateral radiographic projection.
All cases reviewed had a diagnosis that was surgically confirmed and pathologically proven.
Discussion
Subungual exostosis is an infrequent finding in nail US, but it is extremely important to be considered because management will differ. Even though radiographs may be needed to document its presence, the radiologist and sonographer must raise suspicion of this entity when certain clinical and US findings are present. In this series, sex distribution was as described in the literature (63% females), and most cases occurred on the foot (79% on the hallux). Subungual exostosis was clinically suspected in only 15.7% of the cases, and in most instances, the clinical diagnosis was a soft-tissue tumor, soft-tissue enlargement, or cyst. This highlights the importance of a proper approach from the radiologist or sonographer in order to provide this important differential diagnosis, which will dramatically change the management and/or surgical resolution.
It has been described that radiographs are diagnostic for the bone component of subungual exostosis. 2 In most cases, they show an exophytic trabecular bone growth with or without a defined cortex, which projects from the dorsomedial surface of the distal phalanx.1,2,4 However, in early stages, subungual exostosis may not be visible on a radiograph because of its fibrocartilaginous nature. 3
MRI is described as the best radiologic technique to represent the effect of subungual exostosis on the surrounding structures and to distinguish this lesion from osteochondroma. 7 The fibrocartilaginous covering of the subungual exostosis is hypointense in T1- and T2-weighted sequences, while the hyaline cartilage of the osteochondroma has high signal intensity on T2-weighted sequences. 7 However, this approach is expensive, not readily available, and is usually performed only when clinical suspicion is high.
With US, subungual exostosis has been described as calcified heterogeneous and hyperechogenic structures, with well-defined margins and posterior acoustic shadowing that presents a hypoechoic fibrocartilaginous capsule. 4 It is located under the nail plate and connects with the cortical osseous surface of the distal phalanx. 6 The nail bed is enlarged, with an upward displacement of the nail plate, and hypovascularization is observed on color Doppler. 4
In this series, US allows for an adequate evaluation of ungual alterations such as hyperkeratosis, nail dystrophy, distal onycholysis, alteration of the nail curvature, and greater obliquity of the nail. The specialists were able to observe an increased thickness and/or asymmetry in the subungual space and the presence of hyperechogenic subungual images with acoustic shadowing that continues until the superficial osseous surface of the distal phalanx, a finding considered pathognomonic by the specialist in charge. Also, it was characteristic, in this series, that no alteration of the nail root was observable.
The mainstay of treatment is the surgical removal of exostosis, which usually relieves symptoms.1,2,8 Hence, approaching the diagnosis correctly is important, which will provide value-added information to the referring clinician.
Conclusion
It is important to understand this pathology because of its multiple clinical presentations and nonspecific clinical diagnosis. US is an excellent diagnostic method for identifying subungual exostosis, with findings that are pathognomonic, allowing a timely and adequate diagnosis. Knowledge of these US findings will allow an earlier diagnosis with less ungual damage.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.