
Abstract
Diagnostic medical sonography is a leading and favored imaging technique in pediatrics. However, diagnostic medical sonography education does not include a standardized specific curriculum in general pediatric sonography. This mixed-methods study aims to (1) measure pediatric sonographers’ self-assessed knowledge, skill, and competence immediately after graduation or cross-training from radiologic technology as compared with their current levels; (2) gain insights from these sonographers of potential topics/techniques necessary to improve students’ general pediatric sonography preparation; and (3) determine their opinions about a specialized registry examination for pediatric sonography. Twenty-two sonographers completed the self-assessment survey, and 11 sonographers participated in focus groups. Experienced general pediatric sonographers reported a significant increase in self-assessed knowledge and skill. The focus groups showed five consistent themes. Sonographers agreed that development of a general pediatric sonography course concentrating on learning general pediatric-related disease processes and protocols would enhance knowledge, skill, and competence immediately after graduation or cross-training; however, opinions were mixed about adding a general pediatric sonography registry examination.
Introduction
In pediatric institutions, the use of computed tomographic scans has decreased because of concerns about radiation exposure, while the numbers of sonograms have markedly increased. 1 General pediatric sonography is notably different from adult sonography, requiring different equipment and specific knowledge, attitudes, and skills for working with the pediatric population. Hence, applying adult techniques to pediatrics is not suitable. For example, the timely sonographic diagnosis of appendicitis can be critical for pediatric patients, as perforation rate is inversely related to the age, and atypical signs and symptoms can commonly obscure the clinical diagnosis. 2 In experienced hands, pediatric sonography for appendicitis has a high sensitivity and specificity and spares the child radiation. 3 Yet, appendicitis is the second-most prevalent condition in pediatric malpractice claims caused by diagnostic errors, with missed diagnoses reported in up to 27% of cases, 2 underscoring the importance and need for better training and experience for those practicing general pediatric sonography.
According to the Commission on Accreditation of Allied Health Education Programs (CAAHEP), 211 accredited diagnostic medical sonography programs in the United States currently offer general (e.g., adult abdomen, obstetrics and gynecology), cardiac, pediatric cardiac, or vascular concentrations. 4 The CAAHEP and the Joint Review Committee on Education in Diagnostic Medical Sonography require programs to meet or exceed the minimum standards for accreditation.5,6 General pediatric sonography education requirements, however, are limited in the CAAHEP guidelines, with little in-depth explanation of specific information, thereby creating a lack of standardization for general pediatric curricula.
The American Institute of Ultrasound in Medicine and the American College of Radiology have suggested that general pediatric sonography is not adequately taught and that sonographers need more supervised direction, as indicated by multiple practice guidelines.7-12 Despite detailed texts on pediatric sonography and National Education Curriculum, whether the knowledge, skills, and competence have been acquired to competently perform general pediatric sonograms at graduation from accredited programs is unknown.6,13-15 The American Registry for Diagnostic Medical Sonography (ARDMS) is an independent nonprofit organization for sonography professionals whose mission is to promote quality care and patient safety through the certification and continuing competency of sonography professionals. An ARDMS needs assessment survey investigating the need for a general pediatric credentialing examination found that the majority of respondents indicated that their facilities perform >500 general pediatric sonography studies annually, with only one-fourth performed at dedicated pediatric hospitals.16,17 Additionally, 53% of respondents were interested in obtaining a general pediatric sonography ARDMS credential; 63% believed that developing a new ARDMS general pediatric sonography credentialing examination is needed; and 68% believed that this ARDMS general pediatric sonography–specific credentialing would improve the quality of patient care. 16 On the basis of this information, the ARDMS has implemented a general pediatric sonography credentialing examination, which began in February 2015. However, the details necessary to create a dedicated general pediatric sonography curriculum and a validated means of assessing sonographer competence and comfort in performing a general pediatric sonography examination soon after graduation remain unknown.5,16 The purpose of this study was to (1) measure pediatric sonographers’ self-assessed knowledge, skill, and competence immediately after training as compared with their current levels; (2) gain insights from these sonographers on potential topics/techniques necessary to improve students’ general pediatric sonography preparation; and (3) determine their opinions about a distinct licensing requirement. The information gained from this deeper discussion could help shape a future general pediatric sonography (hereafter, pediatric sonography) curriculum to best meet future sonography students’ learning needs.
Methods
A mixed-methods study comprising an online self-assessment survey and focus groups was conducted over a two-month period. The study was approved as exempt by the Institutional Review Board of the Cincinnati Children’s Hospital Medical Center.
Study Setting and Participants
The Cincinnati Children’s Hospital Medical Center is an urban academic children’s hospital with a large pediatric radiology department staffed by 36 clinical radiologists and 28 sonographers. 18 Annually >200 000 pediatric imaging procedures are performed, including roughly 24 000 pediatric sonograms. 18 All of these staff sonographers were contacted via email to see whether they would take the survey and participate in the focus group discussions over a two-month period.
Survey Development
The survey was developed de novo by radiologists, sonographers and medical educators. The survey consisted of 15 items that assessed the perceived knowledge, skill, competence, and attitudes of the pediatric sonographers. Survey questions utilized a retrospective pre- and postdesign, with responses anchored along a scale from novice (1) to expert (5). Participants compared their current self-assessed knowledge in pediatric sonography of specific diseases and skill to perform these examinations with that immediately after graduation from a CAAHEP-accredited diagnostic medical sonography program or from internal department-based cross-training for the more senior sonographers. Surveys were piloted on one pediatric physician, two faculty radiologists, and a pediatric sonography manager to establish content validity and were amended accordingly. There were three open-ended questions regarding (1) topics that may have been missing from participants’ education or what would have made their transitions into pediatric sonography easier, (2) reasons for or against a pediatric sonography registry examination through the ARDMS, and (3) any closing thoughts or comments. The survey was accessed via an online survey platform (www.surveymonkey.com); responses were collected anonymously; and results were grouped prior to analysis.
Focus Group Structure and Analysis
Two pediatric sonographer focus groups were conducted via convenience sampling. A moderator introduced the discussion prompts, which included an introduction about pediatric sonography, time spent learning pediatric sonography during formal education, topics that require additional attention in diagnostic medical sonography programs, and overall attitudes on pediatric sonography (see appendix). Each focus group questioning was completed during a one-hour session, audio recorded, and subsequently transcribed. In addition, the moderator took handwritten notes with impressions to augment the audio recording. Grounded theory was used to analyze the focus group results because the constant comparative process of in-depth group interviews and interpretive coding yielded a rich description of participants’ educational experience and desired need for additional training, leading to numerous concepts and interrelationships.19,20 The four-step coding process described by Corbin and Strauss served as the basis for this data analysis. 19 First, the primary investigator performed open coding, yielding seven different codes. Second, during axial coding, the primary investigator and the qualitative researcher went back and forth within the data, refining connections and combining. Third, selective coding was performed to combine categories into a storyline that described sonographers’ attitudes about a general pediatric sonography course. Fourth, themes were developed per the categories and codes; these themes were discussed until the principle investigator and two medical educators reached agreement. Member check was performed as a final step to ensure that the participants agreed with themes developed.
Survey Analysis
Categorical survey responses were summarized with counts and percentages. Likert scale (1–5) responses regarding perceived skill and knowledge were dichotomized at the two highest scores possible (4 and 5). The dichotomized response shifts from retrospective (after training) to current knowledge, skill, and competence level were evaluated with the McNemar test for paired nominal data.
Results
Participants’ Survey Results
Of the 28 sonographers contacted, 22 (79%) completed the survey. The majority of survey participants were Caucasian and female, ranging in age from 25 to 54 years (Table 1). Participants’ self-assessed knowledge, skill, and competence in pediatric renal, abdominal, appendiceal, pyloric, head, hip, liver, gallbladder and biliary tract, and spine examinations increased significantly to the highly experienced/expert category from immediately posttraining to current level (Table 2).
Participant Demographic Information. a
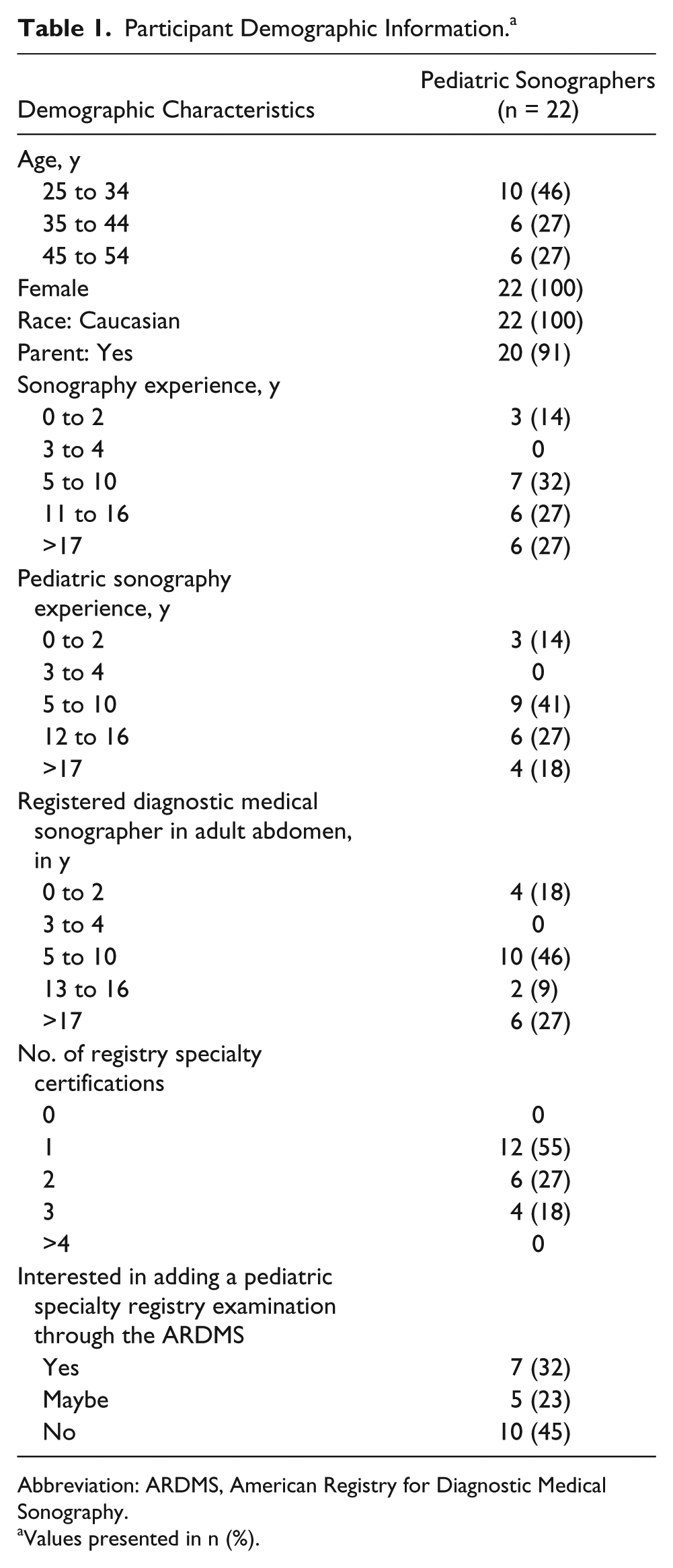
Abbreviation: ARDMS, American Registry for Diagnostic Medical Sonography.
Values presented in n (%).
Sonographers’ Self-assessed Skill Performing Pediatric Sonography Examinations Immediately After Graduation or Cross-training as Compared With Current Level. a
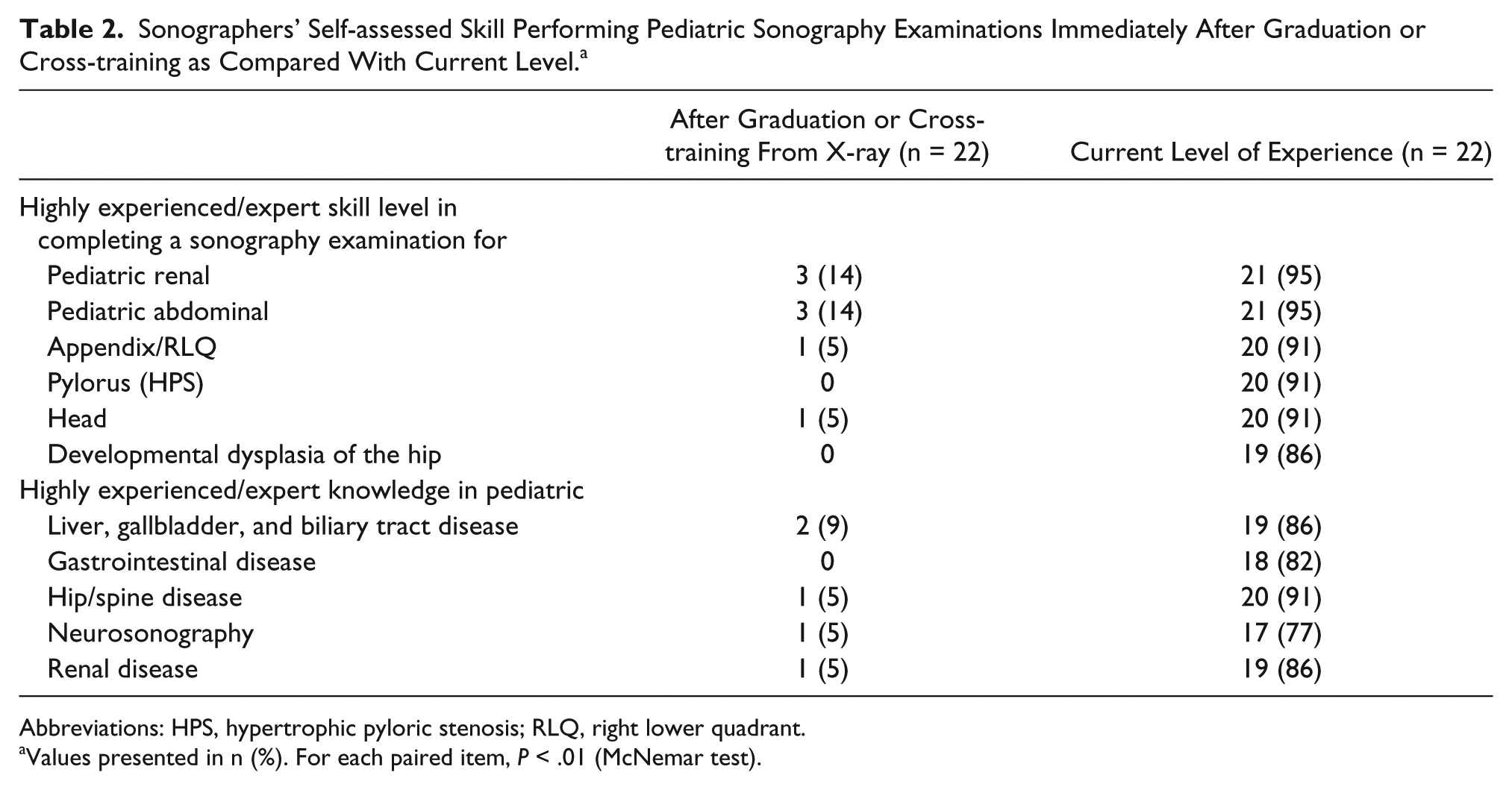
Abbreviations: HPS, hypertrophic pyloric stenosis; RLQ, right lower quadrant.
Values presented in n (%). For each paired item, P < .01 (McNemar test).
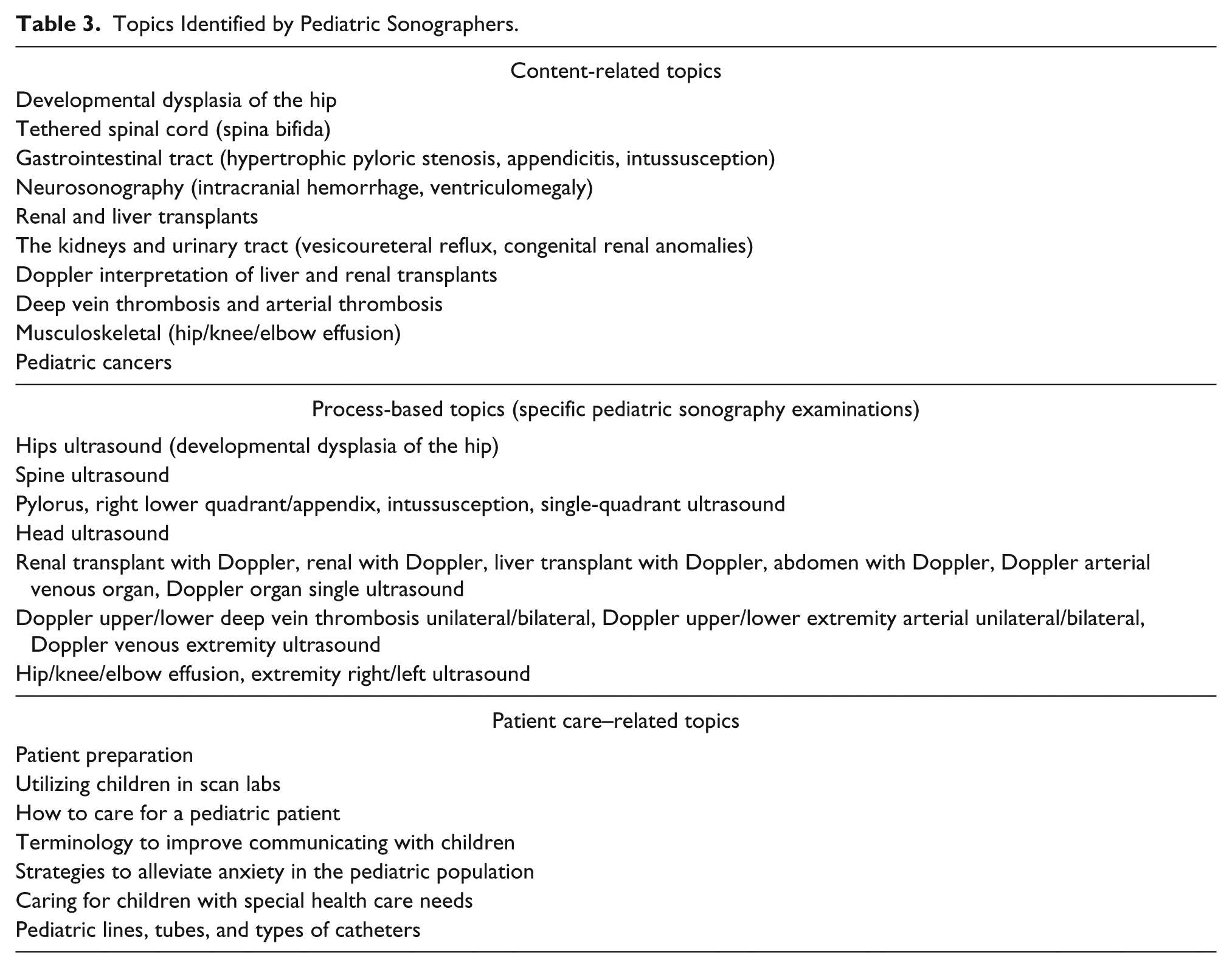
In the open-ended survey questions, participants indicated specific topics that may have been missing from their education or that would have made their transitions into pediatric sonography easier (Table 3). One sonographer stated, “More training specific to pediatric exams [is needed]. Pediatrics was only about two chapters in my entire curriculum.” Even an internally department cross-trained sonographer stated, “I felt my knowledge of diseases/diagnosis was lacking. I feel not being in the classroom atmosphere was somewhat detrimental in learning the many aspects of pediatric anomalies.” Another stated, “Little time was spent on pediatrics. . . . Most [time was] focused on adults. I learned the most from cross-training at the pediatric hospital.” A third cross-trained sonographer stated, “If I did not currently work (and receive extensive specific training upon my hire) at a pediatric facility, I would not feel competent performing any pediatric-specific exams.”
Topics Identified by Pediatric Sonographers.
Despite feeling that their pediatric sonography training curricula were lacking, a majority of survey participants reported little interest in taking a general pediatric specialty registry examination through the ARDMS (Table 1). Sonographers indicated that cost, lack of financial incentive, time studying, current recertification criteria, and continuing medical education certification were all barriers. Typical responses were “I don’t need the registry to prove my skill” and “I feel like I am already competent with my experience and I don’t need a registry to prove it.” Opposing responses included comments such as “[It] would be interesting to see how well I did” and “This ‘specialty’ has been long overlooked by the ARDMS. I feel this should have been instituted years ago. It would be interesting just to see how well I would do!”
Focus Group Results
Eleven sonographers participated in the focus group sessions, the majority having 5 to 10 years of pediatric sonography experience. Five themes emerged during the focus groups: (1) pediatric sonography material covered in school/program; (2) challenges caring for pediatric patients versus adults; (3) comparisons between adult and dedicated pediatric facilities; (4) the benefits and disadvantages of adding a pediatric sonography course, including topics that should be included; and (5) addition of the ARDMS pediatric sonography registry examination.
First, when sonographers were asked about their prior pediatric sonography education, the majority agreed that only a portion of necessary topics were covered and that they never learned how to scan a pediatric patient but, rather, just what an ultrasound image of disease processes would look like. One sonographer recalled, When we had our PowerPoint on pediatrics, it was pretty much just like here are the images, this is the spine, this is what you look for. But when you get [to a dedicated pediatric facility] the patients are [nil per os] a lot of the time and you don’t know, we’re going to feed them a bottle while they’re on their side while we’re scanning their hip. It’s just positioning and the way we scan pediatrics is so different than adults. Even if you had a little bit of knowledge before you came [to a dedicated pediatric facility] then listening and watching the techs, you would learn so much more.
Second, the participants mentioned, multiple times, the challenges of caring for pediatric patients and families as compared with adult patients. One sonographer commented, “One of the biggest battles with pediatrics is the kids. . . . My hardest part [to learn] was trying to get the kid to relax and be still. . . . Getting [a sonogram] on a kid that’s moving is hard.”
The third theme, comparing adult and dedicated pediatric facilities, focused on the specialization in pediatric facilities that made the training more intense. One newer employee explained, My challenges are just learning all the different types of pediatric scans. I already knew how to do a scan on an adult for kidneys but there are so many different anomalies associated with pediatrics, even with kidneys. There are just so many little things you have to learn that we don’t even hear of in the adult world. I had never heard of Mitrofanoff. . . . Learning the terminology alone and the abbreviations is a lot. I was more prepared for the adult world than pediatrics.
Another senior sonographer mentioned that more adult facilities have independent neonatal intensive care units and that the sonographers at these adult hospitals will have to scan these babies, “which they may not be comfortable scanning.”
The fourth theme centered on attitudes about a pediatric sonography course and topics for a dedicated course. Most sonographers stated that they learned more pediatric sonography from going to a pediatric clinical rotation than they did in school. Sonographers suggested incorporation of a hands-on scanning laboratory with pediatric models and pediatric experts facilitating the laboratory sessions. The sonographers also discussed the topics and amount of material required for a general pediatric sonography course, with some disagreement over whether there is enough material to create a dedicated pediatric sonography curriculum without too much overlap from other courses. Typical comments included the following: Hips, pylorus, spine, and, head . . . everything else you scan in adults. I don’t know if you have enough information for a 15/16 week course, [except] if the course covered neurosonography and how to work with kids, parents and pediatric disease processes. Anything you can get registered in, it should be taught in school. Education of lines and tubes would be very good; types of [pediatric] cancers, different types of catheters/tubes, certain transplants. You don’t deal with that kind of stuff in the adult world. This could all be a part of a pediatric course. Now I think that is beneficial! I think there needs to be patient care training in school. . . . I felt like I was not prepared for that when I went out into the real world.
By the conclusion of the discussion, the sonographers agreed that it is the responsibility of the schools to educate their students, although additional training from the workplace may be necessary. Consensus was reached that a semester-long pediatrics course with the topics discussed would be beneficial.
The fifth theme revolved around the creation of a pediatric sonography registry examination. This topic evoked high emotions and conflicting opinions, similar to those of the written survey. A number of sonographers were opposed to the examination: I’m not interested in studying for a test. I don’t want to study for it but it would be nice to be recognized that you do have this additional skill that not many other people have.
However, several sonographers were supportive of a pediatric sonography registry examination: I think it would be nice to have one because then I feel like I could be forced to study and know it. . . . A course or extensive training would be necessary before you took something like that. I think it would be great personally. I think it would really help get it all in your head so you’re prepared to start [working]. It would be a nice option. I think the idea is good, and students coming out now should have it as an option. You would have been forced to learn it, but if they’re going have [a registry examination], they have to teach it more in school.
Discussion
This mixed-methods study revealed that experienced pediatric sonographers self-assess that they had significantly increased their knowledge, skill, and competence since graduation or cross-training. Many of these experienced sonographers now consider themselves experts, but they assessed their pediatric sonography skills at a novice level immediately after graduation/cross-training, suggesting that much of their pediatric training occurred while working at a dedicated pediatric facility. This implies that the amount of training and clinical experience on these topics may not be adequate during a diagnostic medical sonography educational program.
The accuracy of pediatric sonography improves with greater sonographer training and close cooperation with radiologists and clinicians. 21 Expanded standardized training may lead to improved patient safety by improving examination quality and by increasing confidence in both positive and negative sonographic findings. 21 The high percentage of responses to the 2012 ARDMS needs assessment suggested that sonographers and other medical professionals would accept more pediatric sonography education and value a new credentialing examination 16 ; this led to the development of a specialized pediatric sonography registry examination, implemented in February 2015. This new registry may promote increased support for pediatric sonography courses as part of diagnostic medical sonography curricula to better prepare sonographers, which ARDMS-registered medical professionals and members of the Society for Pediatric Radiology believe may lead to improved patient care. 16
Over time, employment at a pediatric institution can rectify deficiencies in pediatric sonography education if hands-on training is provided. However, most pediatric sonograms occur in nonpediatric facilities and are done by sonographers that possibly have not had pediatric sonography–specific training, creating potential for errors and safety concerns. During the focus groups, experienced pediatric sonographers recommended content, process, and patient care topics that could be included in a future standardized pediatric sonography curriculum. Since current accredited diagnostic medical sonography programs may not provide their students with the opportunity to scan pediatric patients or learn pediatric disease processes, these same students will be required to scan pediatric patients during their careers; as such, implementation of a standardized pediatric sonography curriculum is critical.
Sonographers had mixed attitudes and opinions regarding implementation of a pediatric sonography examination. A majority of the pediatric sonographers were not in favor of an additional registry for pediatric sonography, mainly due to time commitments, but many believed that it could be helpful for new graduates. However, sonographers would be more inclined to take a pediatric sonography registry examination if financial incentives were attached.
Limitations
This study has several limitations. First, it was performed at a large, busy pediatric academic hospital with a limited number of participants, which may limit generalizability of the data. Second, the quantitative data were derived from a nonvalidated survey. Additionally, participants self-assessed their knowledge, skills, and competence, which may not reflect true values. This limitation was adjusted by use of an anchored-scale response, with specific verbiage to delineate the qualifications of each level. Third, the principal investigator performed the qualitative data collection alone, which could create some biases. However, all focus groups were recorded and reviewed by three researchers to attempt to minimize this bias. Fourth, since the principal investigator works in the same Department of Radiology as the respondents, sonographers may have altered their responses or felt less comfortable openly discussing their perspectives. The researchers tried to minimize this effect with voluntary participation, anonymizing the comments and not linking these results in any way to their job evaluations.
Future Directions
Future studies with pediatric sonographers from a variety of pediatric and nonpediatric institutions, as well as students currently enrolled in accredited diagnostic medical sonography programs, would improve the generalizability of these results. Comparison of self-assessed competence to manager-reported competence could delineate topics that require additional focus. These perspectives could be beneficial in building a comprehensive pediatric sonography curriculum that targets the necessary knowledge, skills, and attitudes to improve competence in performing pediatric sonography examinations upon completion of a diagnostic medical sonography–approved program.
Conclusion
Additional pediatric sonography education in diagnostic medical sonography curricula is essential for improving the knowledge, skills, and competence necessary for new graduates to correctly perform pediatric sonography examinations. Creating a standardized pediatric sonography course could minimize performance gaps that have historically been remedied with experience in a pediatric institution, with all the built-in fallacies of on-the-job training. The detailed qualitative information may serve as a framework to shape the necessary curricular topics and techniques. Although this may extend pediatric sonography education, the improved competence of pediatric sonographers after training may positively affect diagnostic accuracy and patient safety, which may be particularly important in nonpediatric facilities.
Footnotes
Appendix: Focus Group Prompts
Acknowledgements
We thank Marilyn Goske, MD, Tracey Adams, RDMS, the ultrasound department at the Cincinnati Children’s Hospital Medical Center, Michael E. Hekler, DC, and Jeanette I. Robinson for their motivational support. This research was presented as a final project for the corresponding author’s master in education degree.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.