
Abstract
This is a case study of Jarcho-Levin syndrome, which is a rare genetic disorder described as a malformation of bones in the spinal column and the ribs. This disorder can be an autosomal recessive or dominant trait. Those affected by this disorder have respiratory insufficiency and potentially other abnormalities. Recurrent respiratory infections are expected. In milder cases, surgery is a possibility, but in severe cases, prognosis is poor. OB sonography can aid in diagnosis of Jarcho-Levin syndrome in patients with no known family history of the disease, but it is particularly helpful in known at-risk cases.
Introduction
This syndrome was named for Saul Jarcho and Paul Levin, 1 who first described it in 1938. Jarcho-Levin syndrome is a rare genetic disorder characterized by malformation of bones in the spinal column and ribs. Jarcho-Levin syndrome may be detected prenatally by routine sonogram in both at-risk families and families with no known history. The earliest reported case of Jarcho-Levin syndrome using prenatal transvaginal sonography was at 12 weeks gestation, in a patient with a known family history of the disorder. 2 Advances in sonographic equipment are making it easier for sonographers to detect signs of this syndrome earlier in pregnancy. Criteria for diagnosing Jarcho-Levin syndrome include costovertebral segmentation defect, indistinct or fused posterior ribs, irregularly shortened spine, and short trunk and neck, 3 found alongside normal amniotic fluid, limb length, and biparietal diameter. 4 Other names for Jarcho-Levin syndrome are costovertebral segmentation anomalies, spondylocostal dysostosis or dysplasia, spondylothoracic dysostosis or dysplasia, and occipito-facial-cervico-thoracic-abdomino-digital dysplasia. 2 The terms spondylothoracic dysostosis and spondylocostal dysostosis are most often used to describe this phenomenon. These are two different types of Jarcho-Levin syndrome, which are described below.
Case Report
A 26-year-old Hispanic patient, G3P1, presented for a fetal anatomy survey at 19 weeks 4 days gestation. Indications for the examination were known fetal anomalies. In the prior examination, the fetus presented with a thickened nuchal fold and a short irregular spine, and the fetal heart was not well visualized.
Sonography of the fetal anatomy was performed with a Siemens Acuson S2000 (Siemens Ultrasound, Mountain View, CA). Biometry was adequate for gestational age. The evaluation of the heart revealed normal situs, rate, and rhythm. Both outflow tracts appeared to arise from the right ventricle, the great vessels appeared malposed, and a large ventricular septal defect was noted. The fetal spine was short and contained multiple abnormal curvatures suggestive of segmentation-fusion defects (Figure 1). Although the fetal spine appeared significantly foreshortened, the sacral spine was present. The fetal neck and thorax appeared abnormally small (Figures 2, 3) and compressed with short, flared ribs (Figures 4, 5). Figure 6 shows asymmetrical clavicles and a transverse view of the spine. The long bones were normal in size and appearance (Figure 7). Femur length to abdominal circumference ratio was 20, which was within normal limits for gestational age. A normal femur length to abdominal circumference ratio is 22 ± 2. 5 The amniotic fluid volume was normal with a deepest pocket measurement of 5.1 cm. Two umbilical arteries were noted. The mother was counseled about the findings regarding the high suspicion of an underlying genetic syndrome and the concern for incomplete lung development given the small thoracic size. The mother was offered amniocentesis, which was declined.

Sonogram demonstrating a shortened spine with abnormal curvature.

In this view of the fetal profile, the neck and thorax appear abnormally small.

Longitudinal view of the diaphragm where the difference between the thorax and the abdomen may be observed.

The ribs appear short and flared in this view of the fetal chest.

Transverse image of the ribs, which appear abnormal.

Transverse image of the spine and asymmetrical clavicles.
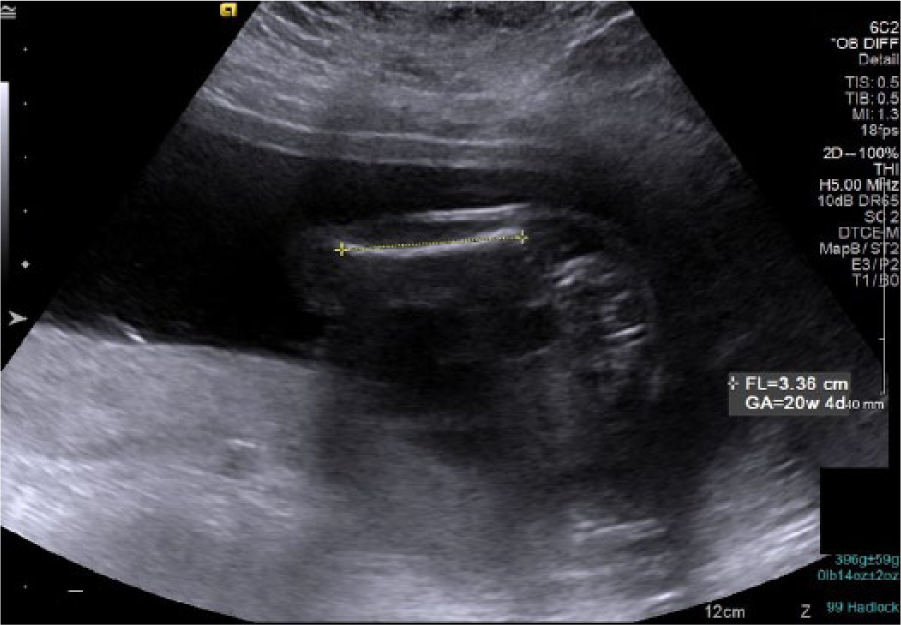
Sonographic view demonstrating a fetal long bone measurement in the normal range for gestational age.
No new findings were noted on subsequent examinations. At 33 weeks gestation, oligohydramnios was discovered. After a short hospital stay, the infant was born at 34 weeks with an Apgar score of only 1 after 1 minute. The infant expired shortly after delivery. A fetalgram, which is a radiograph demonstrating the entire newborn on one radiographic image, was performed and showed seven ribs on the left and five on the right (Figure 8). Physician notes attached to this case stated, “suggestive of Jarcho-Levin syndrome.”

Fetalgram demonstrating seven ribs on the left and five on the right.
Discussion
Jarcho-Levin syndrome has been reported as 1 in 40 000 births globally. 6 It occurs with equal frequency in males and females. 2 Jarcho-Levin is caused by a gene mutation inherited as an autosomal recessive or autosomal dominant trait.4,7 According to the National Organization for Rare Disorders, genes that have been connected to this disorder include the DLL3 gene located on chromosome 19 at 19q13 and MESP2 gene located on chromosome 15 at 15q26.13.3,8 In autosomal recessive cases, the individual with Jarcho-Levin syndrome inherited the abnormal gene from both parents, who are carriers. The risk for two parents who are carriers of the defective gene to pass Jarcho-Levin syndrome on to their offspring is 25% with each pregnancy. The incidence tends to be higher in consanguineous relationships. 9 In autosomal dominant cases, the individual with Jarcho-Levin syndrome inherits the abnormal gene from one parent who is a carrier. In this case, there is a 50% risk of Jarcho-Levin syndrome with each pregnancy. Screening examinations, such as cell-free fetal DNA, detect genetic abnormalities such as trisomies 13, 18, and 21. 10 Due to the lack of a clear genetic marker, there is no specific prenatal genetic test presently available for the diagnosis of Jarcho-Levin syndrome. 2
Spondylothoracic dysostosis (STD) is an autosomal recessive form of the disorder. 3 It occurs in all races but has a higher incidence in people of Spanish heritage, Puerto Rican in particular.11,12 Neonates present with vertebral segmentation and formation defects throughout the spine. This disorder is characterized by fanned-out ribs from fused thoracic vertebral bodies. The prognosis is poor. Spondylocostal dysostosis (SCD) is a milder form of Jarcho-Levin syndrome and may be more difficult to diagnose in utero. It is autosomal dominant or recessive and occurs more often in people of European descent. 12 SCD is characterized by vertebral and intrinsic costal anomalies 3 ; however, unlike STD, there is no flaring of ribs.
Although a radiograph may be used to diagnose Jarcho-Levin syndrome 2 postdelivery, sonography is the primary method of prenatal diagnosis. Since there is no genetic test available to diagnose STD or SCD, many times the final diagnosis is not made until after birth. In India, Kulkarni et al. 4 noted two cases that were diagnosed postnatally. Wong and Levine 12 reported on a Puerto Rican couple who had two consecutive pregnancies diagnosed prenatally via sonogram with Jarcho-Levin syndrome. Although there was no family history of dwarfism, abnormalities were noted sonographically. Another sonogram was ordered for further assessment, much like the current case. Also similar, biometry and long bones were normal alongside a short irregular spine. The second pregnancy 10 months later presented with analogous abnormalities. Cuillier et al. 2 likewise detailed a case where a prenatal sonogram identified abnormal curvature of the spine with the ribs flaring in a “crab-like fashion” alongside normal limbs and a shortened thorax. There was no familial history; the prior maternal serum screening for alpha-fetoprotein, hCG, and UE3 was unremarkable; and chromosome analysis from an amniocentesis showed a normal karyotype.
Sonographic criteria for detecting STD include unpaired or poorly formed vertebrae, indistinct or fused posterior ribs, irregularly shortened spine, curvature of the spine caused by hemivertebrae, 13 and a short trunk and neck, found alongside normal amniotic fluid, limb length, and biparietal diameter. 4 Associated anomalies include minor facial dysmorphism, urogenital and anal anomalies, congenital heart disease, limb and digit anomalies, 4 a single umbilical artery, 14 and an increased fetal nuchal translucency thickness. 15 Jarcho-Levin syndrome may also be associated with neural tube defects, such as spina bifida. 16
Differential diagnosis for Jarcho-Levin includes dyssegmental dysplasia,2,12 a short-limbed dwarfism presenting with vertebral segmentation defects, and spondylo-epiphyseal dysplasia,2,12 which has flattening of vertebrae. With this disorder, extremities may or may not be shortened and the thorax is bell-shaped, but the crab-like morphology of the ribs is lacking. 2 Costovertebral segmentation defects with mesomelia2, 12 are also a feasible differential; these have hemivertebrae, vertebral fusion, and butterfly vertebrae.
Prognosis for Jarcho-Levin syndrome mainly depends on the severity of the disease. In its severe form, the prognosis is grim. The chest is too small to accommodate growing lungs, which compromises the respiratory system 17 and leads to recurrent life-threatening bouts of pneumonia. In these cases, death occurs either neonatally or within the 1st year of life. Thanks to medical advancements, the mild form of the disease, SCD, has a better prognosis, which improves even further if the infant survives beyond 6 months. 18
A treatment to consider postnatally if the infant survives is the vertical expandable prosthetic titanium rib (VEPTR). 19 Dr Karlin and associates have published in The Journal of Bone & Joint Surgery that the VEPTR was created to treat thoracic insufficiency syndrome in pediatric patients. Approved in 2004 by the US Food and Drug Administration, the VEPTR is a device that is implanted and can expand to help straighten the spine and separate ribs so that the lungs can grow and expand. The device is adjustable to grow with the patient.
Conclusion
Jarcho-Levin syndrome is a rare genetic disorder characterized by malformation of bones in the spinal column and the ribs. Spondylothoracic dysostosis and spondylocostal dysostosis are two different types of Jarcho-Levin syndrome.
Many of the physical traits associated with Jarcho-Levin syndrome can be detected in utero with obstetric sonography. Sonographic criteria for Jarcho-Levin syndrome include costovertebral segmentation defect, indistinct or fused posterior ribs, irregularly shortened spine, and short trunk and neck, 3 found alongside normal amniotic fluid, limb length, and biparietal diameter. 4 Infants affected by this disorder have respiratory insufficiency, and other abnormalities such as recurrent respiratory infections are expected. In milder cases, surgery including the VEPTR is a possibility, but in severe cases, prognosis is poor. Since this disorder can be an autosomal recessive or dominant trait, parents in this situation need genetic counseling to be aware of how this could affect future pregnancies.
Footnotes
Acknowledgements
The author thanks Michael Davidson and Parkland Hospital for this case. The author also thanks Michael Davidson for his advice, guidance, and support in writing this article.
Declaration of Conflicting Interest
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.