
Abstract
Leiomyomas of the kidney are rare, mostly occurring in adults as incidental findings, and are a diagnostic challenge. In a renal transplant recipient population, an increased risk of tumors is observed due to the effect of immunosuppressive drugs. A differential diagnosis between leiomyomas and other malignant lesions is not possible with current imaging methods. This report presents a case of a native kidney capsular leiomyoma in a kidney transplant recipient and highlights the features of computed tomography and contrast-enhanced ultrasound (CEUS), along with the histopathologic analysis. The CEUS and quantification studies are helpful in demonstrating the vascularization pattern of the renal capsular leiomyoma. This entity appearing with chronic kidney disease can resemble a renal cell carcinoma, in an otherwise healthy kidney. In this case, CEUS was useful for diagnosing the vascularization of the renal mass, although the pattern of intense vascularization could be diagnostically misleading, implying a malignant lesion. However, the pattern of enhancement due to CEUS showed no peculiarities that indicated histopathologic diagnosis.
Leiomyomas are benign tumors that can originate from any smooth muscle-containing structure. The renal capsule is the most common targeted site of involvement, even though renal leiomyomas can arise from smooth muscle cells in the calyx, renal pelvis, or blood vessels. Leiomyomas of the kidney are rare, mostly occurring in adults as incidental findings, and are a diagnostic challenge. The incidence at autopsy has been reported to be 4% to 5.5%,1–3 and a cortical nodule discovered at autopsy has been found to have a 14% chance of being a pure leiomyoma. 1 Differential diagnosis between leiomyomas and other malignant lesions is not possible with current imaging methods like computed tomography (CT), magnetic resonance imaging (MRI), or the more recently investigated contrast-enhanced ultrasound (CEUS) but only with a histopathologic examination. Renal transplant can present as a clinical situation in which immunosuppressive therapy increases the risk of developing cancer. 4 Therefore, in renal transplant recipients, the presence of a mass identified by imaging methods in a native or transplanted kidney must certainly raise the concern of a malignant lesion. The case presented is a study of a renal capsular leiomyoma, which may be the first reported in a renal transplant recipient. In addition, the imaging features with CEUS are provided.
Case Report
A lean, 24-year-old woman with chronic renal failure secondary to chronic pyelonephritis received a renal transplant from her brother, a 30- year-old male living donor. It was a haploidentical transplantation, regarding human leucocyte antigen compatibility. Posttransplant recovery was good with immediate graft function and no need for dialysis. There was no induction therapy. Maintenance immunosuppression consisted of steroids, cyclosporine, and azathioprine. Six days after renal transplantation, the patient was discharged with serum creatinine equal to 1.1 mg/dL. During the late posttransplant period, she did not require dialysis support, presenting stable creatinine (0.8–1.2 mg/dL) in most queries.
Then, 27 years after kidney transplantation, during a routine sonogram, a nodule was discovered in the native right kidney. Sonography was conducted using a 3.5 MHz convex transducer (Aplio 400; Toshiba, Tokyo, Japan), which demonstrated a 4-cm, well-defined isoechoic mass protruding outward from the superior pole of the right native kidney (Figure 1). Urinalysis revealed no microscopic hematuria and serum creatinine was normal. Physical examination on admission revealed no palpable masses.
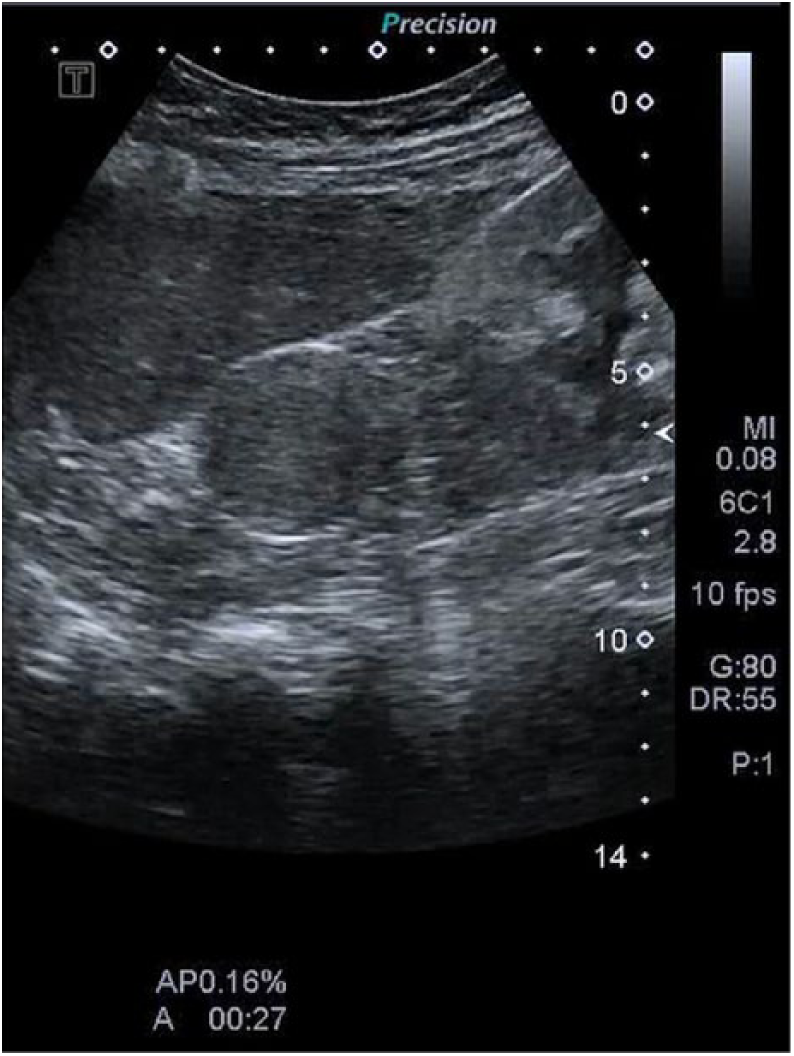
Sonographic image of a well-defined mass in the upper pole of the right kidney.
Computed tomography revealed an approximately 3-cm-diameter, encapsulated, heterogeneously enhanced lesion in relation to the lateral aspect of the right native kidney, which was displaced medially and inferiorly by the tumor (Figure 2). There was no evidence of abdominal lymphadenopathy or involvement of the renal vasculature.
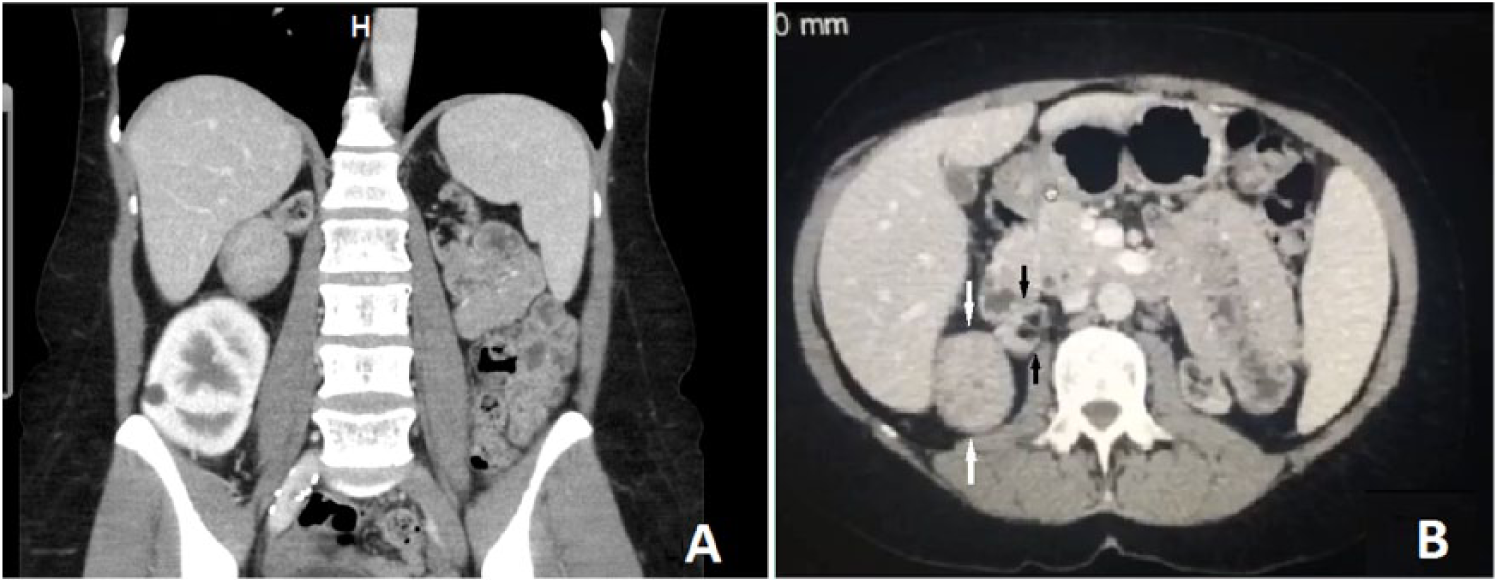
Computed tomography image of abdomen/pelvis. (A) Coronal section shows an exophytic mass with heterogeneous contrast uptake located between the liver and the transplanted kidney. (B) Axial section shows exophytic mass (white arrows) originating from atrophic right native kidney (black arrows).
To better depict the mass, 2 weeks later, CEUS was performed with an intravenous bolus injection of 2.4 mL of Sonovue® (Bracco International, Milan, Italy), followed by 5 mL of saline solution. The examination was performed using contrast harmonic imaging at a low mechanical index of 1.0. The examination was documented by digitally storing the images over 60 seconds in DICOM format. After contrast medium injection, the mass was found to be homogeneously enhanced and showed a well-defined edge and wash-in phase (Figure 3). Wash-out phase findings were not relevant for diagnosis. There were no adverse reactions to contrast administration.
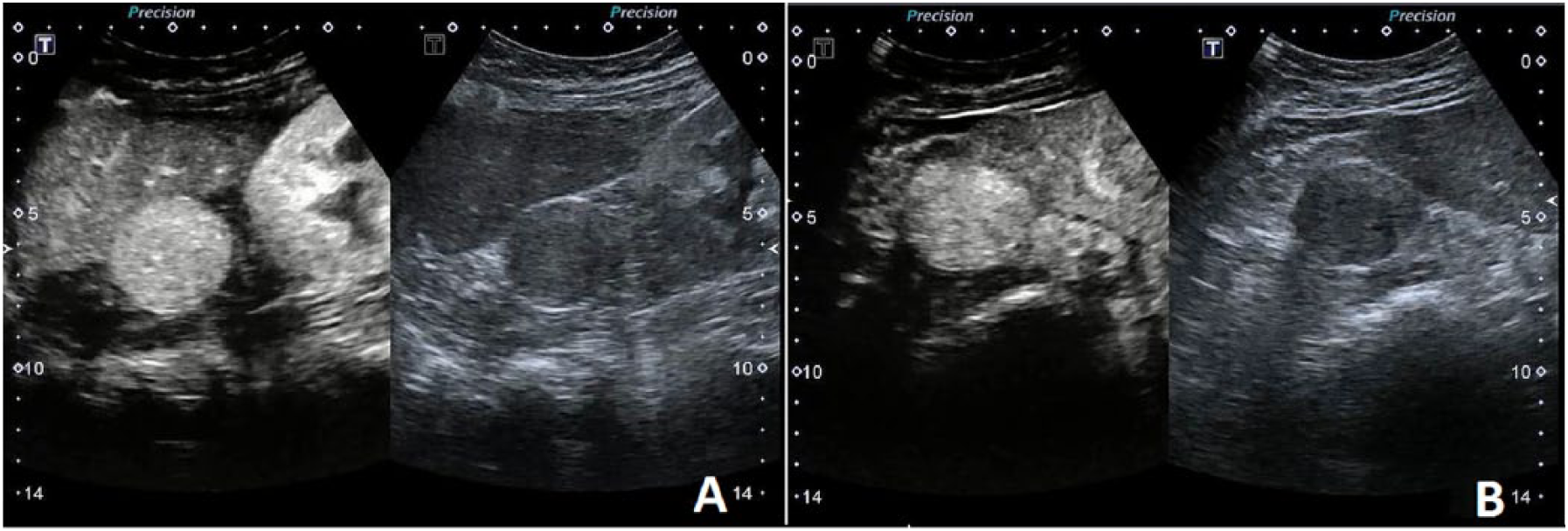
Contrast-enhanced ultrasound image. (A) Longitudinal section shows an exophytic mass with homogeneous contrast uptake located between the liver and the transplanted kidney. (B) Axial section shows exophytic mass originating from right native kidney.
Quantitative analysis with the time-intensity curve was used to calculate the amount of enhancement in the mass, native kidney, liver, and renal graft. Accordingly, in the arterial phase, the mass was considered hypervascular (3.80 intensity units) in relation to the liver (1.20 intensity units) and to the native kidney (1.17 intensity units) and hypovascular in relation to the kidney graft (6.90 intensity units) (Figure 4).
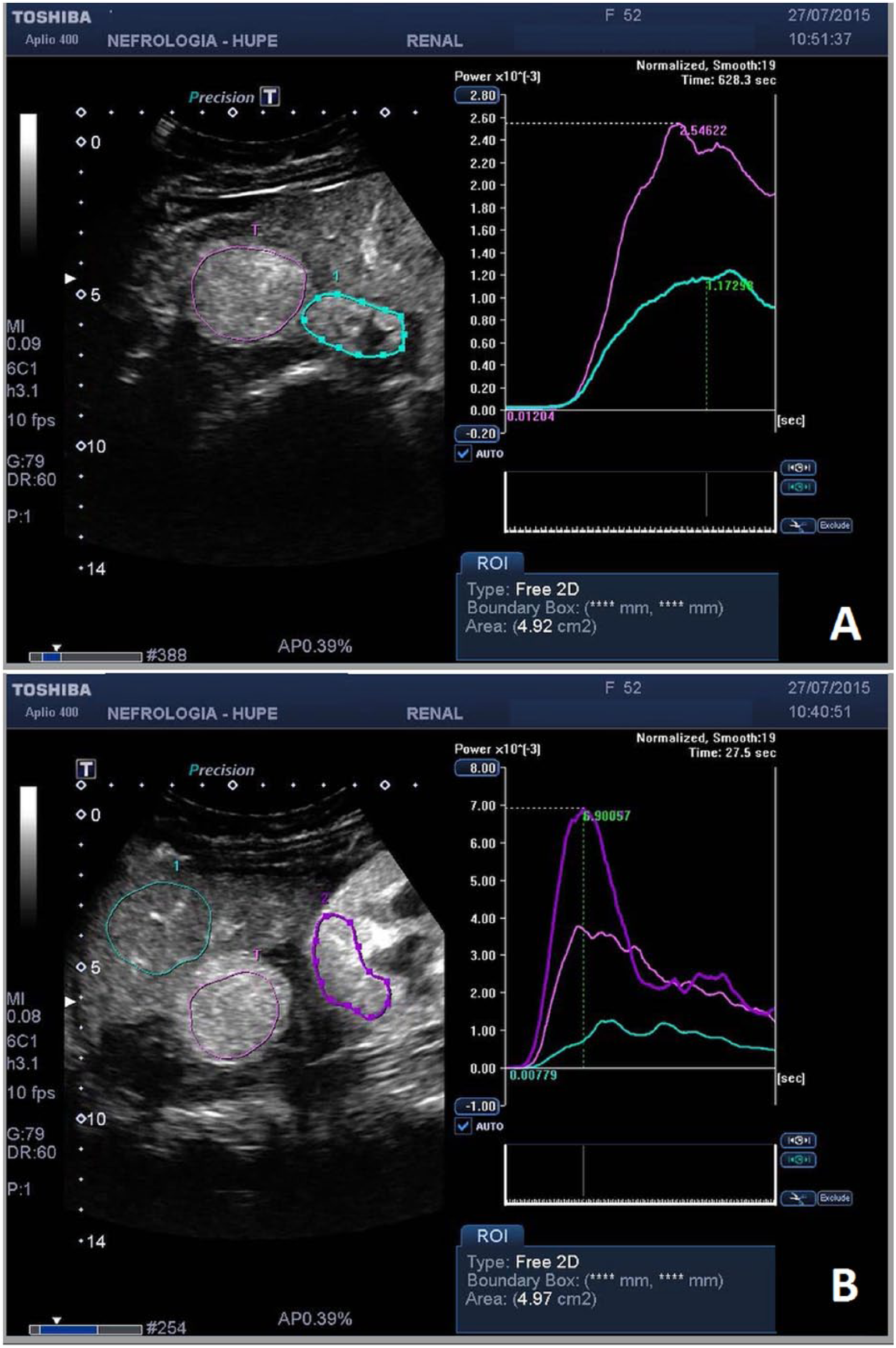
Contrast enhancement by the tumor (pink line) is higher in relation to the native kidney (green line) (A) and in relation to the liver (green line) and lower in relation to the transplanted kidney (purple line) (B). Contrast enhancement pattern mirrors vascular supply of the region.
To rule out the possibility of renal cell carcinoma (RCC), the patient underwent right radical nephrectomy.
During the operation, a firm, well-circumscribed whitish-tan solid tumor, measuring 3 cm and easily mobilized from the surrounding tissues, was found. The mass did not involve the kidney parenchyma itself but was seen adherent to the renal capsule at the superior pole of the right kidney. On the cut surface, no calcific lesions were noted. Microscopic sections disclosed a mass of smooth muscle tissue arranged in whirls and cords. No mitotic figures were seen. Pathologic diagnosis was a benign renal capsular leiomyoma (Figure 5). There was no evidence of recurrence 1 year after the surgery.
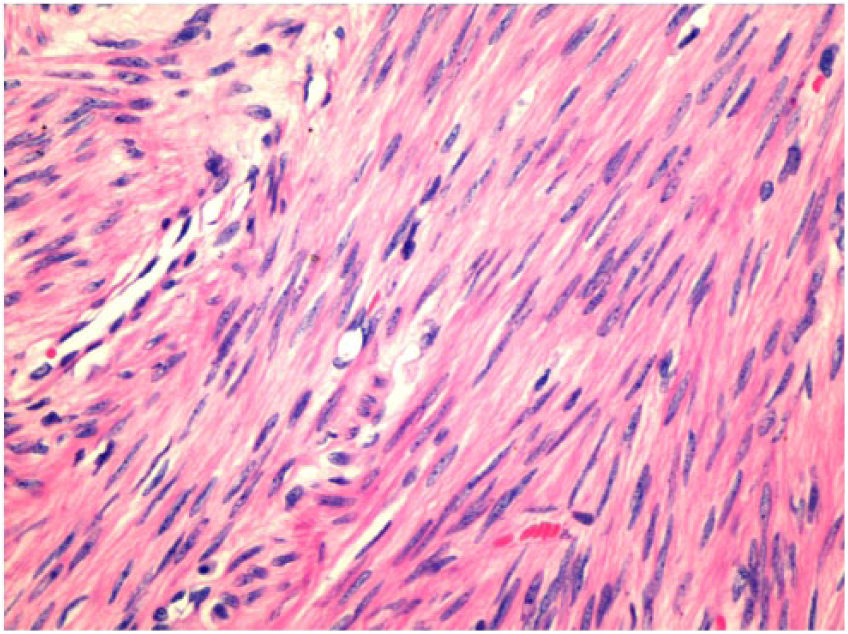
Histopathologic features of leiomyoma. Neoplastic smooth muscle cells without atypia or mitosis, which suggest a benign tumor (hematoxylin and eosin, 390×).
Because CEUS was being performed in our facility as clinical research, the ethics committee approved the study per local legal requirements and informed consent was obtained.
Discussion
Recipients of kidney transplants are more likely to develop neoplasms due to the requirement of continuous immunosuppression therapy to avoid rejection. The risk of malignancy in solid organ recipients is 2 to 4 times greater4–8 than in the general population. Therefore, the surveillance of these patients should be intensive.
In a study that evaluated approximately 1000 nephrectomies performed as a result of kidney tumors, renal leiomyomas were only 0.3% of all lesions and 1.5% of benign tumors, 9 affecting the renal capsule in approximately 15% of cases. 10 The prognosis after resection of these benign tumors is excellent.1,2
The condition is more common in female and in middle-age patients. More than 90% of cases occur in patients older than 20 years, 1 who are usually asymptomatic. If clinically evident, flank or abdominal pain (53%), associated (33%) or not with a palpable mass (57%), is the most common presentation. Frank hematuria can be present in 20% of cases. 11 Establishing a discrete clinical picture in an asymptomatic patient represents a challenge to the medical team. The main goal of imaging renal tumors is therefore to differentiate malignant from benign tumors. Although recent advances in imaging technology have resulted in the detection of incidental renal masses in seemingly asymptomatic patients, none of the currently available imaging modalities can accurately predict the histology of a given renal mass.
There is some diversity of features in imaging diagnosis. Although cystic features like posterior enhancement in mixomatous degeneration 12 and even well-defined cystic lesion appearances in large renal leiomyoma 13 have been reported, the usual findings on ultrasonography are hypoechoic and heterogeneous solid masses.10,14 Features on a CT examination that can be useful in diagnosis are an exophytic, sharply marginated, low-density lesion and no evidence of extrarenal invasion. 1
Ultrasound contrast agents, such as microbubbles, are an important and complementary tool in sonography studies, as they show a clear distribution of the vascular bed. The assessment of microvascular perfusion using time-intensity curves may also be promising in many yet unknown applications.15,16
Contrast-enhanced ultrasound can be useful in the diagnosis of pyelonephritis, vascular complications, cystic lesion, kidney tumors, and pseudotumors. It has also been used to evaluate kidney allografts. 16 In this clinical setting, CEUS is a safe and excellent method for assessing focal lesions and can be used in the diagnosis of renal infarction 17 as well as pseudoaneurysm. 18 In this case, CEUS was useful for diagnosis and evaluation of the renal mass vascularization.
This case is typical of the usual presentation. The patient was a middle-age woman and a renal leiomyoma was found incidentally. The mass was well defined, appeared hypoechoic and solid, and was slightly lower in echogenicity than the adjacent renal cortex with gray-scale sonography. In addition, it appeared slightly hyperdense compared with the kidney, with a similar density to that of muscles before contrast injection, and became hypodense compared with the renal cortex after contrast injection on CT examination.
Despite the availability of advanced imaging methods, the conclusive method still relies on histopathologic evaluation for a reliable diagnosis.1,19,20 To rule out infection, necrosis, or malignancy risk, radical nephrectomy is usually indicated, especially for large leiomyomas. 21
The quantitative analysis in this case showed that the mass was hypervascular in relation to the native kidney parenchyma and hypovascular in relation to the kidney graft. Given that guidelines from urologic associations always include CT evaluation of renal masses, we compare CEUS features with those of CT. Based on data reported in the literature, it is well known that enhancement of renal tumors has a different pattern according to renal function: RCCs are characteristically well vascularized in comparison with the renal parenchymal vascular sclerosis in chronic kidney disease, 22 and leiomyomas in patients with normal kidney function are less vascularized than the renal parenchyma,23,24 quite the opposite pattern from that observed in this case using CEUS.
It follows from this case report and the remarks above that it is reasonable to speculate that in chronic kidney disease, the vascularization imaging features of the leiomyoma by CEUS may suggest that of the RCCs by CT. According to current knowledge, the radiologic features of renal leiomyoma by means of CEUS have not been previously reported in the literature.
Nonetheless, since the hypervascular pattern observed in the present case has also been reported in RCCs, 25 the differentiation of leiomyoma from RCC, using CEUS, might be difficult because of overlap of imaging features.
We speculate in this report that the tumor had a higher enhancement than the adjacent renal parenchyma due to the differing vascularization of the two territories. Whereas renal parenchyma is fed by the renal artery, which in this case should be atrophic secondary to long-term renal insufficiency, the renal capsule receives blood from a more robust vascular supply. A vascular bed that includes anastomosis with suprarenal and gonadal arteries would probably compensate for the compromised blood flow from the interlobar artery.
In summary, although establishing the diagnosis of renal tumors is difficult based on imaging, when confronted with the possibility of an exophytic renal tumor, the CEUS and quantification studies may be helpful to show that the vascularization pattern of renal leiomyoma in chronic kidney disease resembles that of the RCCs in an otherwise healthy kidney. In this case, CEUS was useful for diagnosis of the vascularization of the renal mass, although the pattern of intense vascularization could mislead an early judgment as a malignant lesion. However, the pattern of enhancement due to ultrasound contrast showed no peculiarities that pointed to the histopathologic diagnosis.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support was received in part via Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ). Bracco (Milan, Italy) provided the contrast agent (Sonovue) free of charge.