
Abstract
Necrotizing fasciitis is a rare, life-threatening, flesh-eating bacterial infection that quickly destroys soft tissue beneath the skin. Left untreated, it can result in the loss of limbs or even death. A diagnosis is most often made through laboratory tests and diagnostic imaging such as magnetic resonance imaging, computed tomography (CT), and sonography. This case study demonstrates the use of sonography to assist in the detection and characterization of necrotizing fasciitis. In this case, CT provided the necessary diagnostic information to accurately diagnose necrotizing fasciitis. The prompt diagnosis for this patient facilitated expedited treatment in an effort to stem progressive damage to the affected limb.
Introduction
Necrotizing fasciitis (NF) is a rare bacterial infection involving the subcutaneous tissue and fascia, commonly caused by group A streptococcus (GAS). Since 2010, approximately 700 to 1100 cases of necrotizing fasciitis caused by GAS are reported each year. 1 However, the actual incidence of NF is currently nearly impossible to determine as less common cases caused by various other types of bacteria are not tracked. 1 Necrotizing fasciitis has a relatively high mortality rate that may be attributed to the rapid progression of fascial necrosis that is linked to the disease.2–4 The median mortality rate is 32.2%, and the prognosis is especially poor if the patient has two of the most common comorbidities: diabetes mellitus and/or immunosuppression.2–4 In patients presenting with pain greater than would be expected with the clinical findings, NF should be considered as a part of the differential diagnosis in addition to more common findings such as cellulitis or abscess.5–7 Rapid diagnosis and management of the condition is vital to reduce the patient’s morbidity and mortality. In this particular case, sonography was used in the initial detection of the NF, and the use of computed tomography (CT) provided added global visualization of the infection and the involved tissues. This multimodality approach helped to confirm the diagnosis of NF in this patient.
Case Report
A 53-year-old Caucasian male with a history of cellulitis was admitted to the hospital for redness, pain, and swelling of his left lower extremity, most notably in the area of the thigh. The patient provided a history of tachycardia and hypertension. He also reported a recent minor insect bite on his left thigh. The afebrile patient was admitted with an elevated white blood cell (WBC) count of 14.7 cells per liter and was immediately placed on intravenous (IV) antibiotics. Little improvement was demonstrated after several days of IV vancomycin treatment, therefore a sonogram of the area of interest was ordered to rule out abscess.
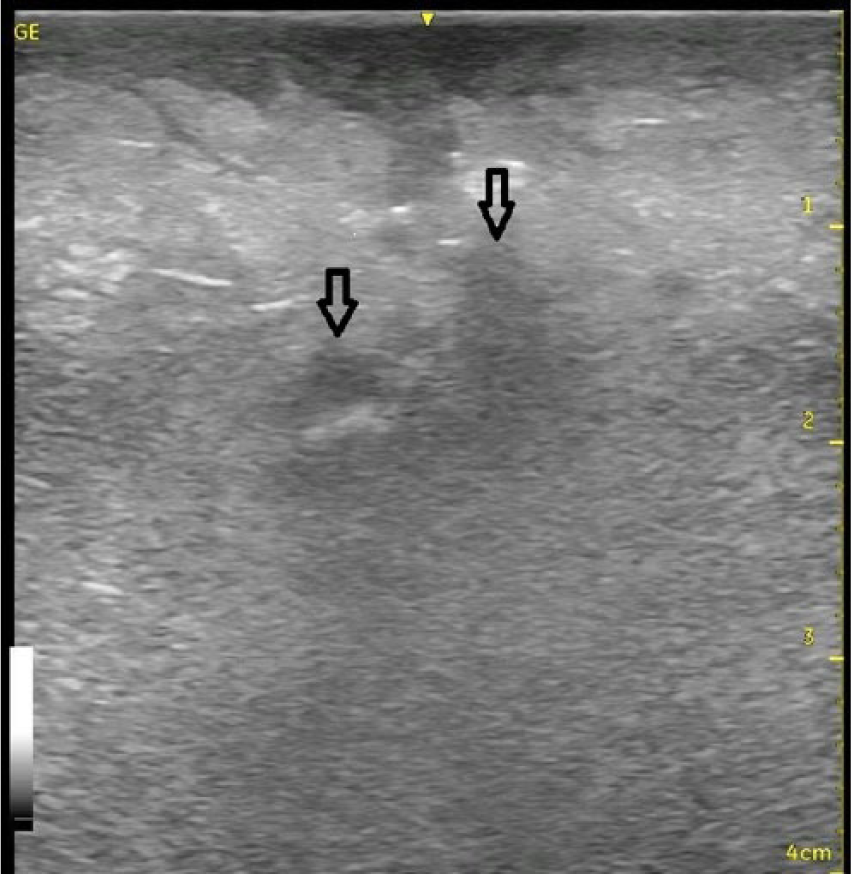
A targeted sonogram of the superficial left lower extremity was performed using a GE Venue 40 ultrasound machine with a 12 MHz linear array transducer (GE Healthcare, Waukesha, Wisconsin). Sonographic evaluation of the left inner thigh demonstrated no evidence of focal abscess. Rather, the fascial and subcutaneous tissue appeared markedly thickened and echogenic (Figure 1). A “cobblestone” appearance was demonstrated approximately 1.0 cm beneath the skin, along the margin of the subcutaneous layer. Abnormal hypoechoic fluid accumulation was visualized in the deep fascia and subcutaneous layers, surrounded by echogenic fat and connective tissue (Figures 2 and 3). Color Doppler evaluation did not reveal hypervascularity within or surrounding the edematous tissue. There was limited visualization of the muscular layer of the thigh due to patient body habitus. Based on these sonographic findings, NF or some other soft tissue infectious process was suspected. A CT examination was recommended to further characterize the infection and confirm this suspected diagnosis.
Longitudinal gray-scale sonogram of the left inner thigh showing edematous fascial and subcutaneous layers as markedly thickened and echogenic tissue.

Longitudinal gray-scale sonogram of the left inner thigh showing the “cobblestone” appearance with hypoechoic fluid accumulation (arrows) within the deep fascia and subcutaneous layers, surrounded by echogenic fat and connective tissue.
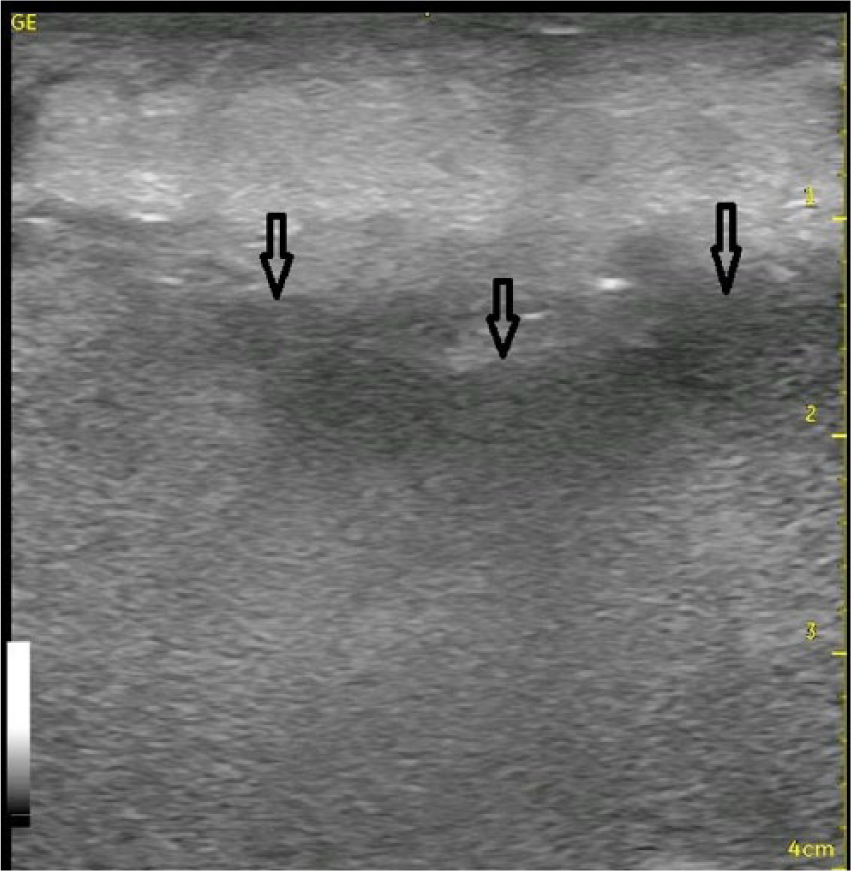
Longitudinal gray-scale sonogram of the left inner thigh showing edematous echogenic subcutaneous tissue and abnormal hypoechoic fluid accumulation (arrows) within the deep fascia.
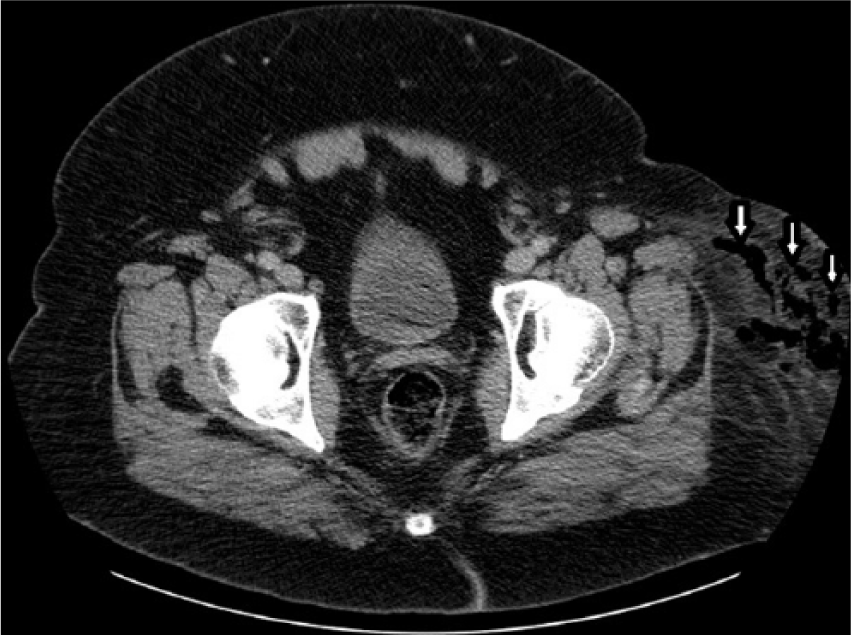
A pelvic and bilateral lower extremity CT without contrast was performed. The CT demonstrated soft tissue edema throughout the region of the thigh in the left lower extremity. Coronal views of the lower extremities demonstrated extensive edema and presence of gas in the anteromedial aspect of the left inner thigh, with normal appearance of the right lower extremity (Figure 4). Axial views demonstrated the extent of edema and gas within the subcutaneous and fascial layers beginning at the anterolateral aspect of the left hip and extending distally into the anterior and anteromedial aspects of the left lower extremity at the level of the thigh (Figures 5–7). No evidence of intramuscular involvement was demonstrated on CT images. Based on the clinical presentation, laboratory values, and multimodality imaging findings, the patient was diagnosed with a necrotizing infection of the subcutaneous fat of the left lower extremity. This infectious process was believed to have extended to the medial fascia, without intramuscular involvement.
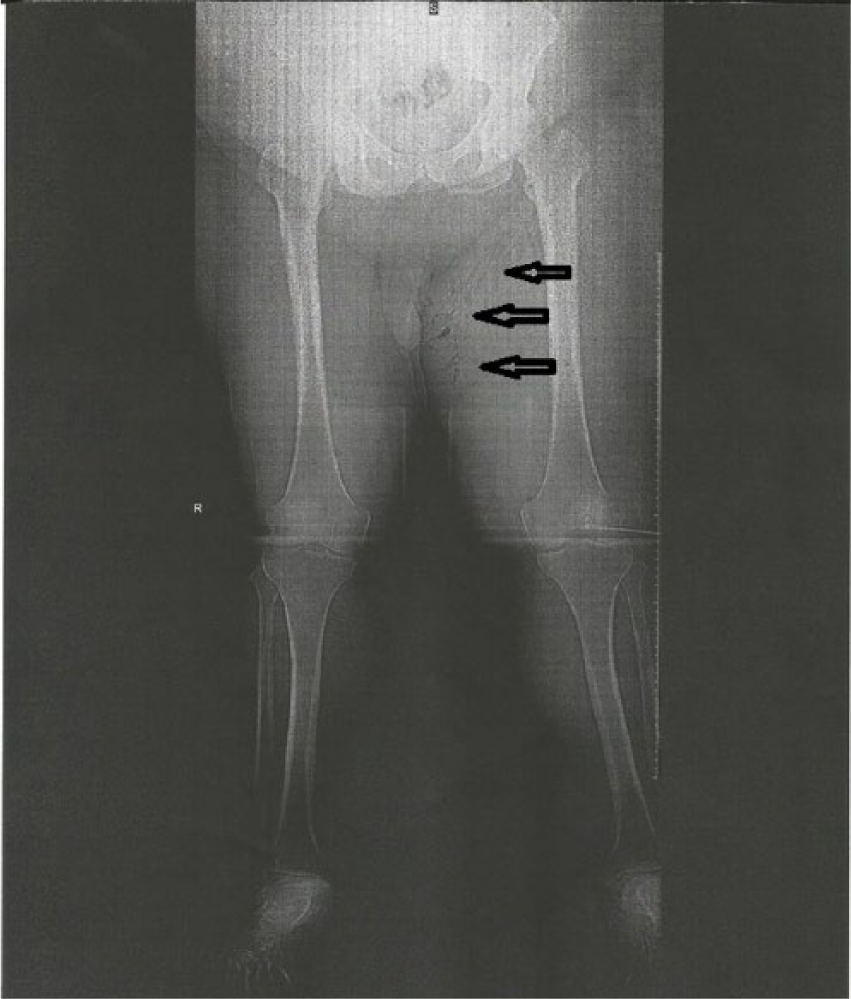
Coronal computed tomogram of the lower extremities showing a global view of the affected area of the left lower extremity, demonstrating extensive edema and presence of air in the anteromedial aspect of the left inner thigh.
Axial computed tomogram at the level of the hip showing fascial edema and gas within the subcutaneous and fascial layers of the anterolateral aspect of the left hip.
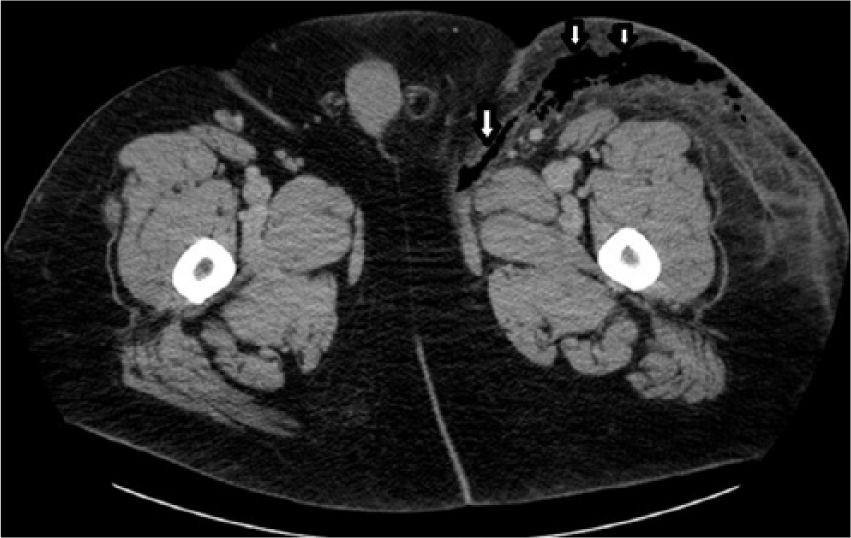
Axial computed tomogram at the level of the proximal thigh showing fascial edema and gas (arrows) within the subcutaneous and fascial layers traversing into the anterior and anteromedial aspects of the left lower extremity.
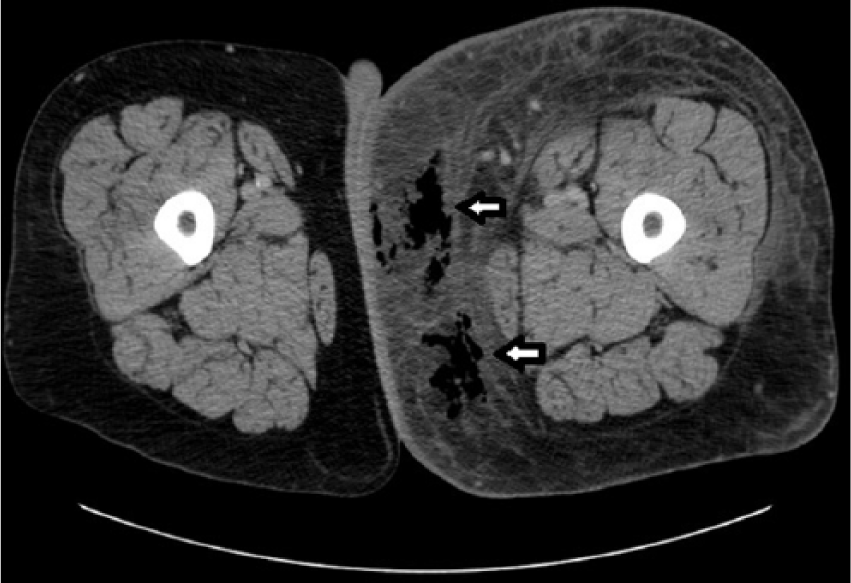
Axial computed tomogram at the level of the mid-thigh showing extensive fascial edema and gas (arrows) within the subcutaneous and fascial layers traversing into the medial aspect of the left lower extremity.
Upon translating the diagnosis of NF, the patient was then transferred to a trauma center for treatment. He was reported to have undergone two surgeries over a three-day time period in which his infection tissue was treated by extensive debridement to remove the necrotic tissue and the subsequent wounds were packed with dressings. Unfortunately, no additional follow-up information was available on this patient due to his transfer to an outside facility.
Discussion
Necrotizing fasciitis is a rare but life-threatening infection of the soft tissue characterized by inflammation that rapidly spreads, especially through the fascia and surrounding tissue.8–10 The soft tissue covering of the body is composed of several different layers. The skin, composed of the epidermis and dermis, is the outermost superficial layer. Beneath this is the subcutaneous tissue, which is composed of connective tissue and lobules of fat and superficial fascia. The superficial fascia is a network of blood vessels and nerves just beneath the skin that promotes movement and communication between the skin and underlying structures. The deep fascia is a form of connective tissue that covers skeletal muscle throughout the body. 11
Necrotizing fasciitis most commonly affects the lower extremities and often can be a complication of an injury, trauma, surgical incisions, or minor lesions.8,9,12,13 In addition, risk factors for developing NF include: obesity, immunosuppression, corticosteroid therapy, drug abuse, diabetes mellitus, and peripheral vascular disease (PVD).8,9,12,14,15 In 21% to 64% of NF cases, there is coexisting diabetes mellitus.8,14 In addition, comorbidities that can put individuals at greater risk of developing the condition include chronic renal failure, chronic alcoholism, peripheral vascular disease, obesity, and liver cirrhosis.3,4,12,16,17
Three classifications of NF have been proposed for added specificity. NF-Type 1 makes up 80% to 90% of all cases and is considered a polymicrobial infection, involving more than one bacteria. 8 NF-Type 2 involves the presence of GAS (Streptococcus pyogenes) and/or Staphylococcus aureus. NF-Type 3 is caused by gram negative rods; however, methicillin-resistant S aureus (MRSA) and Escherchia coli have been reported as causes of NF-Type 3 as well.8,9,12
The mortality rate for NF ranges from 6% to 76%, with the median being 32.2%, thus an early diagnosis is critical for an optimal patient outcome.2,5,8 The diagnosis is most often made through laboratory tests and imaging. Laboratory tests ordered for NF generally demonstrate an elevated WBC count. Additional medical laboratory results associated with NF are azotemia (elevation of blood urea nitrogen and serum creatinine levels), decreased platelet and fibrinogen levels, increased lactate and blood glucose levels, hypocalcemia, anemia, and hypoalbuminemia. 18 In some cases of NF, hyponatremia (decreased serum sodium level) and leukocytosis have been found to suggest diagnosis as well. 18 Blood cultures and/or wound samples are often collected to further pinpoint the specific microorganisms so that the proper antibiotics can be intravenously administered. 19 Clinical signs such as blisters and bullae with serosanguinous and hemorrhagic fluid drainage are visual inspection findings that can prompt diagnostic imaging to detect the possible presence of NF. Additional variables to consider are patient symptoms of swelling, inflammation, and pain that can coexist.8,9 Diagnostic imaging can provide further information regarding tissue characterization and depth of involvement to aid in establishing a multimodality diagnosis.
Local inflammation of soft tissue often marks the beginning of NF. It can progress to the underlying fascia, which can elicit systemic sepsis.8,10 The most common initial differential diagnosis is cellulitis, which can be coexistent.8,20 Diagnostic imaging such as magnetic resonance imaging (MRI), CT, and sonography can provide tissue characterization and multimodality information that should be correlated with the patient’s clinical presentation and laboratory test results for a diagnosis of NF.
Imaging
Magnetic resonance imaging has a sensitivity of 93% in detecting necrotizing fasciitis. 8 It is considered the gold standard for diagnosing NF and is considered superior to other imaging modalities because of its exceptional soft tissue imaging capabilities. 21 An MRI typically demonstrates thickening of greater than 3 mm in the deep fascia in addition to extensive multicompartment involvement of the deep fascia.21,22
Computed tomography has an estimated sensitivity of 80% in detecting necrotizing fasciitis.18,23 The cross-sectional imaging capabilities offered by CT can reveal intermuscular fluid collections and fascial plane thickening with variable contrast enhancement.21,24 A CT also demonstrates increased attenuation of the subcutaneous fat and shows gas and edema within the soft tissue layers.8,9 However, these findings lack specificity in both MRI and CT as they can often still be seen in cases of non-NF and even noninflammatory conditions. 25
In one study, sonography revealed a sensitivity of 88.2%, specificity of 93.3%, positive predictive value of 83.3%, negative predictive value of 95.4%, and accuracy of 91.9% in the diagnosis of NF. 26 With the use of sonography on unaffected patients, the skin generally appears as a single superficial echogenic layer at the top of the screen. Beneath the skin is the subcutaneous layer, which generally appears hypoechoic with randomly distributed hyperechoic fibrous septa, between the fat globules. The fascial planes are hyperechoic, and the muscle appears hypoechoic with brightly echogenic striations throughout. 27 Conversely, in cases of NF, sonography typically demonstrates distorted and thickened fascial planes with fluid accumulation in the fascial and subcutaneous layers. 28 Sonographic assessment may be limited by soft tissue gas, although if it can be identified, this finding may be diagnostically beneficial. 28 Sonography is often used as the imaging method of choice in pediatric cases of NF to limit radiation exposure. Sonography offers rapid, dynamic assessment of soft tissue, which is helpful in identifying fluid above the fascia (an indirect sign of NF).8,9 Due to sonography’s ability to detect fluid collections within the fascial planes, it can also aid in imaging-guided diagnostic fluid aspiration.21,29 Sonography can also be useful in distinguishing between various differential diagnoses of NF, such as abscess or cellulitis. The sonographic appearance of abscess typically appears more complex and irregular, while NF will often appear as subcutaneous thickening with the presence of air and fascial fluid. 30 The depth of tissue involvement shown by sonography can help to distinguish from cellulitis.
Cellulitis is defined as inflammation affecting only the dermal and subdermal layers of soft tissue, while NF has deeper involvement affecting the superficial fascia and subcutaneous tissue.31,32 The sonographic appearance of cellulitis is greatly dependent on the site and severity of the infection as the appearance can range from a diffuse swelling demonstrated by an increased echogenicity of the skin and subcutaneous tissue to a more variable cobblestone appearance, depending on the amount of fluid, degree of subcutaneous edema, and orientation of the interlobular fat septa. 33 A study conducted by Tsai et al. 34 aimed to determine how cellulitis and NF can be differentiated on sonography and found that the sonographic findings of NF include: an irregularity of the fascia, an abnormal fluid collection along the fascial plane, and a diffuse thickening of the fascia when compared with the opposite limb, if unaffected. 34 In comparison, when considering cases of severe infectious cellulitis, the aforementioned findings were not observed. 34
While research into the effectiveness of sonography in differentiating cellulitis versus NF is ongoing, there have been several reported cases where sonography accurately demonstrated characteristics consistent with NF while CT and MRI were only consistent with demonstrating changes indicative of cellulitis. 3 For example, a recent case reported by Kehrl 35 in 2014 details a diabetic patient who presented to the emergency department with atraumatic right foot and lower leg pain associated with fever. A point of care sonogram was performed as the clinical presentation was concerning for NF. The limited soft tissue sonogram demonstrated thickening of the deep fascia and the presence of fluid along the deep fascial plane, with fluid pockets measuring 6 mm in depth, factors suggestive of NF. However, CT and MRI of the patient’s lower extremity were performed, both being interpreted by the radiologist as demonstrating changes that were consistent with cellulitis. Septic shock and multisystem organ failure soon set in, and the patient was eventually taken to the operating room, where surgical intervention demonstrated findings consistent with NF. 35 These results help emphasize the utility of sonography in establishing an accurate early diagnosis of NF, which can lead to improved prognosis and patient outcome.
Conclusion
Necrotizing fasciitis is a rare but serious, life-threatening condition affecting soft tissues of the body, most often in the lower extremities. Multimodality imaging can play an important role in the diagnosis of the condition, most commonly sonography, CT, and MRI. In this particular case and others, sonography has shown to be a valuable imaging modality in the detection and characterization of NF, resulting in accurate diagnosis. The sonographic features that should raise the most suspicion for NF rather than a more common pathology are: irregularities of the fascia, thickening of the fascia, and abnormal fluid collections along the fascial plane. Early detection, diagnosis, and treatment are all keys to improving the patient outcome to prevent further tissue damage, amputation, and/or death.
Footnotes
Acknowledgements
The authors thank Courtney Angelhow, BHS, RDMS, and Megan Cravens, BHS, RDMS, RVT, for their assistance in obtaining images and information for this case study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.