
Abstract
Hemangiopericytoma (HPC) is a rare mesenchymal tumor that is predominantly found in the pelvis, retroperitoneum, and lower extremities, occasionally occurring in the larynx, spleen, bones of the thorax, or the meninges. A case is presented of a hypervascular soft tissue mass of the skull suggesting a diagnosis of hemangiopericytoma. Imaging modalities including computed tomography and sonography were used to help characterize this soft tissue lesion of the skull to aid in the proper course of diagnosis and treatment. The characteristics of hemangiopericytoma are described, and note is made that because of the vascular nature of these lesions, surgical intervention is used as a final resort when there are multiple reoccurrences following radiation therapy.
Introduction
Hemangiopericytoma (HPC) is a rare mesenchymal tumor that is predominantly found in the pelvis, retroperitoneum, and lower extremities, occasionally occurring in the larynx, spleen, bones of the thorax, or the meninges.1–8 Intracranial meningeal hemangiopericytoma (M-HPC) represents a rare and aggressive intracranial neoplasm located along the dural sinuses. It constitutes less than 1% of all intracranial tumors and approximately 2% to 4% of all meningeal tumors.9,10 Clinically, these tumors can present as palpable non-tender masses when they extend into soft tissue. Many authors have argued about the true origin of this tumor. Because these tumors are considered vascular in nature, sonography is a useful tool in adjunct with other imaging modalities such as computed tomography (CT). 11 Sonography is particularly able to characterize the lesion’s vascular and compositional elements. This case report describes a superficial lesion located on the left frontal/parietal portion of the scalp suspicious for hemangiopericytoma that was evaluated using both sonography and computed tomography.
Case Report
A female patient in her late 70s presented to the Radiology Department with a complaint of a “knot” on her head. Her past medical history included breast cancer. Her physical examination confirmed a non-tender palpable mass located on the left frontal/parietal portion of her scalp. The patient was referred for a soft tissue sonogram of the region of interest and was later referred for a correlative CT for the same area.
Sonographic Findings
Sonographic findings included a large hypervascular solid appearing lesion correlating to the non-tender palpable mass on the patient’s scalp. The mass measured up to 6 cm in its longitudinal dimension (cranio-caudal) and 3.3 cm in its antero-posterior dimension, obtained in the sagittal plane (Figures 1 and 2). In the transverse plane, the mass measured up to 3.3 cm in its widest dimension (Figure 3). The mass appeared to extend through the adjacent calvarium, with the bony defect measuring 2.7 cm at its widest point (Figure 3). This figure also shows small spicules of bone that were seen as multiple small echogenic foci near the defect of the calvarium, which was suggestive of a malignancy arising from the skull. The mass also appeared to extend intracranially but was not able to be completely characterized on this superficial sonographic examination. The vascularity of the mass, extending through the defect of the calvarium, was shown by color Doppler imaging (Figure 4). Further testing using CT without contrast was recommended and obtained three weeks later.
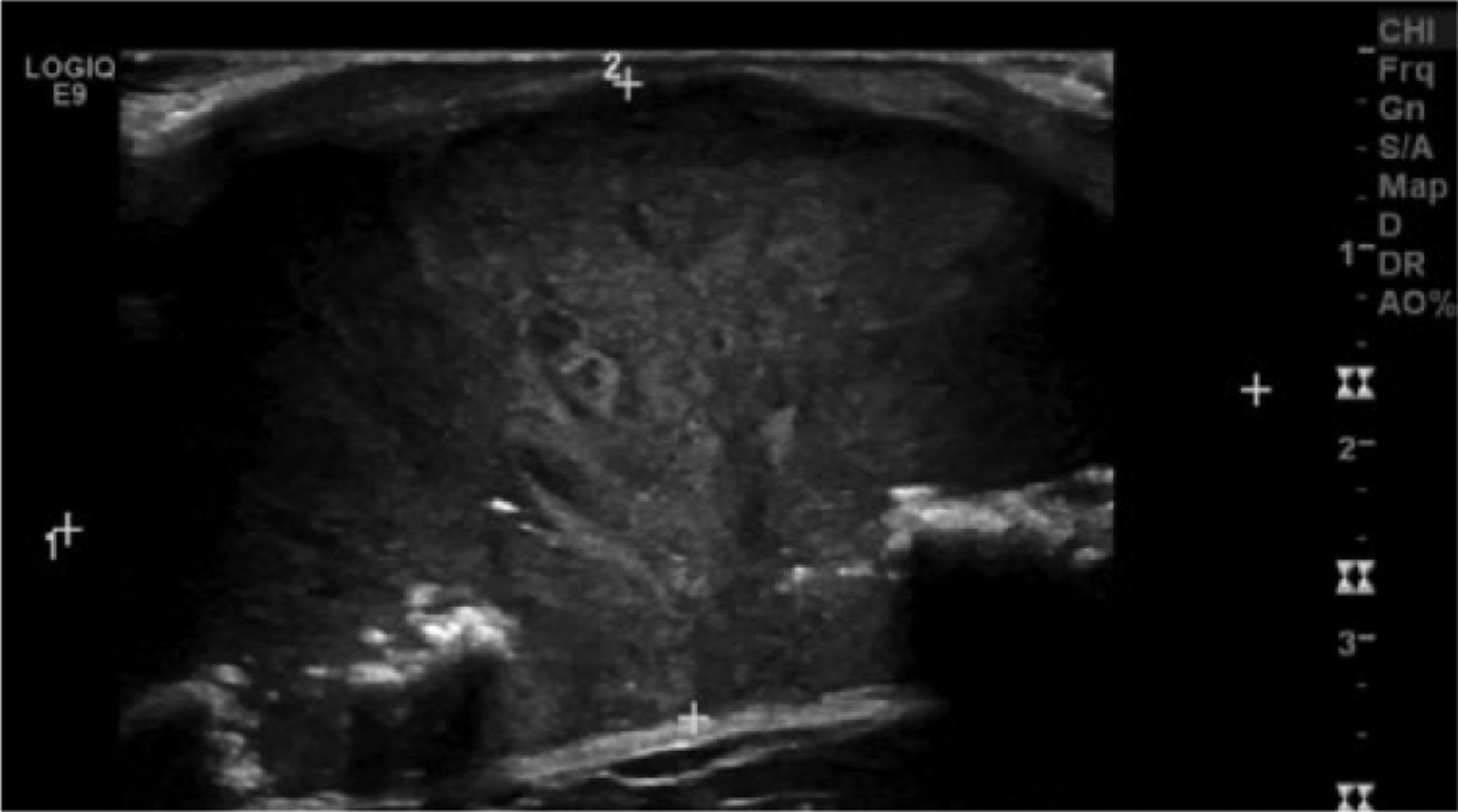
Gray-scale longitudinal view of the superficial soft tissue mass showing where calipers were placed to determine maximum measurements in the (1) cranio-caudal and the (2) antero-posterior dimensions. (The top of the skull is to the left in the image.)
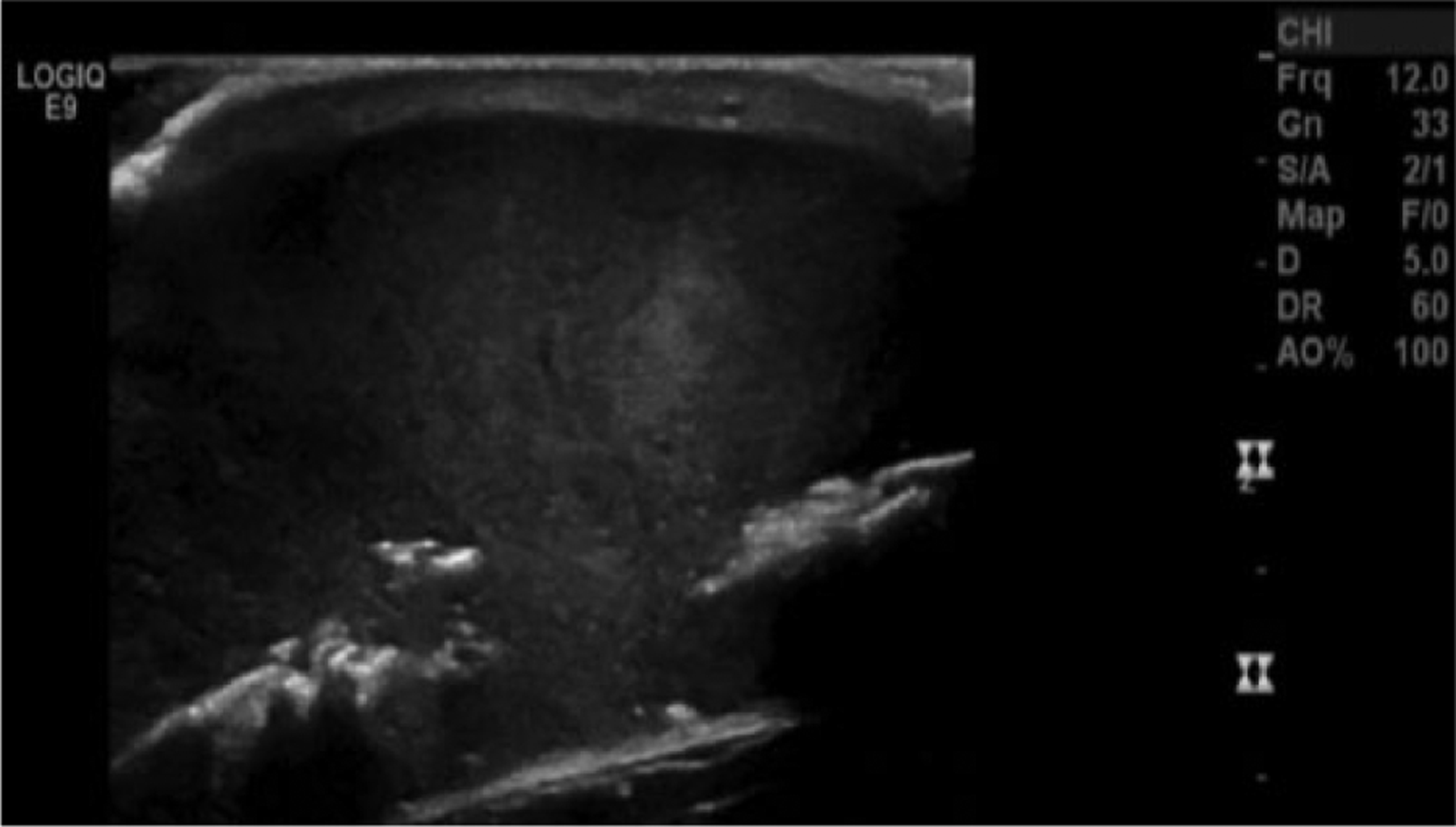
Gray-scale longitudinal view of the superficial soft tissue mass showing echogenic foci characteristic of small spicules of bone near the defect in the calvarium.
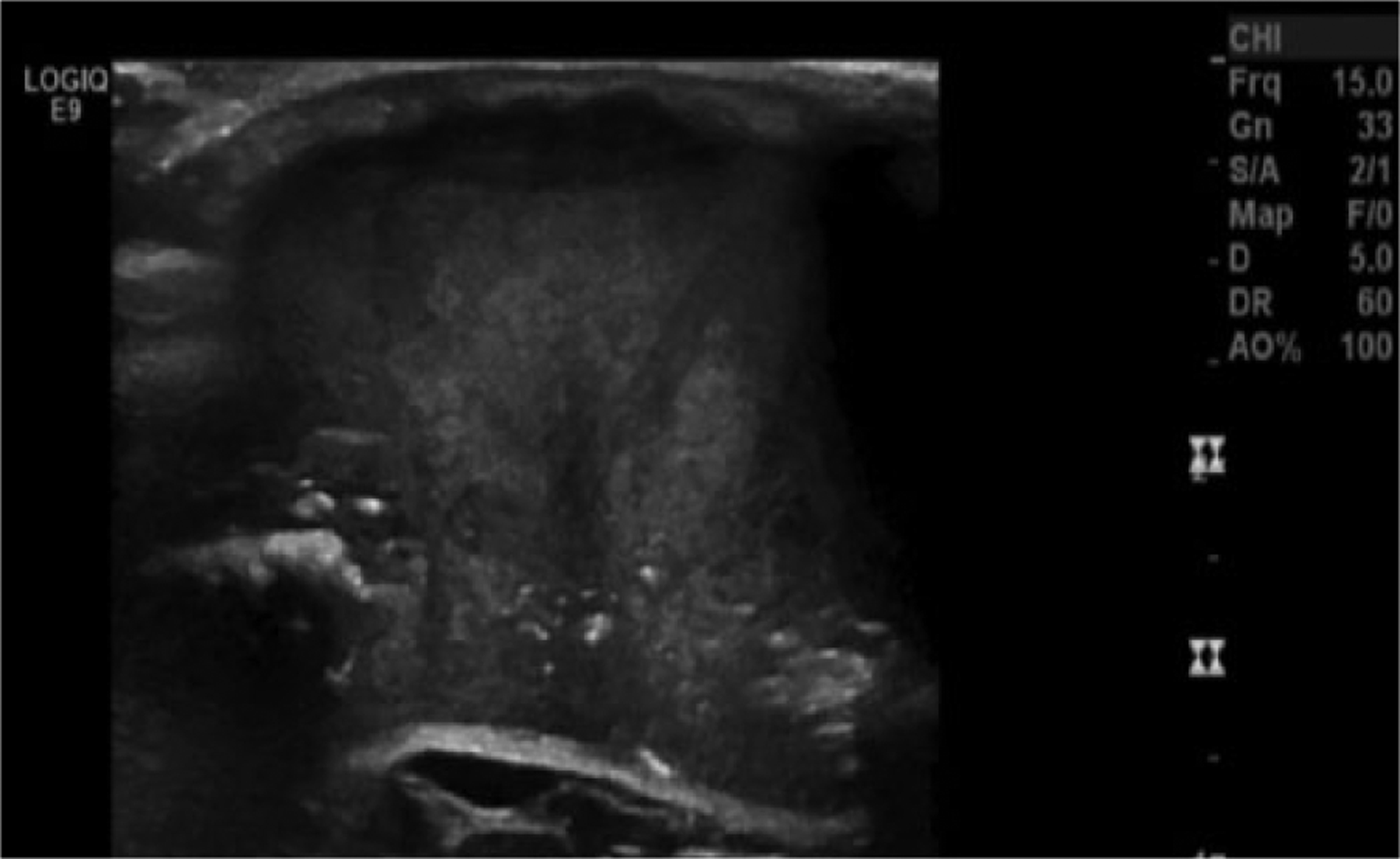
Gray-scale transverse view of the superficial soft tissue mass showing its maximum left-to-right widest dimension as well as the greatest dimension of the defect in the calvarium; also seen were the echogenic foci of the small spicules of bone. Appreciation of the gyrus portion of brain tissue can be seen deep to the defect of the calvarium.
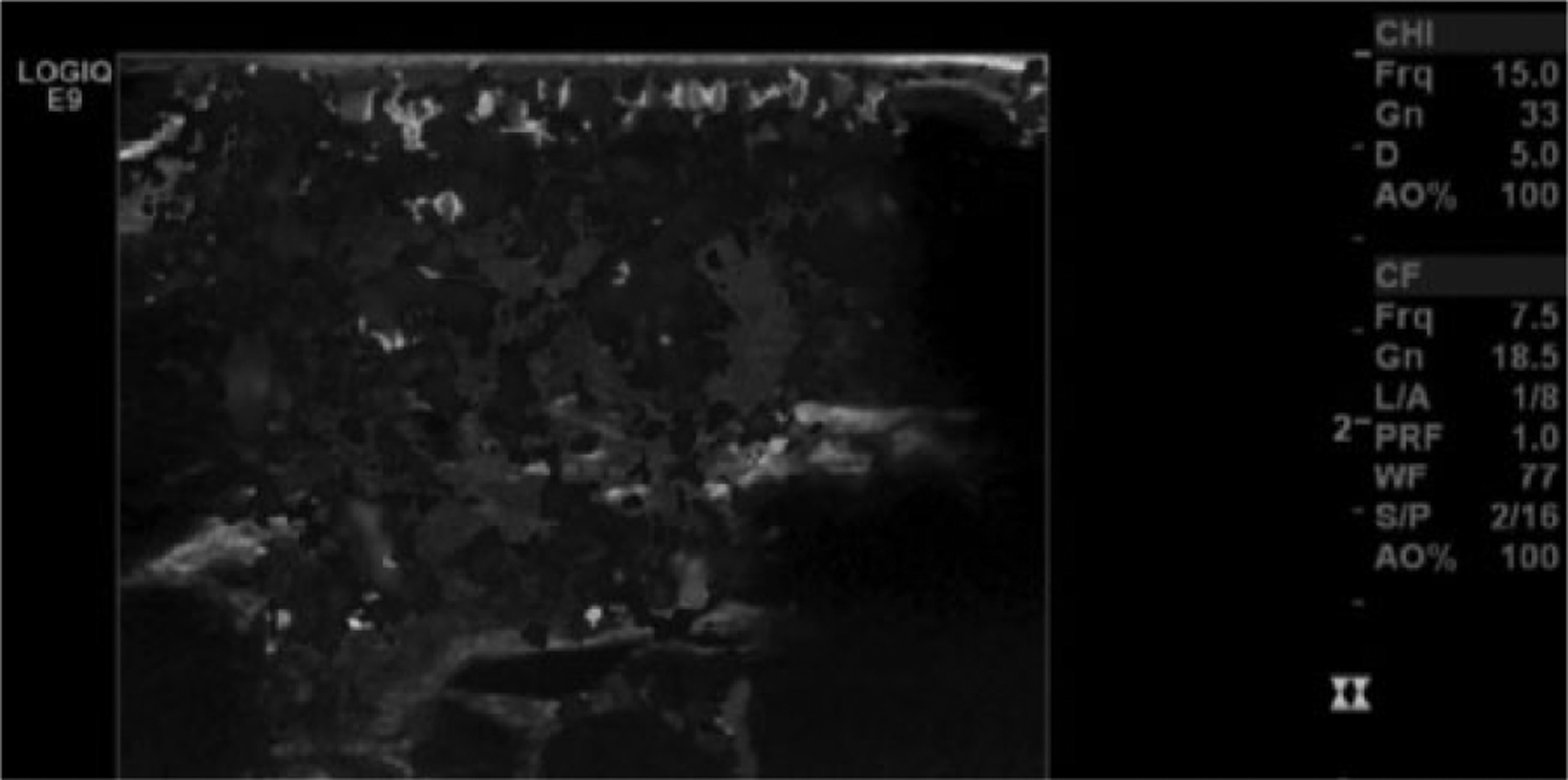
Transverse view similar to that in Figure 3 taken using color Doppler imaging (color is displayed in gray-scale) showing the high degree of vascularity of the tissue mass.
Computed Tomography Findings
Computed tomography without contrast was done using 5 mm axial cuts obtained from the vertex through the base of the skull per routine protocol (Figures 5A–5D). A large, partially pedunculated soft tissue mass arising from the vertex scalp of the left parietal scalp was shown. This mass measured up to 7 cm in largest transaxial diameter. Associated permeative destruction of the underlying parietal and frontal calvaria was also shown without significant change since the prior sonographic study. The paranasal sinuses were clear.
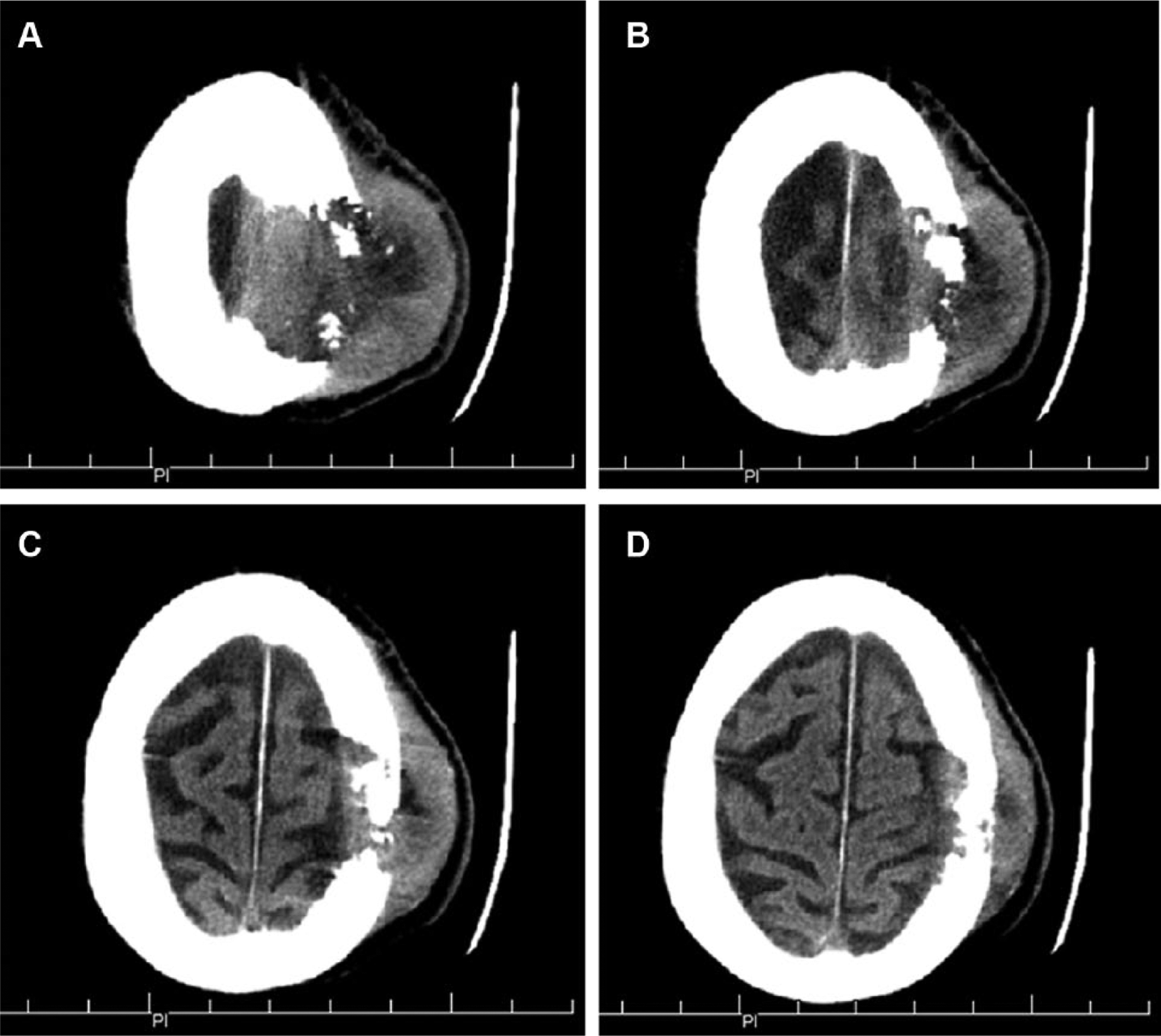
Five-mm axial cuts of computed tomography images obtained beginning at (A) the vertex of the skull and (B–D) progressing inferiorly, showing the soft tissue mass and the defect in the calvarium.
No further clinical follow-up or tissue biopsy diagnosis was available for this patient, making the diagnosis presumptive for hemangiopericytoma but not proven.
Discussion
Hemangiopericytoma is a highly vascular tumor that occurs around capillaries and postcapillary venules. 4 It originates in a specific cell type called pericytes, identified by Rouget in 1873 and subsequently described by Zimmermann in 1923.9,12 Just slightly more than 300 cases of HPC have been reported since Stout and Murray 12 described HPCs as “vascular tumors arising from Zimmerman’s pericytes” in 1942. 13 They account for 3% to 5% of soft tissue sarcomas and only 1% of all vascular tumors with the frequency of occurrence in the head and neck at about 16% to 33%. 8 The rarity of HPC and its controversial histological classification results in its frequent misdiagnosis, thus making the treatment quite challenging.4,8,9
The World Health Organization classification of central nervous system tumors previously considered HPC tumors a very close comparison with meningiomas, but the current classification system introduced in 2007 distinguishes HPC as a separate entity. Recent studies have suggested that the histomorphology and immunophenotype of HPCs are different from that of meningioma. Presently HPCs are classified into a group of “mesenchymal, non-meningothelial tumors.” 10 Formerly considered one of the variants of meningioma, and often referred to as “angioblastic meningioma” because these tumors are considered vascular in nature, sonography is a useful tool in adjunct with other imaging modalities such as CT.4,11
Typical of these tumors, the case reported previously was first demonstrated as a non-tender palpable soft tissue mass presenting on the patient’s skull. The hypervascular characteristics of the mass were also demonstrated using color and spectral Doppler imaging techniques with duplex sonography. Although the official final report did not state a definitive site of origin for the mass, HPCs have been noted to arise often from dural sinuses, the skull base, tentorium, and the falx cerebri. 6 Based on the presentation of the mass demonstrated on both sonography and CT, it was believed likely that the mass was skull-based in origin.
These very aggressive tumors are characteristically highly cellular and richly vascular, tending to recur even after macroscopic total resection. 14 A microscopic diagnosis is based on the recognition of an architecture characterized by a pericytomatous pattern. However, the same pattern occurs in a variety of neoplasms, such as fibrous histiocytoma, solitary fibrous tumor, and fibrous meningioma. 4 Therefore, distinguishing HPC from other tumors can be difficult, especially when the characteristic features of other neoplasms are inconspicuous. However, because of differences in the prognosis and patient management, a proper diagnosis is critical. Unfortunately, there was no available follow-up information for this case to report such as histological results or treatment. Several authors, however, have reported that lytic destruction of the adjacent skull on plain X-rays or CT suggests an HPC while hyperostosis, or the excessive growth or thickening of bone tissue, suggests a meningioma.8,9 Marked lytic destruction of the calvaria was demonstrated on both sonographic and CT images obtained for this case. Sonographic images demonstrated both a defect in the calvaria and spicules of bone nearby, leading to the high probability that the mass had lytic properties. Both the gyrus and sulcus of the patient’s brain tissue could also be appreciated deep to the defect of the calvaria, again suggesting that the mass was an HPC and not a meningioma.
Meningeal HPCs can recur locally or distantly in the neural axis or as extraneural distant metastases.15,16 They have a relentless tendency for local recurrence and metastases outside the central nervous system, which can appear even many years after diagnosis and adequate treatment of the primary tumor. 10 The local recurrence rate varies from 45% to 91% among different studies, and a 15-year distant metastasis rate approaches 70% after surgery alone.8,9 The patient in this case, however, already had a previous history of breast cancer. In a study of 21 patients carried out over a 34-year period, patients with surgical removal of an intracranial meningeal hemangiopericytoma followed by external radiotherapy had a reduced risk of local recurrence. 7 Considering the aggressive nature of HPCs, gross total resection of the tumor is the optimal treatment method, though complete resection can be difficult or impossible because of the highly vascular nature of the lesion and the risk of bleeding tendency in the operative field. Because of this, some authors have suggested the use of radiotherapy as a neoadjuvant treatment based on the possibility that the proliferating capillaries will be obliterated after radiation. 16 Stereotactic radiosurgery may be an alternative option for the treatment of HPCs that are less than 2 cm in diameter with radiation doses of 15 GY or higher at the 50% isodose line.
Conclusion
The rarity of hemangiopericytomas and their unique histological properties make the correct diagnosis of such a lesion difficult based solely on diagnostic imaging findings. Some characteristics, however, including the high vascularity and the lytic properties of the mass, can be appreciated sonographically and be suggestive for HPC. Because of the aggressive and vascular nature of this lesion, it is imperative that proper technique is used to adequately represent the characteristics of the lesion so that appropriate management and treatment options can be undertaken. Sonography can be as a significant adjunct tool in assessing both the lytic and vascular components in lesions that present as soft tissue palpable masses in asymptomatic patients. This case report is meant to help sonographers characterize and distinguish the features of hypervascular tumors in order to reach a proper diagnosis.
Footnotes
Acknowledgements
A special thank you to Baylor University Medical Center in Dallas, TX, for their contribution of images and reports and to El Centro College’s Diagnostic Medical Sonography Program for their everlasting effort to educate the sonographers of tomorrow. Special acknowledgments to Jennifer Shovlin, RDMS, RVT, and Lynn Schluns, BS, RDMS, RVT, for their assistance in preparing this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.