
Abstract
Simulation allows educators to teach important skills outside the clinical environment. The objective of this study was to evaluate advantages of a testicular phantom scanning workshop in a sonography curriculum and ascertain if it is a beneficial teaching tool. Students participated in a workshop facilitated by registered sonographers using testicular phantoms and ultrasound machines. Students provided anonymous feedback. All participants found this activity helpful. Sixty-seven percent indicated that the phantom reflected a good representation of a real patient. Ninety percent indicated that scanning skills improved and the workshop positively affected their confidence in performing the examination. More than 90% reported greater confidence in describing the examination to a patient. Ninety-five percent reported increased knowledge of sonographic anatomy and identification of testicular structures. These sonography students perceived the testicular simulation workshop as a positive learning experience that increased confidence and skills in testicular scanning and as a viable tool for teaching testicular sonography.
Simulation has been a part of healthcare education as early as 1960, with the creation of Resusci-Annie 1 for cardiopulmonary resuscitation education, but until recently, its range of usage and application was limited. In the past, healthcare education methods have included lecture and clinical training at the bedside. Sonography students learned didactic material in the classroom and learned to scan on patients in a hospital setting. Perhaps now teaching techniques are beginning to change. With the advent of new technologies and increasing demands for patient privacy and safety, simulation technology is advancing, and companies are developing products for use as tools in healthcare education.
Simulation provides an opportunity for healthcare professionals to teach important concepts and run training drills in a safe environment without penalties, risk, or consequence of errors. It provides instructors with an opportunity to give immediate feedback on student behavior and performance during the activity. It allows students to ask probing questions that they would not or should not ask in front of a patient. Simulation has become an increasingly popular way to educate medical students and allied health professionals, as access to patients in clinical settings may decrease or become complicated.2,3 Using simulation can address the acquisition of deliberate practice, psychomotor skills, and affective domain training, 4 all vital skills needed by healthcare providers. It can also provide a more uniform training experience. 3
Simulation training has increased in popularity as educators recognize the advantage that it provides to kinesthetic learners, using a hands-on and experiential approach to learning.4,5 This is also a method well received by adult learners.6,7 In the past, the products and technology were not advanced enough to provide realistic images. With renewed interest in simulation education and improved technology, a new generation of sonography simulators and phantoms has appeared on the market that makes it a viable tool for education.
The literature describes many different types of simulators, task trainers, and phantoms that are now available.8,9 Phantoms (low-fidelity simulators) can be created using easily obtained materials or purchased through commercial vendors (i.e. task-trainers). High- fidelity computer simulators are also available from commercial vendors for sonography training. Each of these types of simulators has advantages and disadvantages. Some variables to consider are cost, portability, long-term life, realistic texture of tissue, sonographic appearance, and the ability to be noninfectious. 9 High-fidelity simulators are costly, and homemade phantoms have limited use before they degenerate. There is a range of capabilities and qualities that vary with different sonography simulation equipment and phantoms. As such, there are different options for simulation, and one must assess them individually to determine how best to implement them.
Simulation can be used for practicing interventional sonography-guided procedures and for diagnostic cardiac sonography, emergency sonography, obstetrics and gynecology, and superficial structures, without having to practice on a human patient. Although used for medical education, 3 there is little research on using simulators to teach sonography students. The simulation platform currently available for testicular training is the low-fidelity phantom (task trainer).
Sonography phantoms are models of patients or representative body parts that have been uniquely crafted to mimic soft tissue and organs, and when used with ultrasound systems, the images generated are highly representative of human tissue.
Phantom scanning is particularly useful for certain types of sonography studies. Because of the sensitivity of patient preparation and interaction required for various sonography examinations and because many students may not have enough clinical experience with certain types of examinations, testicular and pelvic phantoms can be valuable training tools.
Challenges for Adopting Sonography Simulation Products
A significant amount of time and effort is required to create, design, and integrate simulation into a curriculum. 4 Many options for sonography simulations are available for purchase, and the number of companies creating simulation products continues to proliferate. 2 The use of these products in medical and allied health education may be questionable. Challenges in acquiring and integrating these technologies into an education curriculum are varied. Simulation technology is expensive, and prior to purchase, an institution must evaluate the products to determine how realistic the simulation is. Funding must be secured for the purchase, as well as time allotted for training of faculty. Faculty must evaluate how simulation activities will be aligned with the intended learning objectives. Space must be available to store the equipment, and a low student-to-faculty ratio should be available to implement this type of training successfully. 10
Rosen 1 indicated that three items have contributed to the delay in accepting simulation as part of medical education, namely, “lack of communication, skepticism, and the burden of proof.” Rosen noted that widespread acceptance of standardized patients, virtual reality, and mannequins has occurred only in the past decade. Studies that demonstrate that simulations are effective tools have yielded preliminary results with mixed outcomes.4,8
Medical simulation can be divided into five categories: verbal (role play), standardized patients, part task trainers, computer patients, and electronic patients. 11 Despite the fact that research is just beginning with regard to the effectiveness of simulation training, 4 Gaba 11 stated that, historically, many vocations requiring human safety have adopted simulation for critical skill training, deciding that it is more prudent to save human lives by reaping the potential benefits of simulation, rather than wait for definitive proof.
Although there are studies evaluating both the efficacy and benefits of sonography phantoms for learning sonography-guided intervention procedures, there are few data regarding how phantoms may assist in educating students.
Sonography scanning requires cognitive, affective, and psychomotor skills that are all vital to providing a quality examination. Acquiring diagnostic quality images requires specific complex interactions between the patient, equipment, and sonographer. 12 Simulation is a good way to introduce a first-year sonography student to the skills necessary to scan the testicles. It provides students with a learning environment with the opportunity to have specific instruction, the ability to practice with immediate feedback, and no harm or embarrassment to the patient or student sonographer. The student has the leisure of deliberate practice 13 and the freedom to ask “what if” questions that one could not do in a clinical setting.
Although there may be limitations regarding the ability to integrate simulation into the curriculum due to cost, access, and trained faculty, it can be an adjunctive measure to enhance sonography education. This was a pilot research study that involved first-year sonography students participating in a testicular phantom scanning workshop.
Materials and Methods
This study was approved by the local institutional review board and deemed exempt. This was a prospective observational study conducted at the College of Health Related Professions, in a Commission on Accreditation of Allied Health Education Programs–accredited sonography program. All 21 students participated in a testicular phantom scanning workshop as part of their first-year sonography curriculum.
Students were divided into groups of three and assigned to a faculty facilitator. To ensure consistency of instruction across the different groups, the program director conducted a training session with faculty. During this session, the key points were outlined, content reviewed, and approach discussed. A lesson plan provided faculty with detailed steps used to introduce students to skills needed to perform a testicular sonogram. Registered Diagnostic Medical Sonographer (Abdomen) instructors led the workshops. Equipment used for the workshop included Philips HD7 ultrasound systems (Philips Ultrasound, Bothell, WA, USA), conductive gel, L12-3 Mhz linear-array transducers, Blue Phantom Scrotal Phantoms (CAE Healthcare, Sarasota, FL, USA), towels, and gloves. The workshop objectives included identifying common indications for testicular sonograms and demonstrating patient preparation and proper positioning of genitalia as well as appropriate dialogue with the patient, identifying and recognizing sonographic views of testicular anatomy, using hand–eye coordination and movement required for testicular scanning, and acquisition of sonographic images (Figure 1).
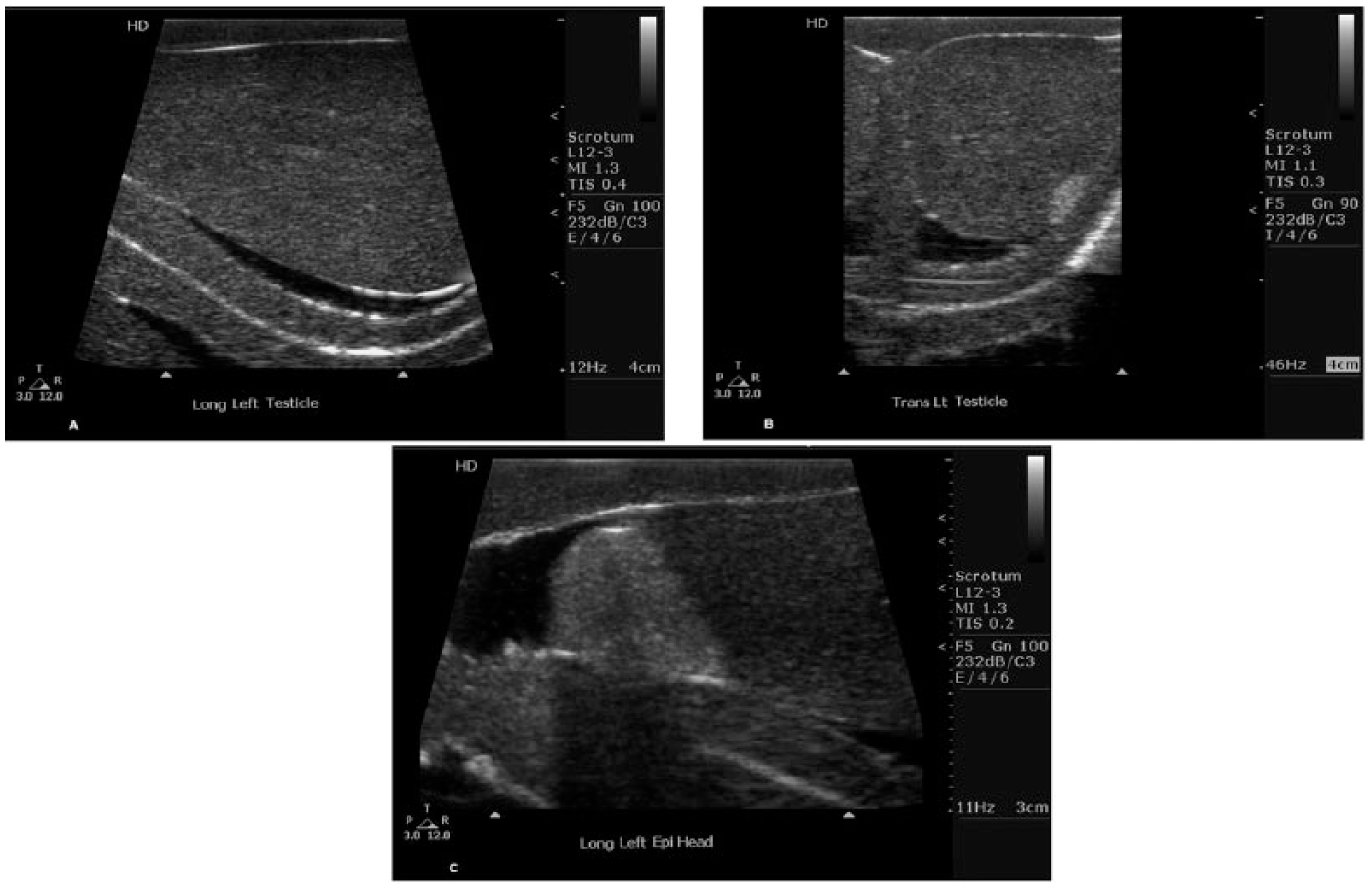
Sonographic images obtained from the Phantom. (A) Longitudinal partial view of testicle. (B) Transverse view of testicle. (C) Longitudinal view of the epididymal head.
Each workshop had a 10-minute introduction by faculty, followed by student groups each having a 25-minute scanning session of the phantom with faculty supervision and feedback. Students were encouraged to role-play with the phantom, ask patient history, describe the examination, and then perform a testicular sonogram, identifying the anatomy as they scanned. At the completion of the activity, each student answered three open-ended questions regarding the experience; within 24 hours, they received an anonymous survey link asking them about the session. The survey included Likert-type scale multiple choice questions and demographic information.
Results
All 21 students participating in the workshop completed the survey. All students were female (no male students were enrolled in this cohort of students at this time). All students indicated that the phantom workshop was helpful and gave a better understanding of testicular anatomy. When asked what would help improve the sessions, many students indicated more time.
In evaluating the students’ exposure to scanning or observing testicular sonography prior to this workshop, all students (n = 21) indicated that they had seen fewer than ten testicular examinations in the clinical setting, and all indicated that they had personally performed fewer than four testicular sonograms.
Ninety-five percent of students reported that the phantom activity increased their knowledge of the sonographic appearance of the testes, epididymi, and surrounding structures, and 90.5% expressed greater confidence in identifying testicular anatomy (Figure 2).
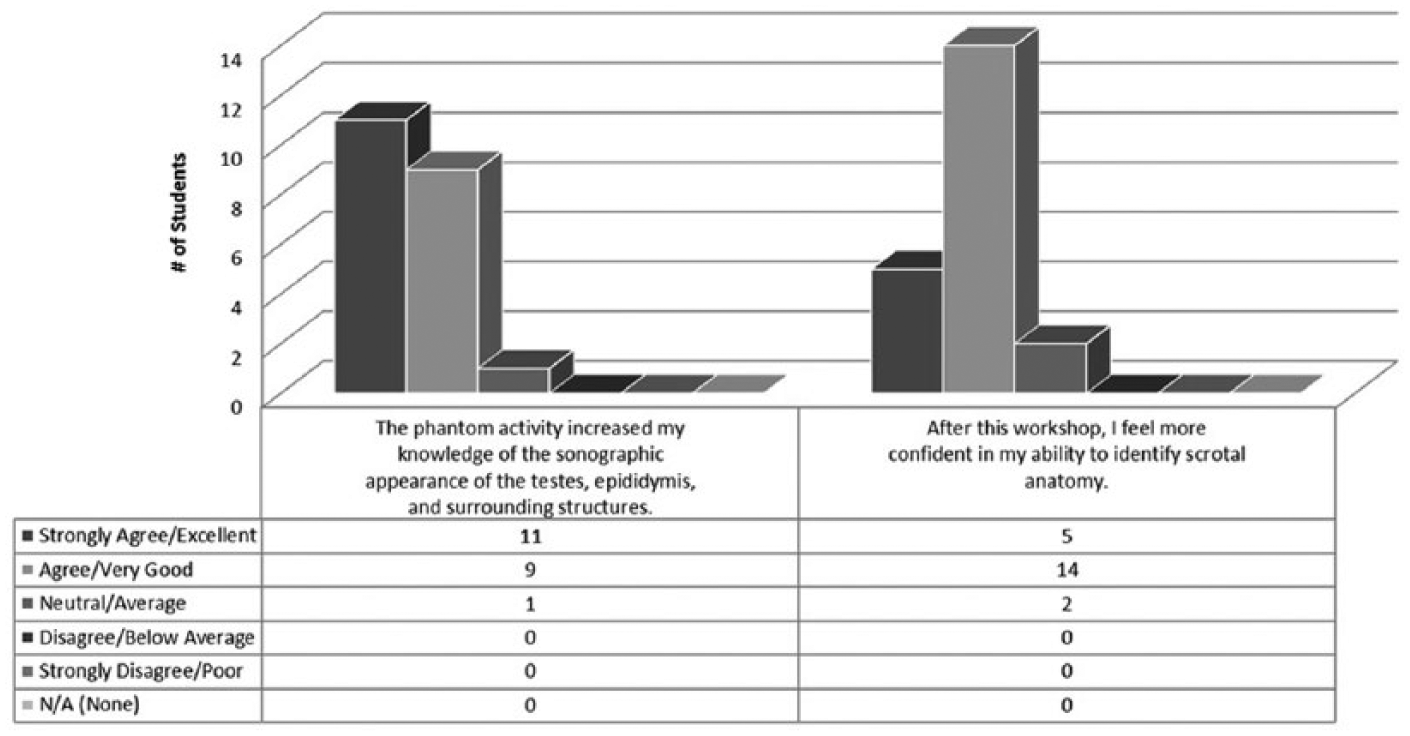
Student feedback.
A challenge in adopting simulation technology is its likeness to real human appearance and sonographic appearance. The Blue Phantom scrotal sonography training model was used for this workshop; 67% (n = 14) of students indicated that the phantom was a good representation of a real patient, whereas 33% (n = 7) were neutral. Only 5 of 21 students (23.8%) reported their scanning skill level as average prior to the simulation activity. After the workshop, 90% of students reported that their scanning skill for this examination had improved (Figure 3). Nearly 91% of students reported an increase in confidence in describing the examination to a patient. Ninety-five percent reported increased confidence preparing the patient for an examination, and 90.5% reported an increased confidence level in performing the testicular examination (Figure 4). Ninety-five percent of students indicated that the phantom was a useful teaching tool, and all 21 students indicated that they would like to have an opportunity to participate in more scanning workshops in the future.
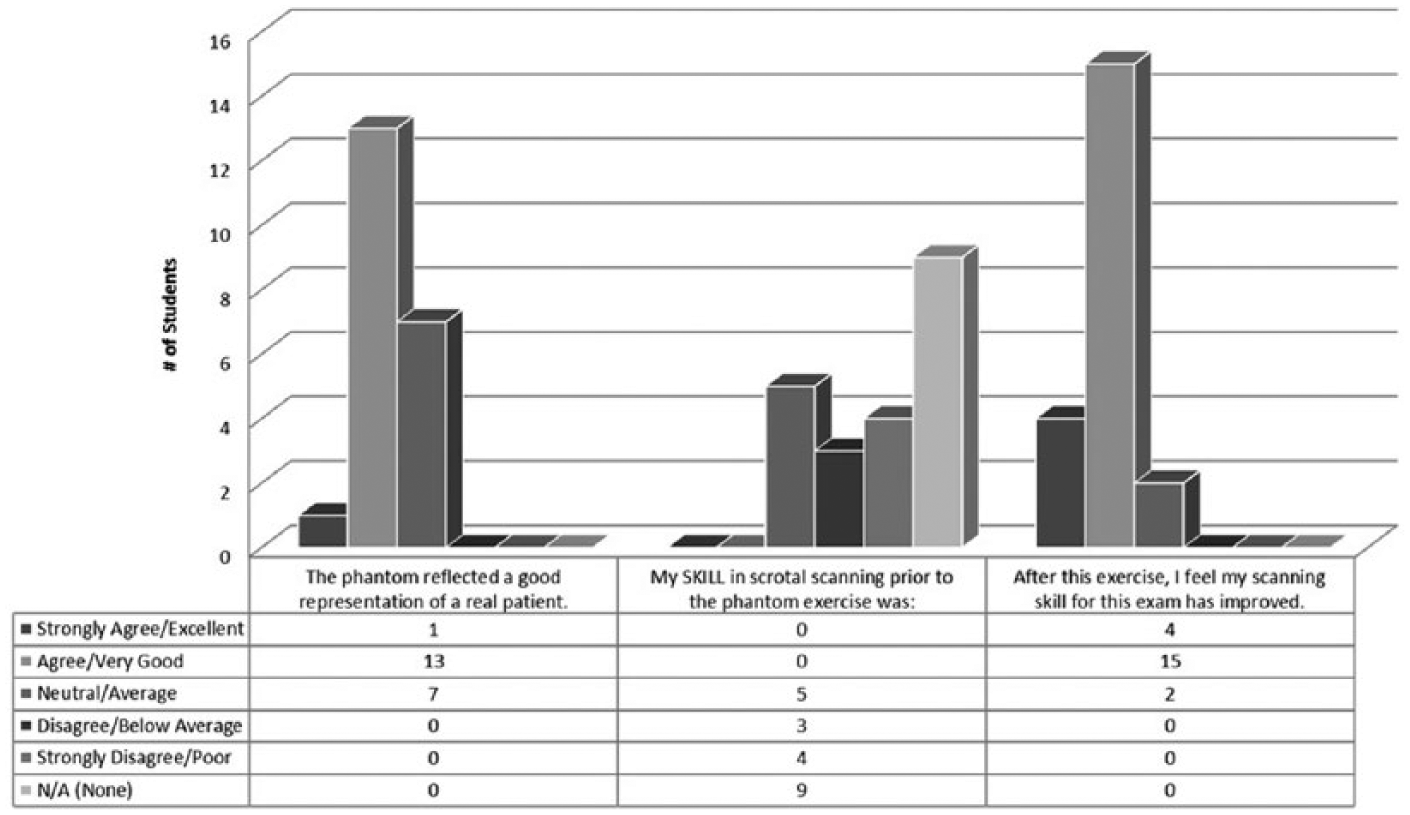
Student scanning skill.
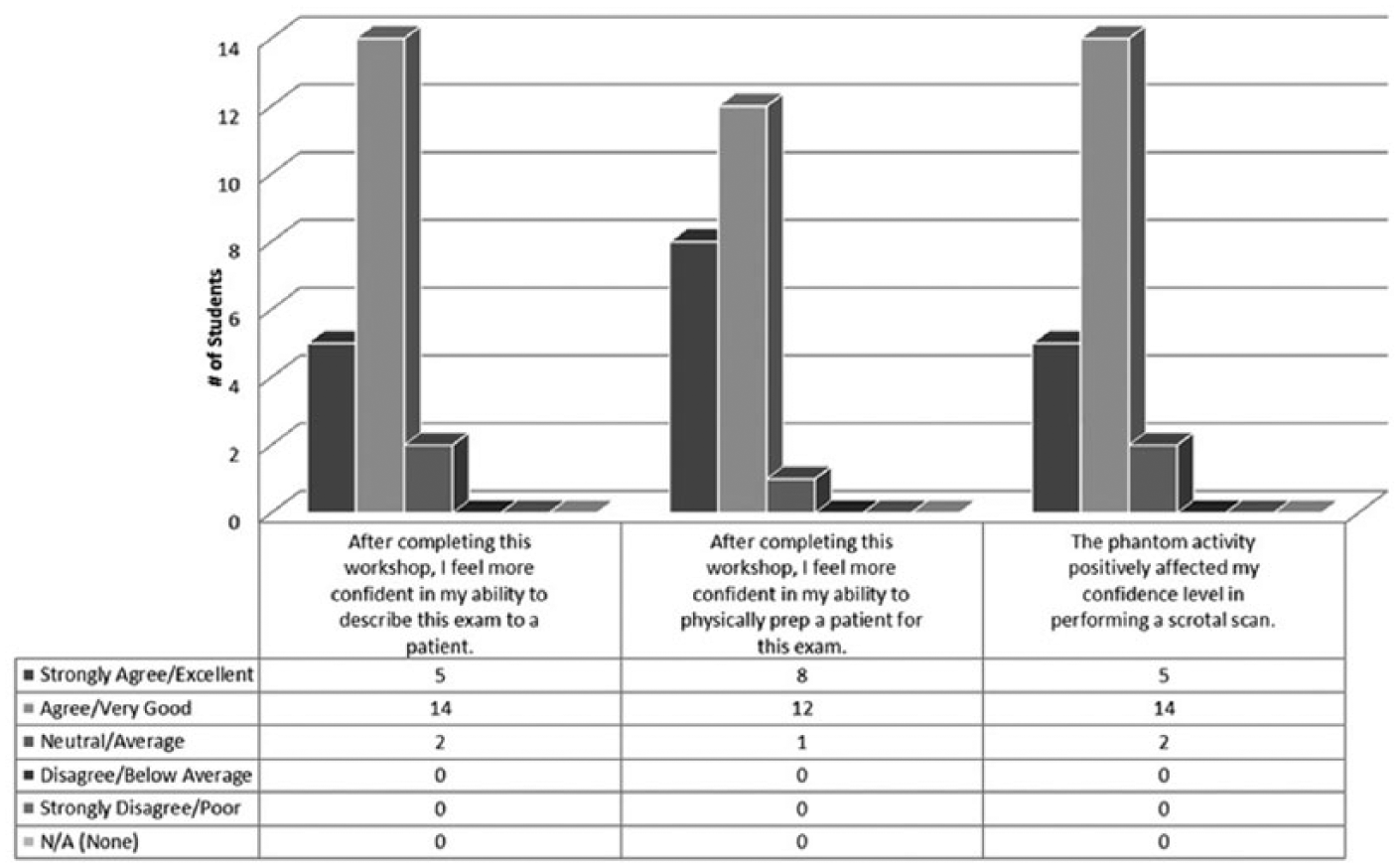
Student confidence in patient interaction.
Discussion
Performing a testicular sonogram on a patient for the first time can be awkward and intimidating for a sonography student as well as the patient. Many students can be uncomfortable with explaining the procedure to the patient, taking a proper patient history, and performing the sonographic examination. In addition, access to patients requiring this type of examination is limited, and if a student is not confident in his or her ability to perform the examination, the student is less likely to volunteer to conduct the examination.
As much of the literature has indicated, simulation provides an opportunity for students to learn in a risk-free environment. Creating a safe environment where a sonography student can role-play proper patient interaction and use a scrotal phantom to practice scanning, one can increase the confidence level of student sonographers, as evidenced by these results. Dividing the students into small groups of three allowed faculty to provide one-on-one feedback, and students were able to ask questions or raise concerns without any detriment to a patient. All students were unanimous that the workshop was time well spent and was personally useful. Although some students expressed concern that the phantom was not exactly like a real patient, they all recognized the value of practice in a no-risk environment with immediate feedback on their scanning. Students also recognized that the phantom could not replicate vascular perfusion, and thus the activity could not simulate any vascular pathology such as torsion or varicocele.
When using phantoms, the scanning experience becomes learner centered, not patient centered, as it would be in the clinical setting. 3 The simulation workshops integrate Kolb’s cycle of learning by providing concrete experiences with active experimentation and reflective practice. 7 Four levels of learning can be acquired and/or evaluated: basic knowledge, applied knowledge, performance, and action. 7
Simulation platforms and products should always be evaluated by experienced practitioners to assess usefulness and realism. Although the phantom was not perfect, most students were happy with the level of quality and similarity of the phantom’s likeness to a true sonographic appearance of testicular anatomy. Those who choose to adopt phantoms or high-fidelity simulators for student education are encouraged to investigate what is available and test products before adoption, as they can be costly or lack realism.
Although simulation activities require a significant amount of time in a curriculum and investment of faculty time to ensure low student-to-faculty ratios, students overwhelmingly enjoyed this activity and requested more workshops. Simulation can provide hands-on experiential learning that can make a difference in student-sonographer confidence levels. This activity enabled students to hone their expertise in the clinical setting, instead of spending time acclimating to protocol and patient interactions.
Limitations of this study are that this was a convenience sample and the design of the study is purely descriptive. In addition, the small sample was female gender biased, so it would be difficult to ascertain if male students would provide similar results. One should note, however, that this is reflective of trends in the field, as most practicing sonographers are female. With particular regard to the phantom representing a real patient, it should be noted that nearly 43% (n = 9) of the sample had not observed a testicular examination on a real patient prior to the workshop. When these responses were removed, 75% of respondents indicated that the phantom was a good representation of a real patient. The testicular phantom, however, cannot spontaneously move or demonstrate vascular blood flow or perfusion like a human.
Suggestions for further studies include evaluating the level of knowledge of testicular sonography with a pretest and posttest design as well as including male students in the sample.
Conclusion
New simulation technology products are available, and their integration is becoming more widespread in healthcare education. Although simulation adoption can be costly and require planning and faculty effort, it provides an immersive student experience and could be a valuable teaching tool. The low-fidelity Blue Phantom scrotal phantom with an ultrasound system provided an excellent, effective method of teaching testicular sonography and achieved great student satisfaction with learning. Experiential learning in a safe environment allows students to acquire hands-on skills without concern for adverse effects on patient care. It also enables students to be better prepared to maximize their clinical education opportunities.
When students are trained using these techniques, they enter a clinical environment confident in their knowledge and with a greater skill set. Simulation could assist with bridging the gap between the didactic and clinical experience, identifying skills that need to be acquired, refined, and addressed in a safe learning environment.
Footnotes
Acknowledgements
The authors would like to acknowledge Diagnostic Medical Imaging faculty Rivka Hellmann, Melissa Paraison, Donna Sceusa, and Iryna Struk for their participation in this project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.