
Abstract
Background: Smoking is considered to be associated with a variety of public health problems. The objective of this study was to explore the effects of smoking on carotid artery hemodynamics in Saudi Arabian participants. Methods: In a quantitative descriptive study, 121 participants were investigated by B-mode and Doppler sonography: 76% (n = 92) were smokers, and 24% (n = 29) were nonsmokers. The mean age of all participants was 36 ± 2 years (range, 19-100). Carotid arteries for all participants were evaluated with 7-MHz linear transducer according to a standard carotid sonography protocol. Results: The majority of the smokers (89.1%) were asymptomatic. The prevalence of carotid plaques in the smoker group was 22.8% of the 92 subjects. There was a significant statistical association between frequency of smoking and age with the presence of plaques (P < .001). In the smoker group, 18.4% had measurable carotid artery atherosclerotic disease. The duration and frequency of smoking increased the percentage of carotid stenosis by 0.34% and 0.31% per year, respectively. Regardless of plaque presence and age increase, there was a linear association between the duration of smoking and an increase in carotid peak systolic and end diastolic velocities, which increased 0.62 and 0.65 per year, respectively. Conclusion: Current tobacco use has a strong association with carotid artery plaque and alterations in carotid hemodynamics in Saudi Arabian smokers.
Approximately 26.5% of Saudi Arabian men are current smokers, and the tobacco-related health problems are estimated to cost $176 billion per year in the Kingdom of Saudi Arabia. 1 Smoking is a significant public health problem and a recognized risk factor for carotid artery disease. It contributes to the incidence of stroke, which is considered to be the second-leading cause of death worldwide, according to World Health Organization reports. 2 The objectives of this study were to structurally evaluate the carotid artery and its hemodynamic alterations in male Saudi smokers, with B-mode and Doppler sonography.
Material and Methods
An Acuson X300 (Siemens Acuson Ultrasound, Malvern, Pennsylvania) ultrasound machine with a 7-MHz linear transducer was used throughout the study. B-mode and color Doppler ultrasonography measurements were made during the examination of all participants. A questionnaire and data sheet were used to collect the data on tobacco usage. This quantitative descriptive study was conducted from February 2011 to June 2013 at the King Abdul-Aziz Specialty Hospital in Taif, Kingdom of Saudi Arabia. The populations evaluated were Saudi smokers (n = 92) and nonsmokers (n = 29). Of the 92 smokers, 89% were medically asymptomatic; the remainder were hypertensive or diabetic or had known hypercholesterolemia. Exclusion criteria included patients with known coronary artery or other cardiac diseases. Simple, convenient systematic sampling was utilized to select all the participants.
Carotid arteries for all participants were examined according to a standard carotid sonography protocol. The participant was lying on an examination table in a supine position with a small pillow under his head. The participant’s head was turned slightly to the side opposite that being evaluated; all examinations were bilateral. Both the right and left carotid arteries were scanned with gray-scale imaging to anatomically locate the arteries; gray-scale imaging was used to evaluate the carotid artery lumen throughout its course to determine the presence or absence of atherosclerotic plaque as well as to assess the intima-media thickness.
Spectral Doppler scanning was then done to acquire the required measurements of common, internal, and external carotid artery (CCA, ICA, ECA, respectively) velocities with a Doppler angle of 60 degrees. This closely followed other published protocols in the literature.3,4 Peak systolic velocity (PSV) and end diastolic velocity (EDV) were measured in all vessels evaluated. Carotid stenosis was graded with published criteria. 4 A PSV <125 cm/s, even in the presence of plaque, was considered <50% diameter narrowing. A PSV >125 cm/s indicated >50% stenosis, and when the EDV was >140 cm/s, the stenosis was >80%. The absence of any blood flow signal was taken to be a total occlusion. A single investigator performed the majority of the duplex studies (95%), while another sonographer participated in 5%.
Data regarding smoking were collected though a questionnaire. SPSS 16.0 (IBM, Cary, North Carolina) was used to analyze the findings. Student t tests and scatter plot diagrams were used to calculate the statistical values of correlation between smoking and the carotid artery changes.
Results
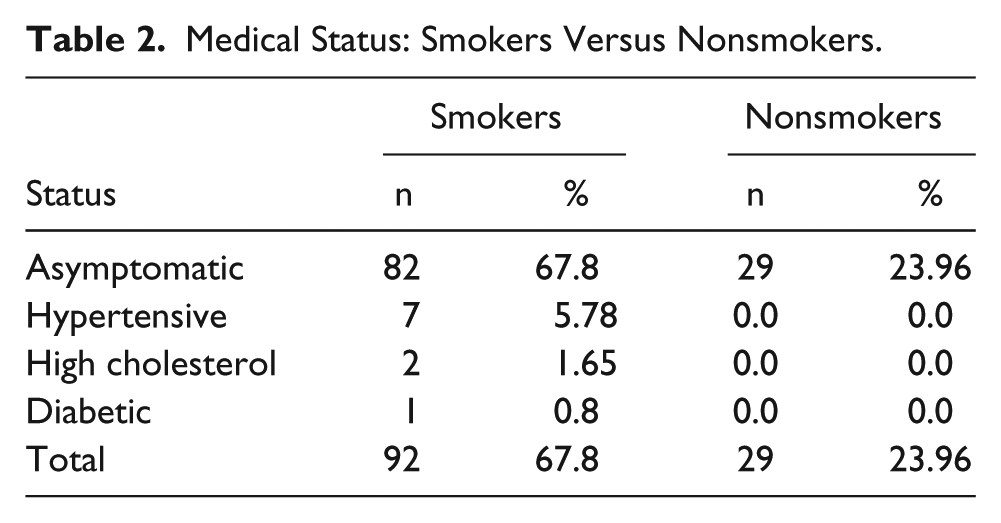
The 121 participants had a mean age of 36 ± 2 years (range, 19-100; Table 1). Table 2 summarizes the other classic risk factors for atherosclerotic disease found in the 92 smokers: 7 (7.6%) were hypertensive; 2 (2.2%) had hypercholesterolemia; and 1 (1.1%) was diabetic. All nonsmokers were medically asymptomatic. Table 3 summarizes the frequency of stenosis found in the carotid arteries of the smoker group. Of 92, 17 (18%) had measurable disease, with 12 (13%) having <50% diameter narrowing and 5 (5%) >50% diameter stenosis but <80%. Two subjects in the smoker group (2%) had a total ICA occlusion. An additional 4 subjects in the smoker group had minimal atherosclerotic disease versus significant thickening of the intima.
Study Variables: Smokers Versus Nonsmokers. a
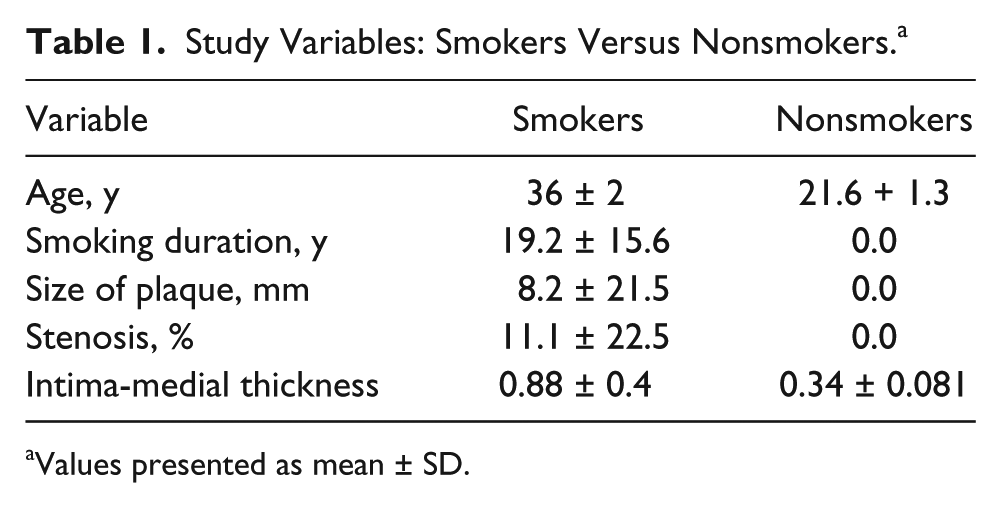
Values presented as mean ± SD.
Medical Status: Smokers Versus Nonsmokers.
Frequency of Narrowing/Stenosis in the Smoker Group.
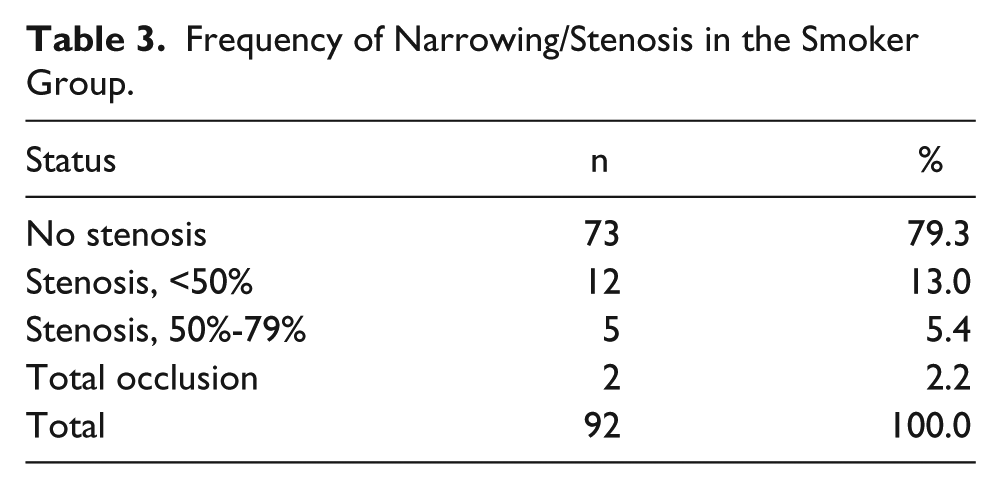
Table 4 summarizes the statistical analysis of the association between frequency of smoking (number of cigarettes per day) and age with the presence of plaque (P < .001). Figure 1 shows a scatter plot of the linear association between the duration of smoking and the percentage of carotid stenosis, which increased 0.34% per year. Figure 2 shows a similar scatter plot of the linear relationship between the frequency of smoking and the percentage of carotid stenosis, which increased 0.31% per unit frequency. Figure 3 summarizes the linear relationship between the duration of smoking and the increase of CCA PSV, which increased 0.62 cm/s/y. Figure 4 shows a similar linear association between the duration of smoking and the increase of CCA EDV, which increased 0.65 cm/s/y.
Statistical Relationship Between the Presence of Plaque and Evaluated Variables.
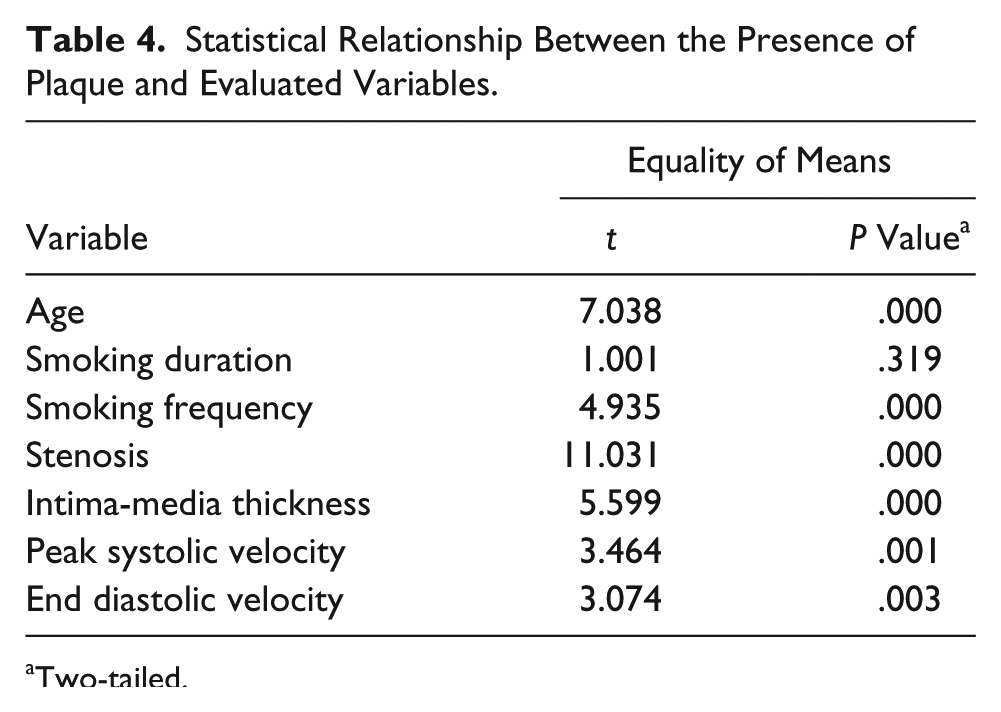
Two-tailed.
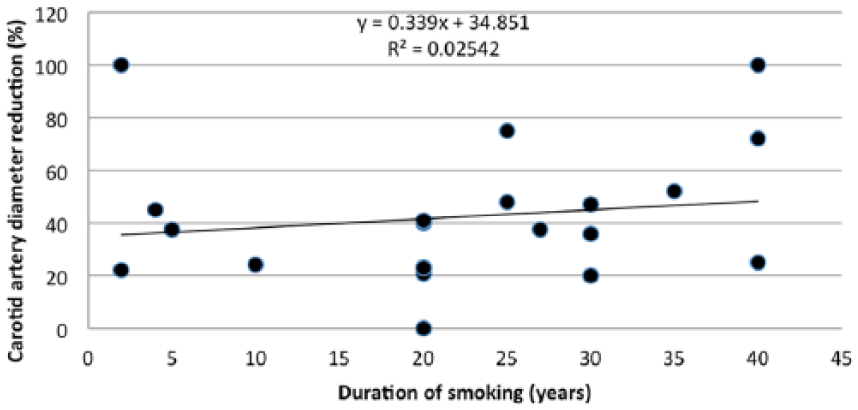
Graph showing the association between the duration of smoking in years and the degree of narrowing of the carotid artery.
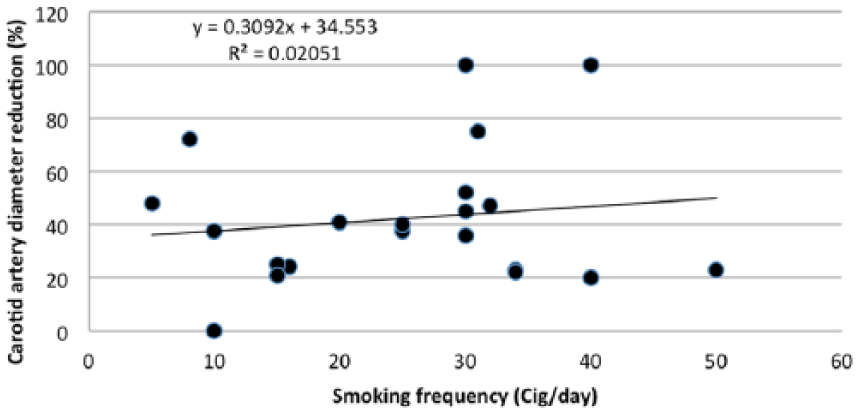
Graph showing the association between the frequency of smoking in cigarettes per day and the degree of narrowing of the carotid artery.
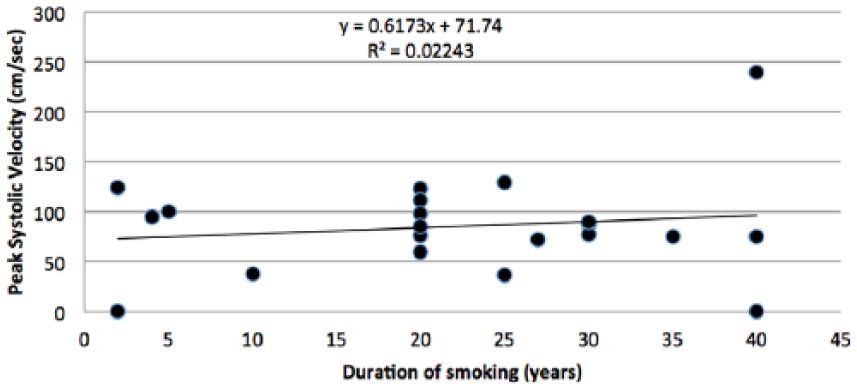
Graph showing the association between the duration of smoking in years and the peak systolic velocity in the common carotid artery.
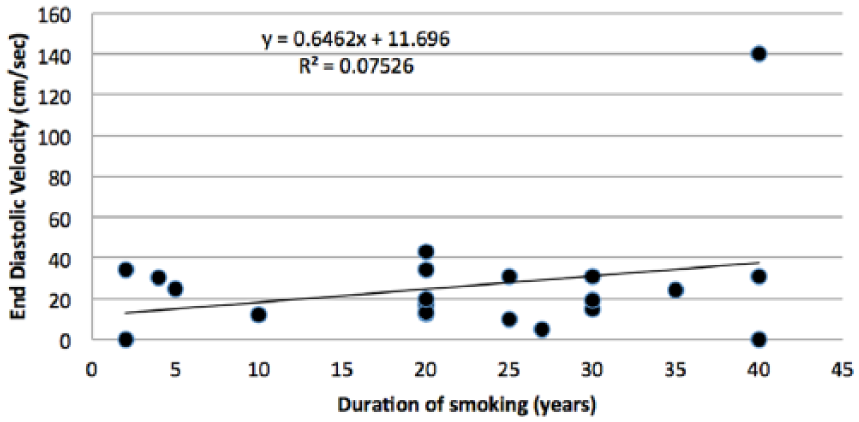
Graph showing the association between the duration of smoking in years and the end diastolic velocity in the common carotid artery.
For the entire group, the mean common carotid PSVs in smokers versus nonsmokers were 66.4 ± 3.0 and 59.2 ± 1.5 cm/s, respectively. The common carotid EDVs in smokers versus nonsmokers were 17.3 ± 1.5 and 14.5 ± 4.0 cm/s, respectively. Figure 5 summarizes the comparison of carotid artery velocities between a sample of 15 young smokers versus a sample of 15 young nonsmokers, all within the age range of 19 to 29 years. The mean PSVs in the smokers were 60.5, 57.4, and 76.0 cm/s in the CCA, ICA, and ECA, respectively. For the nonsmokers, the PSV velocities were 58.1, 55.6, and 68.4 cm/s in the CCA, ICA, and ECA, respectively. This trend to lower velocities was not statistically significant.
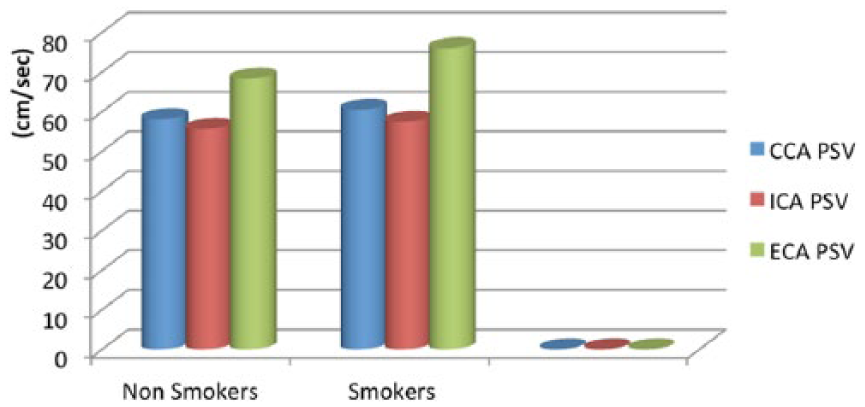
Graph comparing the common, internal, and external carotid artery (CCA, ICA, ECA, respectively) peak systolic velocities (PSVs) between nonsmokers and smokers.
Figure 6 summarizes the association between the presence or absence of plaque in the group of smokers and the resulting mean carotid PSV and EDV (P < .05).
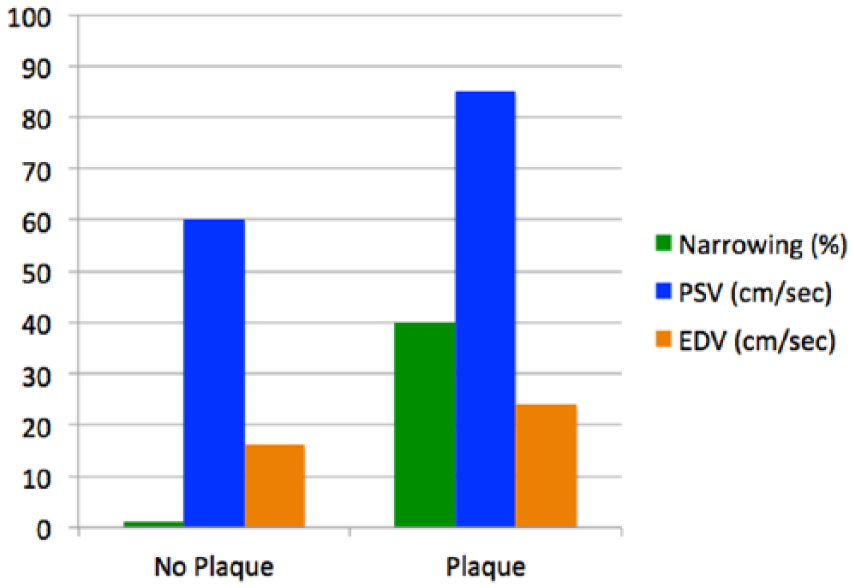
Graph showing the peak systolic velocity (PSV) and end diastolic velocity (EDV) as a function of the presence or absence of atherosclerotic plaque in the study subjects who smoked.
Discussion
The objective of this study was to evaluate the association of carotid artery structural and hemodynamic alterations with the frequency and duration of smoking in Saudi Arabian men. The significance of these carotid artery abnormalities is that they may ultimately have an association with more advanced arterial disease and stroke. The study found a strong significant association between smoking and the occurring of carotid plaques as well as carotid artery hemodynamics, as expressed in PSV and EDV measurements. The data showed a strong linear association between the duration of smoking and the percentage of carotid stenosis, which increased 0.34% per year, as well as between the frequency of smoking and the degree of carotid narrowing, which increased 0.31% per unit frequency. These findings are consistent with those of Barutcu et al., 5 whose results based on transcranial Doppler measurements suggested that smoking causes acute hemodynamic alterations in the common carotid artery. The data presented also agree with those of Tell et al., 6 who showed that among all participants, the prevalence of clinically significant (≥50%) internal carotid stenosis increased from 4.4% in never smokers to 7.3% in former smokers to 9.5% in current smokers (P < .0001).
This study also showed an association between the duration of smoking and increases in carotid PSV and EDV, which increased 0.62 and 0.65 cm/s/y, respectively. These findings are in line with those of Barutcu et al., 5 who found that PSV, maximum EDV, and time-averaged maximum velocity were all significantly increased after smoking. Cigarette smoking also was noted to significantly alter the CCA hemodynamics in nonsmokers, possibly as a consequence of enhanced adrenergic activity. To some extent, the results of this study also agreed with the findings of Mustafa, 7 who proposed that cigarette smoking is associated with carotid artery morphologic changes caused by significant impairment of the arterial endothelial function. This atherogenic effect leads to variability of blood flow velocity inside the CCA by increasing the PSV and EDV in a proportionally linear manner. The current study indicated that smoking increases both PSV and EDV in direct relation to the frequency and duration of smoking.
Comparing smokers and nonsmokers, this study showed an association between smoking and the increase in carotid velocity, even in young smokers. The findings for the entire group of subjects—that mean common carotid PSVs in smokers versus nonsmokers were 66.4 ± 3.0 and 59.2 ± 1.5 cm/s, respectively, and that the common carotid EDVs in smokers versus nonsmokers were 17.3 ± 1.5 and 14.5 ± 4.0 cm/s, respectively—are in agreement with Pereira et al., 8 who showed that smoking had an acute and significant effect on vascular function in young healthy individuals.
Conclusion
The data from this study suggest that smoking has a significant effect on carotid artery atherosclerotic disease and hemodynamics. The effects are measurable as a function of both the frequency and the duration of smoking, independent of age. This suggests that smoking is a significant risk factor for alterations in carotid artery hemodynamics and likely increased stroke risk.
Footnotes
Acknowledgements
We thank the King Abdul-Aziz Specialty Hospital, Taif, Kingdom of Saudi Arabia, for its cooperation and the opportunity to conduct this study.
Declaration of Conflicting Interest
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.