
Abstract
Peripheral arterial aneurysms may be true aneurysms, a dilation of the lumen lined by the remnants of the stretched arterial wall, or a false aneurysm (pseudoaneurysm), a penetration of the luminal wall with contained flow external to the vessel. Pseudoaneurysms are typically a result of blunt or penetrating arterial trauma, which includes a variety of iatrogenic injuries. This case report describes a traumatic psuedoaneurysm of the left internal carotid artery that occurred after a fall resulting in hyperextension of the neck. The psuedoaneurysm was undetected for three months until a sonographic examination for persistent neck pain showed the lesion. Endovascular repair of the pseudoaneurysm was done without complications.
Introduction
A true arterial aneurysm is an abnormal dilation of vessel to a lumen diameter greater than 1.5 times the native vessel lumen. They can involve any artery in the body, and venous and cardiac aneurysms may also occur.1–3 True aneurysms are generally secondary to various indigenous and exogenous factors including heredity, diabetes, obesity, hypertension, tobacco use, alcoholism, high cholesterol, copper deficiency, hematogenous infection, and increasing age.4–9 False aneurysms, or psuedoaneurysms, are typically the result of blunt or penetrating trauma, including a variety of iatrogenic injuries, with perforation of the arterial wall, and they are characterized by a collection of blood flow outside the lumen of the vessel contained by the surrounding soft tissue structures.10–15 A case is reported in the following of an internal carotid artery pseudoaneurysm ultimately detected during sonography approximately three months after a fall with hyperextension of the neck.
Case Report
A woman in her mid 70s was referred for sonographic evaluation of her carotid arterial system because of chronic, persistent pain in the left neck. Three months prior she had fallen backwards, striking her head on the ground and injuring her neck, with hyperextension of her neck posteriorly and to her right side. Cervical spine films at the time showed reversed lordosis secondary to muscle spasm; no fractures were identified (Figure 1). The patient was diagnosed with a whiplash injury and treated conservatively with a neck collar, muscle relaxants, and analgesics. While the symptoms of her whiplash injury subsided, she continued to have left-sided neck pain. Sonographic examination of her carotid arterial system was done using a Toshiba Nemio Ultrasound system (Toshiba Ultrasound, Tustin, California, USA) with a 14 MHz linear array transducer.

Lateral c-spine radiograph showing reversed lordosis secondary to muscle spasm.
Evaluation of the left carotid system showed a normal common carotid artery and external carotid artery. The left internal carotid artery (ICA) appeared markedly tortuous in its proximal segment (Figure 2). Approximately 1 to 2 cm distal to the bifurcation, note was made of an approximate 2 × 4 cm region with active blood flow characteristic of aneurysmal dilatation of the ICA (Figures 2 and 3). Color Doppler imaging within this region showed loss of normal antegrade laminar blood flow with disorganized, chaotic to-and-fro flow patterns (Figure 3); the distal ICA was seen to extend from this region with more normal flow patterns, giving the appearance of a pseudoaneurysm as opposed to a true aneurysm. No mural thrombus was identified. The most distal segment of the internal carotid artery was obscured by the angle of the mandibular ramus, making it difficult to evaluate its extent beyond this point. The patient was referred to a vascular surgeon who obtained a computed tomographic angiogram (CTA) at an outside facility. Computed tomography imaging without and with intravenous contrast was done with coronal and sagital reconstructions showing a 4.3 cm area of focal aneurysmal dilation arising from the proximal ICA, confirming the diagnosis of a traumatic psuedoaneurysm (Figures 4, 5, and 6). The patient had percutaneous endovascular repair of the pseudoaneurysm using a covered stent without incident.
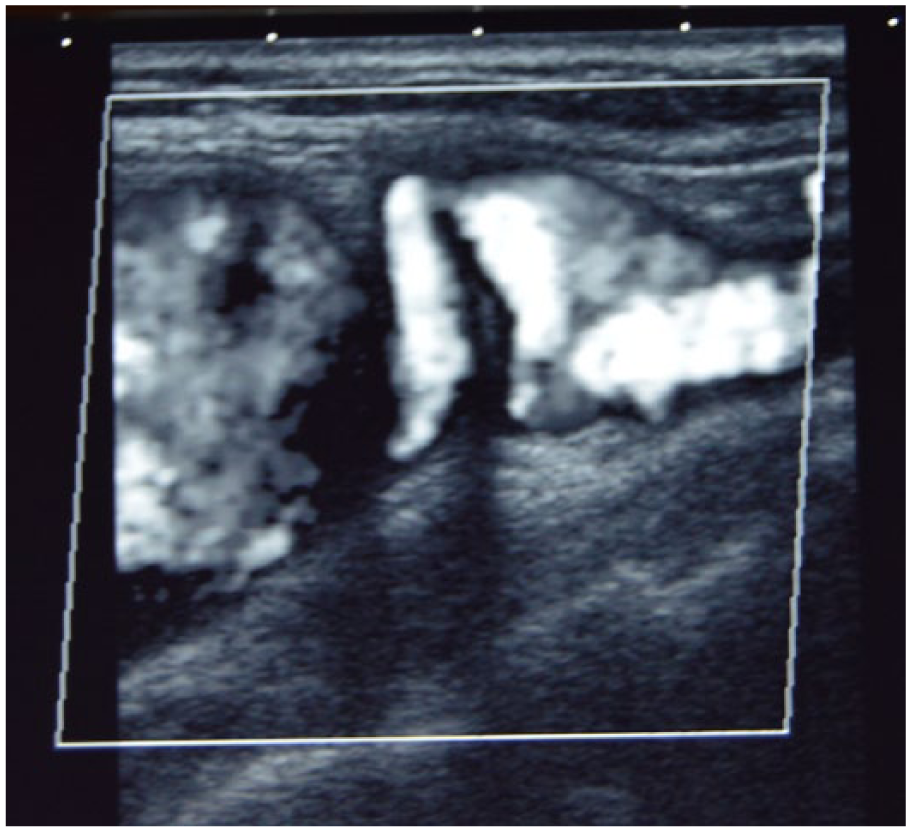
Sagittal color Doppler (displayed as shades of gray) image showing a tortuous proximal internal carotid artery (ICA); distal to the tortuosity is seen a large region of disturbed flow.
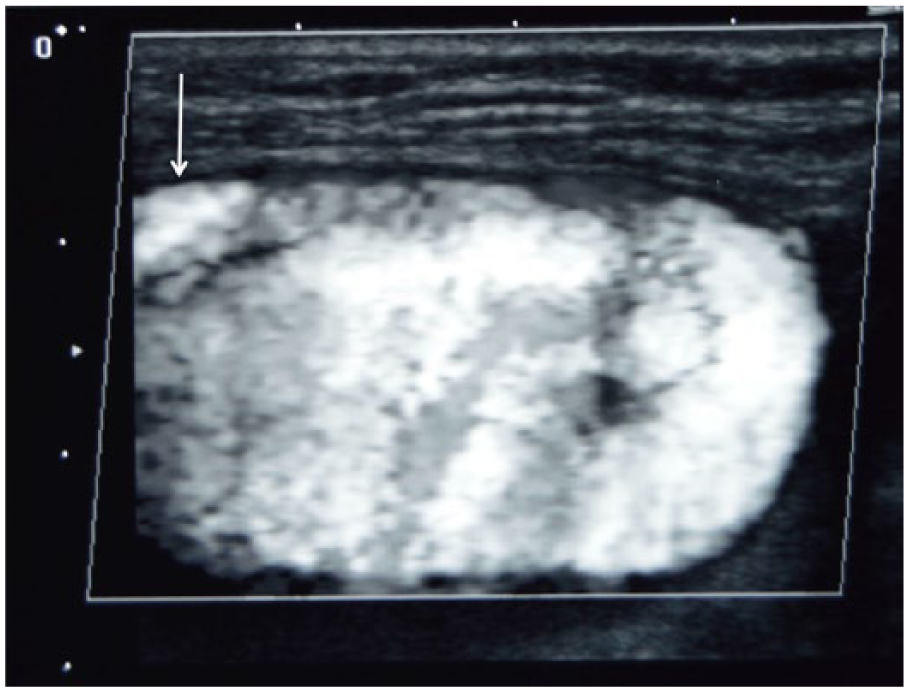
Sagittal color Doppler (displayed as shades of gray) image of the region of active blood noted in Figure 2, showing markedly disturbed flow within. The distal internal carotid artery (ICA) can be seen to extend from this region (arrow) with more normal flow patterns, giving the appearance of a pseudoaneurysm arising from the mid-segment of the ICA.
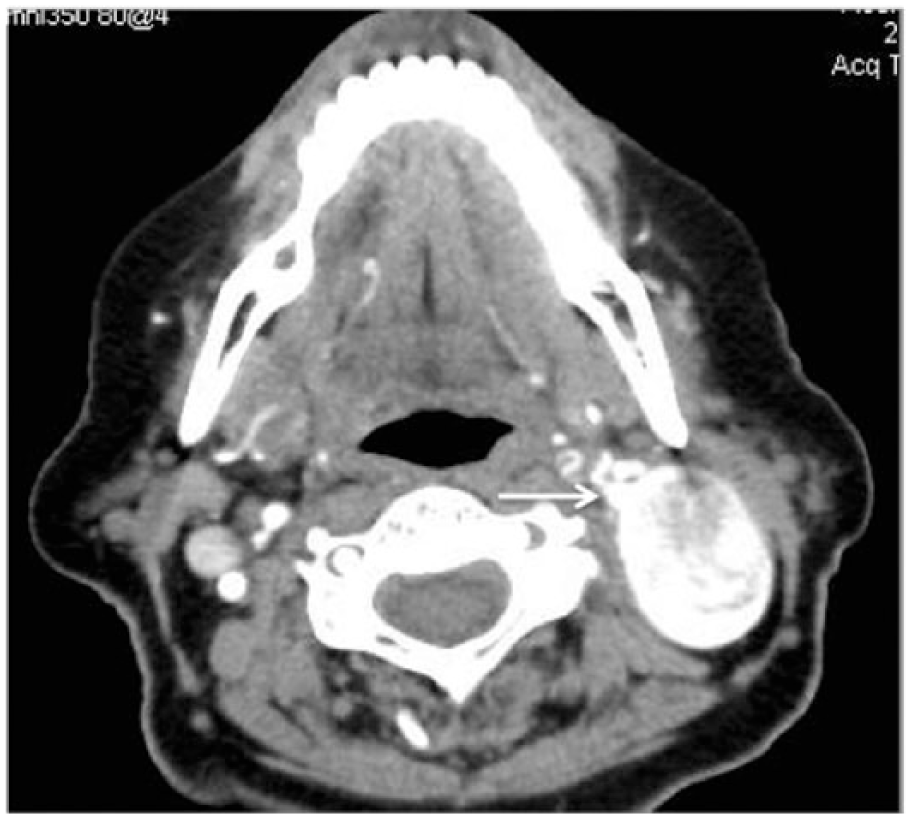
Axial computed tomographic angiographic (CTA) image of the pseudoaneurysm, showing its association with the internal carotid artery (arrow).

Sagittal computed tomographic angiographic (CTA) image of the pseudoaneurysm, again showing its close relationship to the internal carotid artery (arrow). (Horizontal streaks in the image are the result of metallic artifacts.)
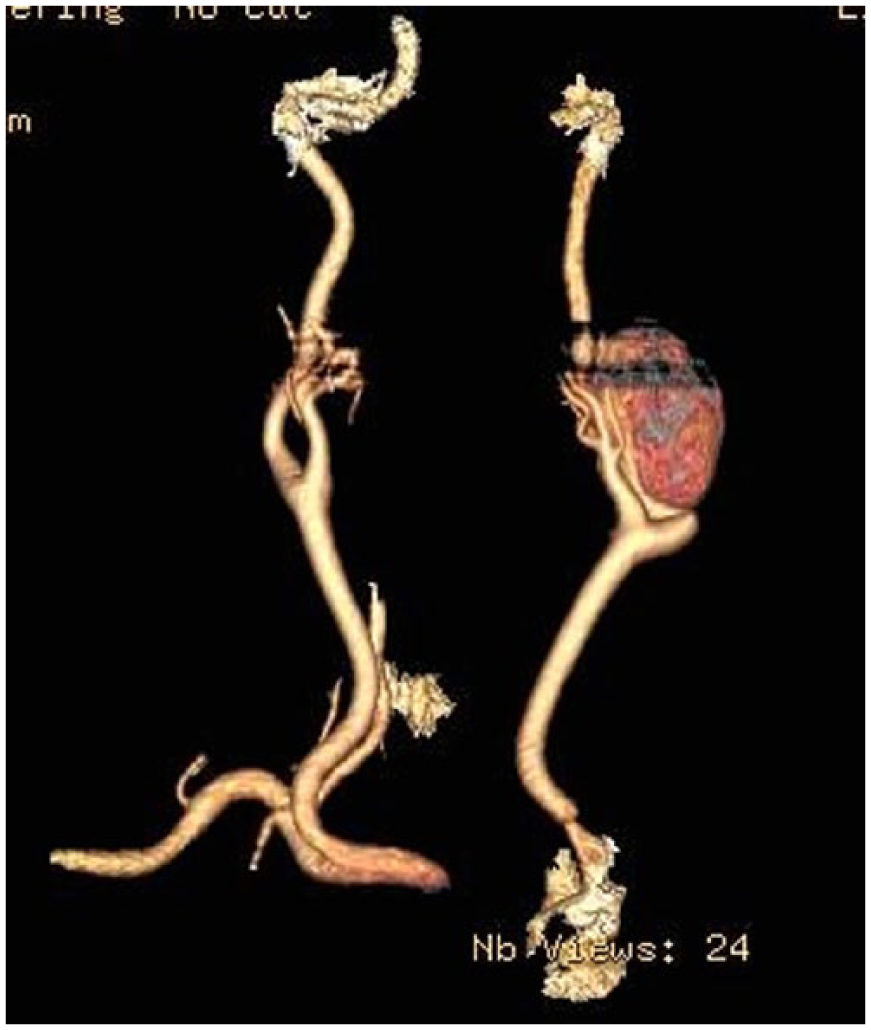
Three-dimensional computed tomographic angiographic (CTA) image reconstruction of the pseudoaneurysm. (Horizontal streaks in the image are the result of metallic artifacts.)
Discussion
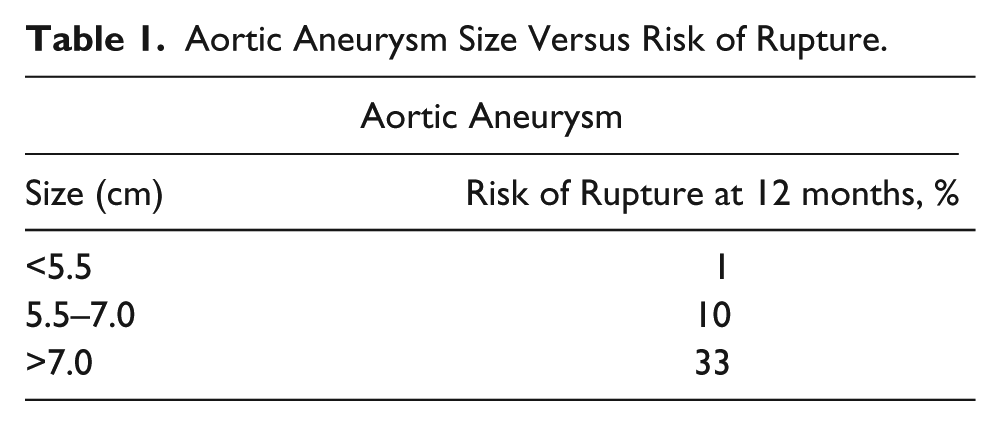
True aneurysms are a dilation of an artery contained within the remnants of the dilated (and sometimes degenerated) arterial wall. They are typically classified as either fusiform, a concentric widening of the artery (Figure 7), or saccular, a more sac-like circular or oval extension from a point of the arterial wall (Figure 8). The most common location for a peripheral arterial aneurysm is the aorta, with about 70% of these occurring within the abdomen. As the size of abdominal aneurysms increases, there is a subsequent increase in the risk of rupture2,16–18 (Table 1). Less commonly involved with aneurysmal dilation are the iliac, femoral, popliteal, carotid, subclavian, axillary, and brachial arteries, as well as visceral aneurysms involving the kidneys and/or mesentery. These other aneurysms have a lower risk of rupture, and except for the carotid and visceral arteries, rupture is very rarely fatal. 4 The most common complication of these other peripheral aneurysms is thromboembolism causing distal ischemia.
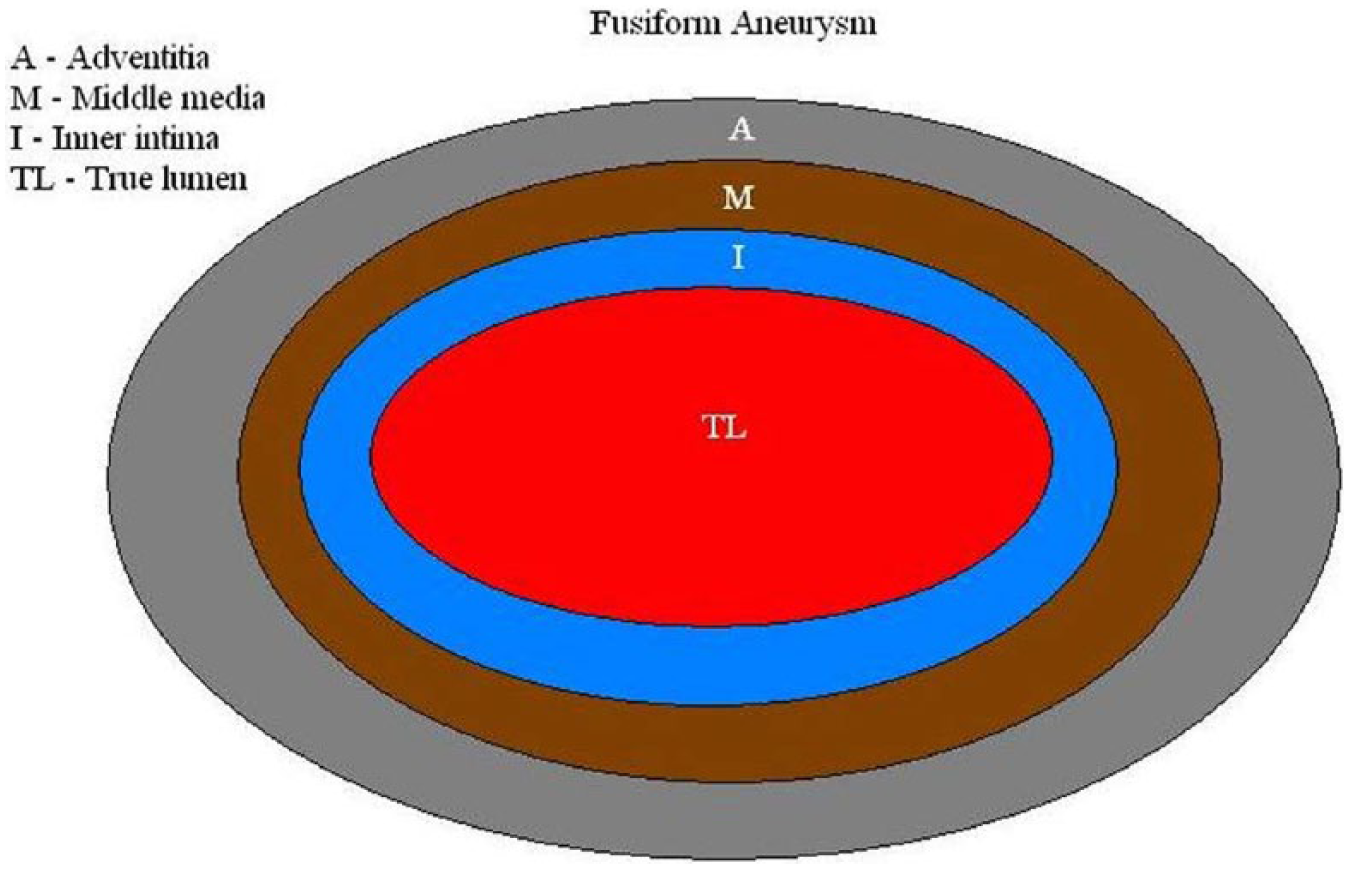
Schematic illustration of a typical fusiform aneurysm.

Schematic illustration of a typical saccular aneurysm.
Aortic Aneurysm Size Versus Risk of Rupture.
True aneurysms are generally secondary to various indigenous and exogenous factors including increasing age, heredity, diabetes, obesity, hypertension, tobacco use, alcoholism, high cholesterol, and certain mineral deficiencies.2–7 Mycotic aneurysms secondary to the hematogenous spread of bacterial infections can be contributory as well.8,9 True aneurysms usually result from slow, progressive weakening of the arterial wall due to the risk factors cited previously. Over time, arterial blood pressure causes dilation of the weakened blood vessel. As an aneurysm increases in size, tension within the arterial wall increases, and the risk of intimal dissection and rupture increases proportionately.
False aneurysms, or psuedoaneurysms, are the result of trauma that compromises the integrity and tensile strength of the arterial wall causing extravasation and a collection of blood outside of and adjacent to the vessel that is contained only by the surrounding soft tissues10–15 (Figure 9). These aneurysms can be secondary to blunt trauma, lacerations, or puncture wounds as well as iatrogenic trauma secondary to invasive medical procedures. Pseudoaneurysms may involve any artery in the body, and depending on their location, complications may be either life threatening or limb threatening. The most common complications are either thromboembolic in nature or involve excessive bleeding if the surrounding soft tissue containment is not adequate.10,13
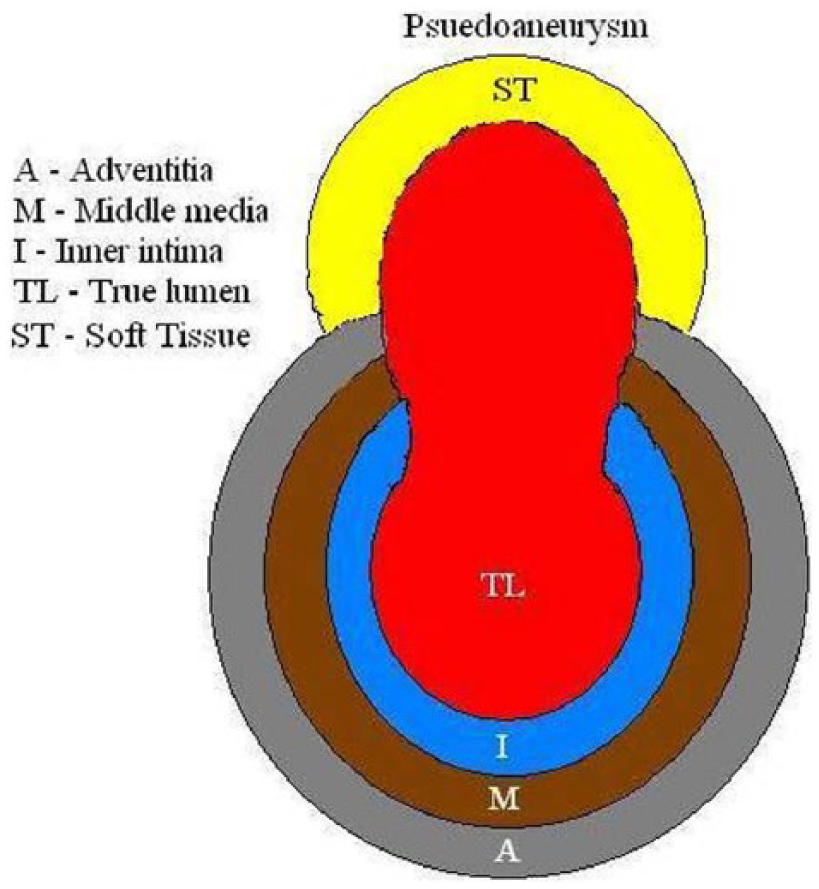
Schematic illustration of a pseudoaneurysm showing perforation of the vessel wall and flow outside the lumen contained by surrounding soft tissue.
A pseudoaneurysm of the carotid arterial system presents some unique management challenges not seen for other locations. It has become commonplace to treat most peripheral arterial pseudoaneurysms with ultrasound-guided thrombin injection, which causes near instantaneous thrombosis of the pseudoaneurysm.11,12 However, because of the risk of thrombosis of the associated native vessel during thrombin injection, this is not done for carotid artery lesions as a stroke would result. These lesions are best treated using percutaneous endovascular techniques, crossing the wall defect with a covered stent to seal the leak and spontaneously thrombose the pseudoaneurysm. If this is not successful, open surgical repair is done.
Conclusion
Trauma-induced pseudoaneurysms of the extracranial carotid artery system can be reliably diagnosed by sonography. Even in the case of a delayed diagnosis, as reported here, sonography leads to rapid identification of the lesion and prompt treatment. Sonography is widely accessible and cost-effective, and it is often the technique initially chosen for evaluation of most peripheral aneurysms, both true aneurysms and false aneurysms, with the exceptions of intracranial or intrathoracic aneurysms.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.