
Abstract
Objective:
The aim was to assess the structural and hemodynamic effects of smoking on the common carotid arteries (CCAs) in current smokers from Himachal Pradesh. In addition, it was important to determine any association between smoking duration, frequency, pack-years, and the occurrence of common carotid atherosclerosis.
Materials and Methods:
The study evaluated 50 current smokers for common carotid intima-media thickness (CIMT), plaque presence, and resistive index (RI) with sonography. The findings were compared with 50 healthy control patients, who had never smoked.
Results:
A positive association was observed between smoking and an increase in CIMT (P = .001) and occurrence of plaques (P = .007), with substantially higher mean CIMT values in smokers above 45 years (P < .05) in both genders (P < .05). No difference in overall RI was seen in both groups taken as a whole, while higher RI values (P < .05) were noticed in smokers exclusively above 60 years. A positive association was noted between smoking frequency, pack-years, and an increase in CIMT, RI, and occurrence of plaques. For every unit increase in the number of pack-years and smoking duration, there was a 0.01 unit increase in CIMT among the current smokers.
Conclusion:
This research provides evidence that smoking has a structural impact on CIMT while its hemodynamic effect is still unclear.
Keywords
Carotid atherosclerosis is a chronic condition that is caused by the deposition of fat in the vessel walls, resulting in the formation of plaque. The symptoms and pathologic substrate of carotid artery atherosclerotic occlusive disease were first described by Fisher in 1951. 1 Coronary artery disease (CAD) has been reported to be associated with extracranial carotid atherosclerosis. 2 Existing literature has shown that before the formation of plaque, in the coronary arteries, the atherosclerotic process develops correspondingly in the carotid arteries as well as in the aorta. 3 It has also been suggested that carotid atherosclerosis is significantly correlated with the extent of coronary artery atherosclerosis. This would suggest that thickening of the intima-media complex of carotid arteries not only reflects the local morphological alterations but also corresponds to generalized atherosclerosis. 4 Carotid artery distensibility, which decreases as atherosclerosis progresses, has a close relationship with general atherosclerotic changes. However, its evaluation is complex and can be time-consuming. In contrast, the arterial resistive index (RI), developed by Pourcelot, is a hemodynamic parameter that can be easily calculated from Doppler sonographic data. RI reflects the vascular resistance, which in turn is dependent on vessel distensibility. Thus, arterial intimal medial thickness (IMT) and RI play a complementary role in assessing the development of atherosclerosis within the vascular system. 5
Cigarette smoking is a public health problem and is a significant risk factor for atherosclerotic vascular disease. 6 Smoking has long been linked to atherosclerosis and other related health issues such as stroke and ischemic heart disease. In the Cardiovascular Health study, cigarette smoking was associated with a twofold increased risk for stroke recurrence in the elderly. 7 According to the World Health Organization (WHO), India is home to 12% of the world’s smokers. As per the Global Adult Tobacco survey conducted in 2016–2017, 19.0% of men, 2.0% of women, and 10.7% (99.5 million) of all adults were active tobacco smokers in India with marginally higher prevalence in the hill state. 8 In Himachal Pradesh, men accounted for 26.7 % of tobacco smoking and women and all adults accounting for 1.6% and 14.2%, respectively. 8
The study of carotid atherosclerosis and its relationship with smoking is a critical issue due to more than one-third of the adults in India using tobacco in one form or another. Smoking has been responsible for nearly 100 million premature deaths in adult men of ≥35 years, over the past decade, which accounts for nearly 4.52 trillion cigarettes and 40.3 trillion bidis (traditional form of cigarettes having tobacco hand rolled in leaves).9,10 In a representative rural study sample, from Himachal Pradesh, included 38 457 participants, and Agarwal et al concluded that those of a lower socioeconomic status were more likely to have abnormal behavioral risk factors, such as smoking. 11 Craven et al also demonstrated a strong independent correlation between the extent of carotid atherosclerosis measured by gray-scale sonography and the presence or absence of CAD documented with coronary angiography. 12 High-resolution sonography (HRS), which has proven to be a noninvasive, reliable, readily accessible, cost-effective, and preferred imaging modality, can easily determine common carotid IMT and plaque presence. Duplex sonography plays a role in evaluating the physiological and hemodynamic changes that take place in the extracranial portion of carotid arteries, by assessing peak systolic velocity (PSV), end diastolic velocity (EDV), and resistivity index. Since arterial endothelial dysfunction and resultant atherogenic effects, induced by smoking, are known to alter the hemodynamics of carotid arteries, Doppler was used to assess carotid hemodynamics by measuring RI. The implication of physiological alterations of the common carotid artery (CCA) is that it could potentially have an association with more advanced arterial disease, cardiovascular disease, peripheral vascular disease, and stroke.
Based on a review of the published literature, no study evaluating the CCA changes in current smokers and comparing them with nonsmokers has been conducted in Himachal Pradesh. The objective of this study was to determine how smoking influenced carotid intima-media thickness (CIMT) and carotid Doppler hemodynamics in current Himachali smokers. Likewise, it was important to investigate the relationship between time duration, the number of cigarettes smoked per day, pack-years (PY) of smoking, and the development of common carotid atherosclerosis.
Materials and Methods
This cross-sectional study was conducted over six months from May 2019 to October 2019 at a tertiary health care center.
Sample Size and Sampling Strategy
The sample size was calculated using an online sample size collection software (https://www.openepi.com/SampleSize/SSCC.htm). To detect to a difference of 0.5 standard division between the means of two groups, taking the baseline mean of CIMT was 0.06 ± 0.01 in the control group. Therefore, it was important to recruited 50 patients in each group, that is, 50 current smokers as cases and 50 nonsmokers. The cases and control participants were matched for age groups, sex, and body mass index (BMI) based upon the WHO’s BMI classification. These patients were recruited through convenience sampling technique. Subsequent patients who visited the study site were recruited in the study after obtaining their written consent.
The study included 100 participants, with 50 current smokers and 50 nonsmokers as controls of the same age group, sex, region, and BMI.
Parameters of Smoking Exposure
Current smokers were defined as participants who had smoked within the previous 30 days and/or had smoked 100 cigarettes in his or her lifetime. The smoking burden was represented by PY of smoking, defined as the average number of packs of cigarettes smoked per day multiplied by the duration of smoking in years. The smoking intensity was defined as the number of cigarettes smoked per day by current smokers. Cases were categorized based on the duration of smoking (<15 years and >15 years), PY (<5 PY and >5 PY), and frequency of cigarettes smoked per day (<5 cigarettes per day and >5 cigarettes per day). Data regarding tobacco usage were recorded in a data Excel sheet. The thickness of CIMT greater than 0.8 mm was considered abnormal. 13 The plaque was defined as a localized protrusion of the vessel wall extended into the lumen ≥1.5 mm. 14 Patients with diabetes, hypertension (WHO criteria), or on antihypertensives were excluded by measuring blood sugar levels and blood pressure, respectively, to eliminate the confounding effects. All the subjects were without any significant history of alcohol intake and cardiopulmonary disorders to negate their influence on the CCA blood velocities.
Data Collection
An informed consent was taken from all the participants enrolled in the study. All the examinations were performed by two examiners independently who were unaware of the smoking status of the participants. CIMT and RI values bilaterally were obtained twice by each examiner (Figures 1 and 2). The values were analyzed to derive the mean values for CIMT and RI for all the cases and control patients, thereby achieving reproducibility. A Philips Affiniti-50 ultrasound equipment system, with a 5 to 12 MHz linear transducer, was used to image all the participants, throughout the study. The CCA sonographic protocol used was based on the criteria established by the American Institute of Ultrasound in Medicine (AIUM). 15 After explaining the procedure to the participants, adequate positioning for carotid sonography was achieved by having patients lie supine, elevate their chest with a pillow, and the head being turned away from the side under evaluation. Bilateral CCAs were first examined in transverse views starting from origin to the vessel bifurcation.
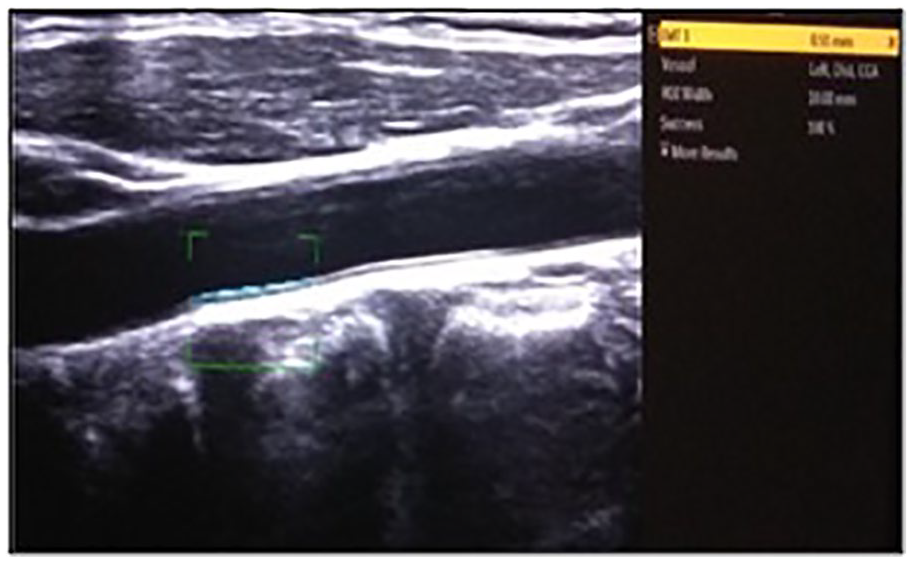
This image demonstrates the measurement of the CIMT of the left CCA (0.51 mm), using automated software. CCA, common carotid artery; CIMT, carotid intima-media thickness.
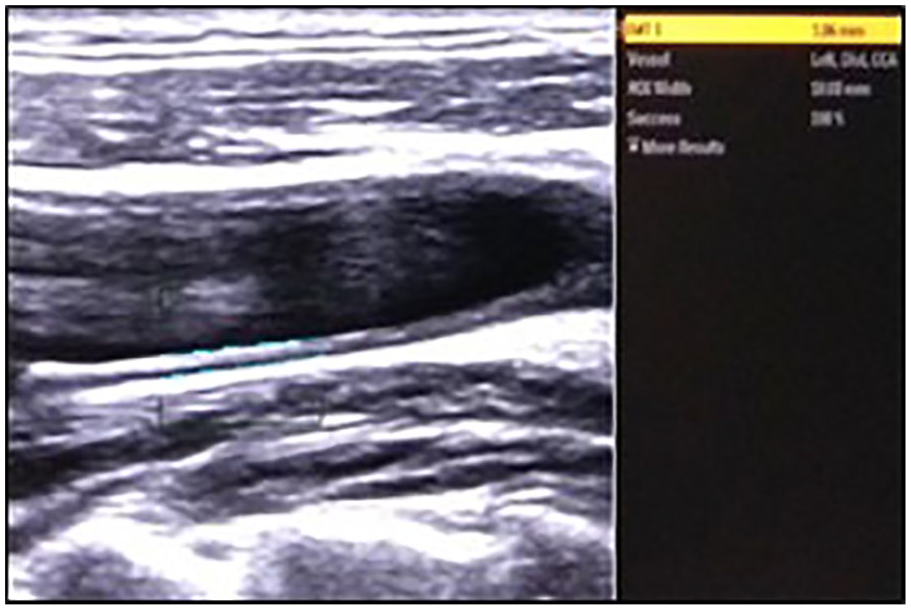
This image shows a gray-scale sonogram of an increased CIMT (1.06 mm) in the left distal CCA, of a smoking participant. CCA, common carotid artery; CIMT, carotid intima-media thickness.
Color Doppler was completed for both CCAs using a Doppler angle between 45° and 60°, with a sampling volume of approximately half of the vascular diameter. The color gain was optimally set so that color just reached the intimal surface of the vessel. The size of the sample volume box was kept between 2 and 3 mm and was aligned parallel to the direction of blood flow, not the vessel wall. The heel–toe technique was used to achieve the optimal Doppler angle by tilting the transducer from the head side to the toe side. All spectral Doppler tracings was taken in the same arterial segment where the CIMT measurements were taken. 16
The PSV (cm/s) and EDV (cm/s) were determined using the manual placement of the measurement calipers to obtain the most accurate results, and the RI was calculated according to Pourcelot equation (see Figure 3):

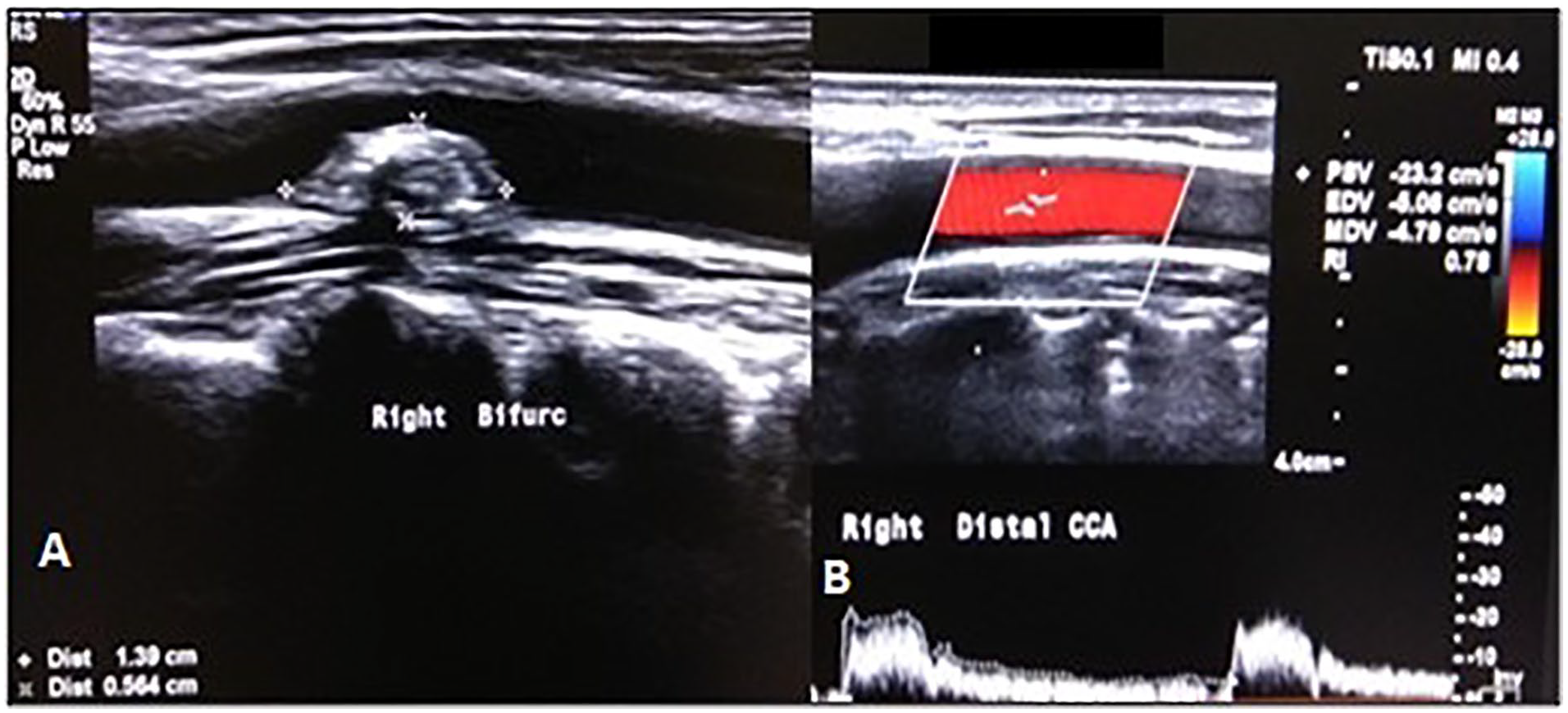
(A) The gray-scale sonogram depicts a heterogeneous plaque of size 1.4 × 0.5 cm at right carotid bifurcation, along the posterior wall. (B) The CD (Color Doppler) and SD (Spectral Doppler) image reveals an increased RI (0.78) in right distal CCA, for a smoking participant. CCA, common carotid artery; RI, resistive index.
Statistical Analysis
The analysis of the data was performed using the Statistical Package for the Social Sciences (SPSS) for Windows, version 17.0, released in 2008 (SPSS, Inc., Chicago, IL, USA). A chi-square test and Fisher’s exact test were used to determine associations between the categorical data (smokers and nonsmokers vs sociodemographic and variables like CIMT and RI), while Student’s t-test was used to compare the quantitative data (CIMT between current smokers and nonsmokers), after assessment of normality using Kolmogorov-Smirnov Test. The mean values of CIMT and RI were compared between current smokers and nonsmokers, between different categories of smoking duration, PY of smoking, and frequency of cigarettes smoked per day. Data were depicted graphically through scatterplots. All associations with a P value of <.05 were considered statistically significant (two-sided). Linear regression plots were used to depict any association between mean CIMT, duration of smoking, and number of PY.
Results
In this research study, 100 participants were successfully enrolled. The mean age in the smoker group was 47.1 + 13.7 years and in nonsmokers was 45.5 + 13.2 years. Table 1 depicts the age and gender distribution of the study participants. The majority were between 46 and 60 years of age (45%), followed by 31 to 45 years (27%) age group, and one-fourth of the participants (24%) were females. The total participants were equally divided into two groups (smokers and nonsmokers), matched by age and gender (P < .05; nonsignificant). The initial HRS evaluation depicted plaque in n = 15 (15%) participants as shown in Figure 3A. Out of 15, smokers comprised a significant number, n = 13 (86.67%) as compared with the nonsmokers, n = 2 (13.3%). This distribution was statistically significant on the Fisher’s exact test (P< .007).
The Demographics and Clinical Profile of the Study Participants.
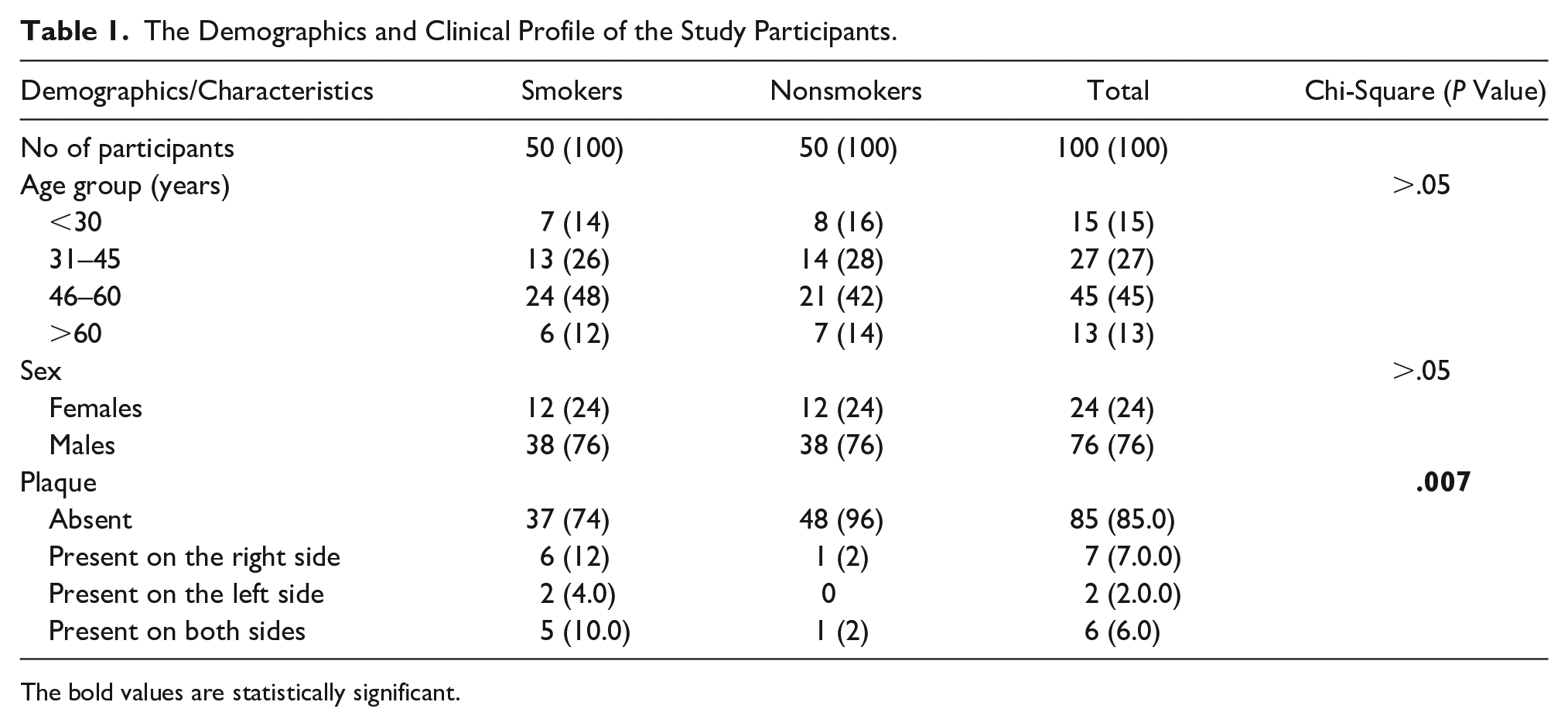
The bold values are statistically significant.
It was important to compare the left and right side of the vessel, as well as the average CIMT and RI, for smokers and nonsmokers (see Table 2). It was observed that the mean CIMT values were significantly higher (P = .001) in smokers, even though they were below the clinical standard of 0.8 mm. On the contrary, no significant differences were observed in the values of RI on the left or right side, as well as the overall mean among the two groups (see Table 2).
A Comparison of Carotid Parameters Between Smoking and Nonsmoking Participants.
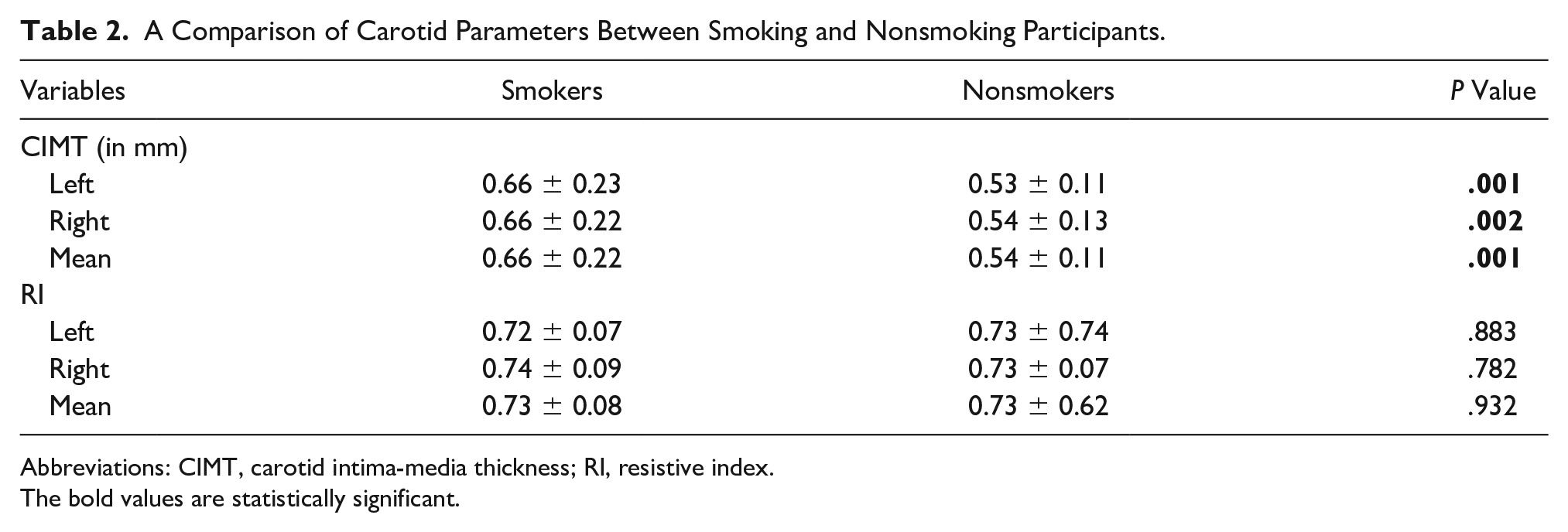
Abbreviations: CIMT, carotid intima-media thickness; RI, resistive index.
The bold values are statistically significant.
A further comparison was made for the carotid parameters among the two groups, based on age and gender stratification (see Table 3). In comparison with nonsmokers, the mean CIMT values were significantly higher among smokers of more than 45 years of age (P < .05) and both genders (P < .05). The mean RI values were substantially higher among smoking participants who were over 60 years of age, but no such correlation was found in those below that age.
The Comparison Between Smokers and Nonsmokers Based on Age and Gender and Various Carotid Imaging Parameters.
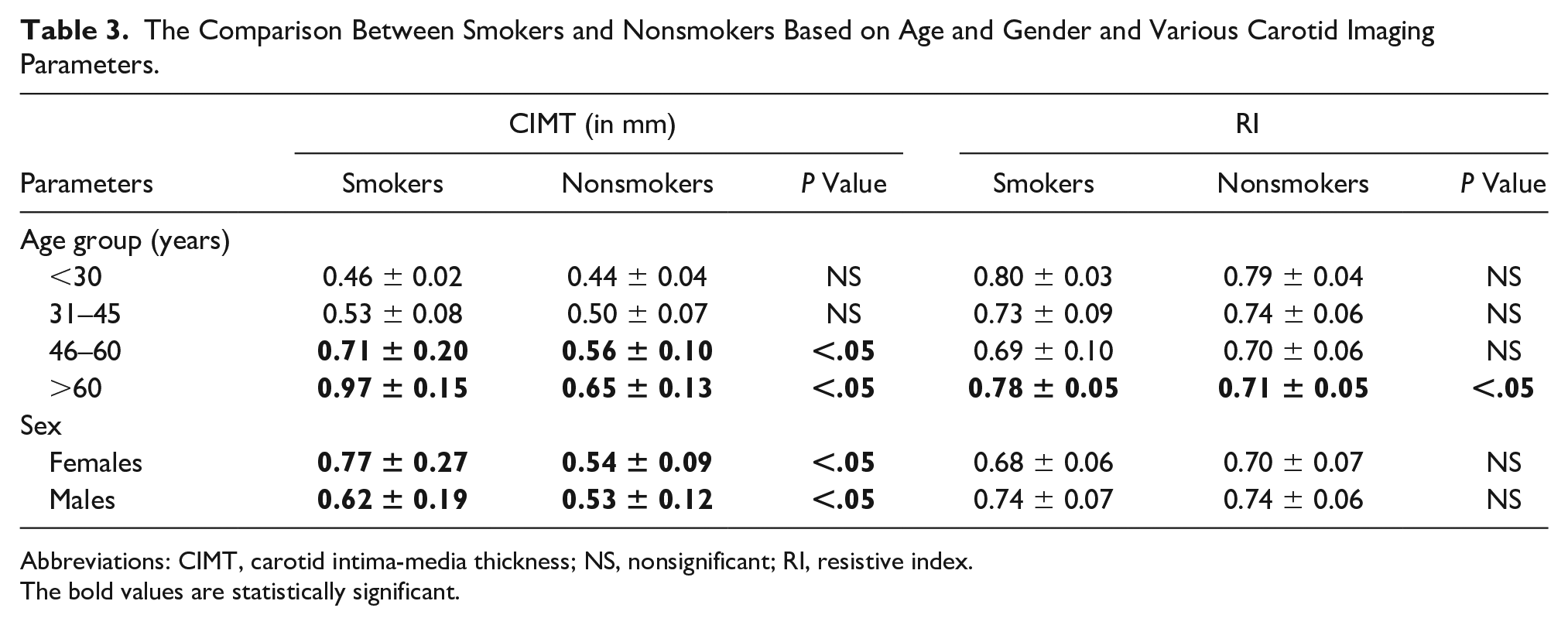
Abbreviations: CIMT, carotid intima-media thickness; NS, nonsignificant; RI, resistive index.
The bold values are statistically significant.
Also, any association between the carotid imaging parameters (CIMT, plaques, and RI), with the duration of smoking, PY of smoking, and frequency of cigarettes smoked per day, was assessed. With an increase in the duration of smoking (>15 years), PY (>5), and frequency of cigarettes smoked per day (>5 cigarettes per day), there was an increase in both the mean CIMT (though they were below the standard cutoff values) and RI. A strong linear association of CIMT with all these parameters was found while RI demonstrated a significant positive correlation with only PY and frequency of cigarettes smoked per day (see Table 4). Pack years depicted strong positive correlation with CIMT (r = .647, P < .05). Among smokers, the number of PY, and duration of smoking explained 44%, and 28% variability in the mean CIMT values as per the linear regression equation depicted in the scatterplots (see Figures 4 and 5).
The Statistical Relationship Between Carotid Sonographic Parameters and the Ascertainment of Smoking Exposure.
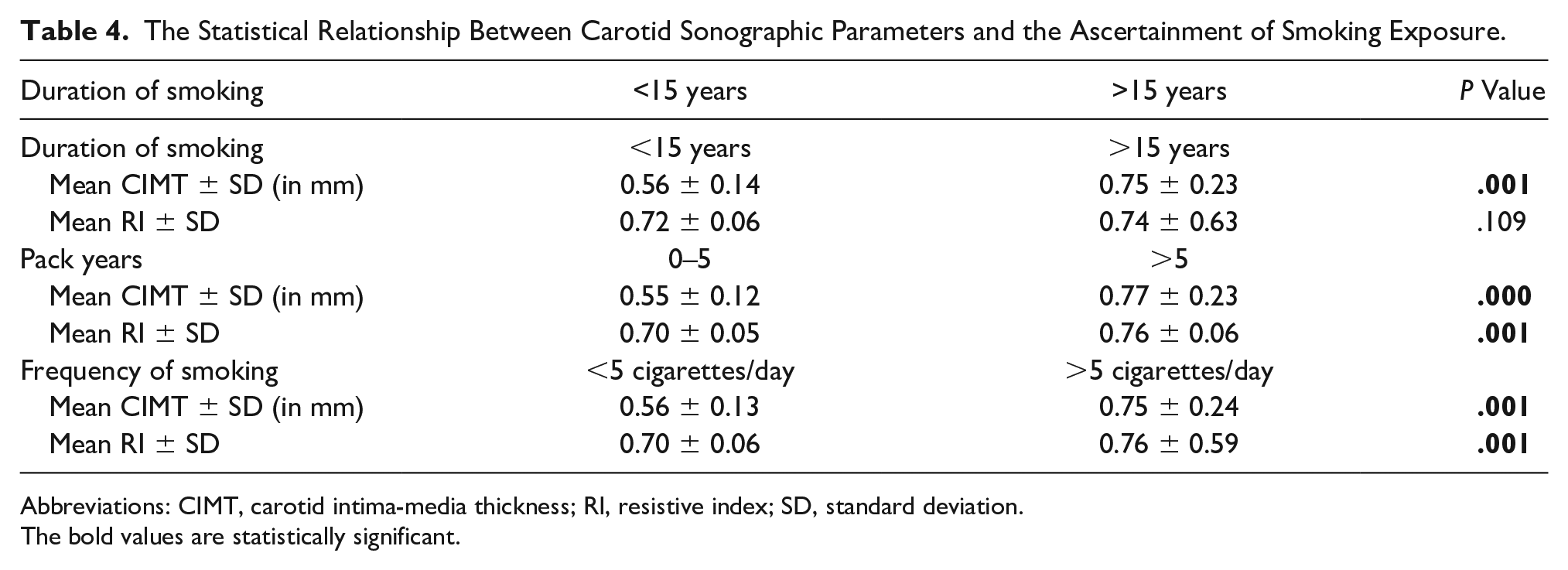
Abbreviations: CIMT, carotid intima-media thickness; RI, resistive index; SD, standard deviation.
The bold values are statistically significant.
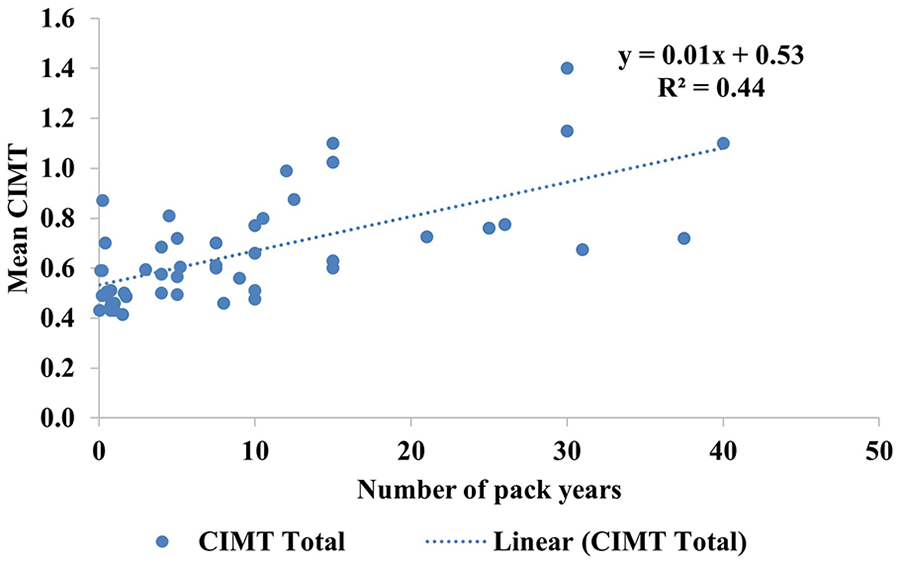
A scatterplot depicts a 44% variability in the mean CIMT values with the number of pack-years among the smoking participants. CIMT, carotid intima-media thickness.
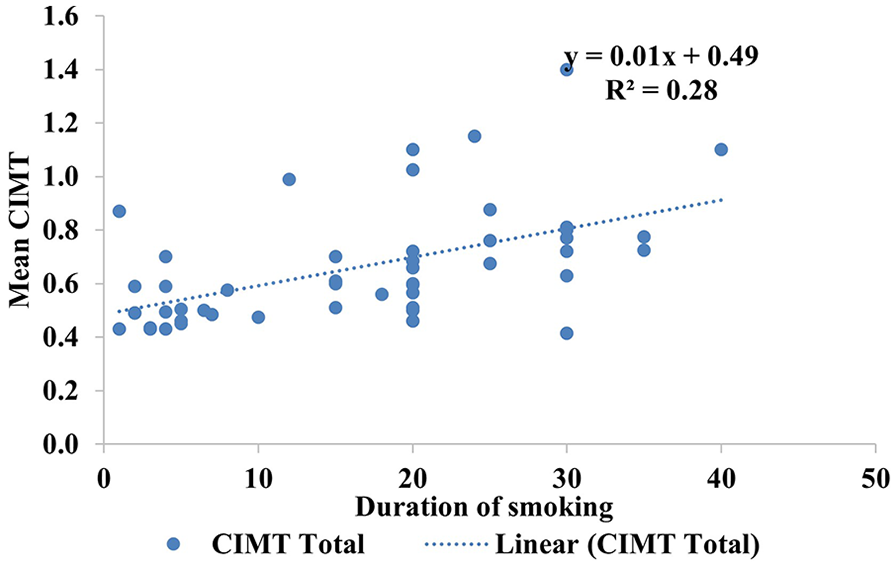
A scatterplot depicts a 28% variability in the mean CIMT values with duration of smoking among those participants. CIMT, carotid intima-media thickness.
On comparing the correlation between the presence of plaque in distal CCA and parameters of smoking exposure, statistically, significant differences were found with an increase in duration (P = .006), PY (P = .004), and frequency of smoking (P < .001), with more involvement on the left carotid artery (see Table 5).
The Association Between the Presence of Plaque in the CCA and Parameters of Smoking Exposure.
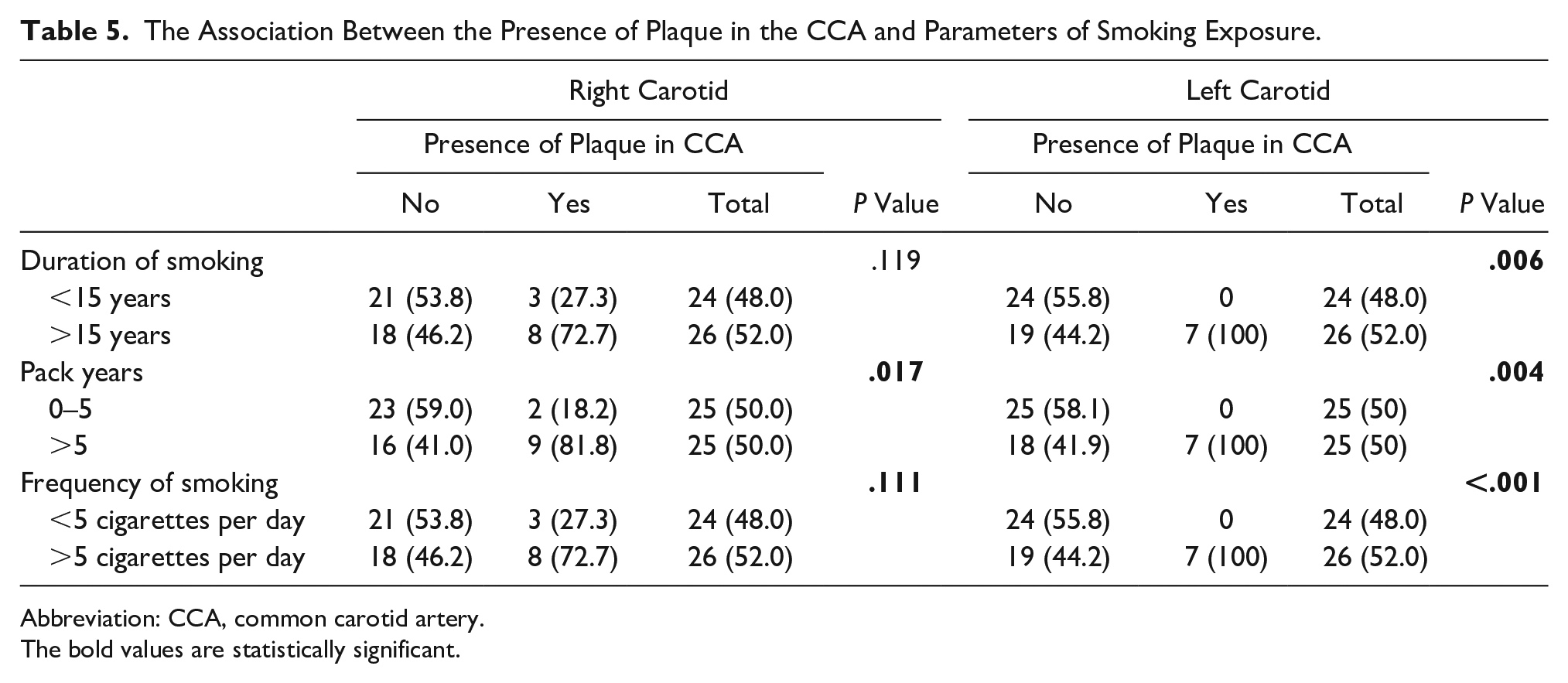
Abbreviation: CCA, common carotid artery.
The bold values are statistically significant.
Discussion
Smoking has been recognized as a strong risk factor for atherosclerosis in general and cardiovascular diseases in particular. The present study was conducted to evaluate common carotid atherosclerosis, in current smokers which revealed an association with smoking burden and smoking intensity, among these participants. This study was the first of its kind that focused exclusively on participants from Himachal Pradesh. The data allowed for a calculated CIMT and RI in bilateral carotid arteries and mean values to compare with results from Kitamura et al. They had observed that consideration of both the right and left carotid arteries would improve the prediction of cardiovascular disease, given the data collection with extensive parameters. 17
An increase in CIMT, measured with sonography, is considered a means to reflect early systemic atherosclerosis. 18 Although mean CIMT values observed in the smokers in the present study (i.e., 0.66 ± 0.22) were below atherosclerosis cutoff, they were significantly higher than the nonsmokers. It can be elucidated by the fact that most of the smoking participants included in the study were less than 60 years of age and likely in their early stages of atherosclerosis. However, a substantial difference in the CIMT values (P = .001) and the presence of plaques (P = .007) between the two groups indicate that smoking has a significant structural impact on the CCA.
Increased CIMT and complex plaque characteristics are well-known risk factors for cardiovascular disease, and the presence of arterial plaques represents an advanced stage of atherosclerosis, as well as a more powerful predictor of cardiovascular events. 19 In this study, there were 15 participants who had plaques, in the distal CCA. Out of those 15, smokers comprised a significant number, 13 (86.67%) all of whom were older (>60 years) and chronic smokers. This would indicate that smoking leads to a progression of atherosclerosis by initially increasing CIMT and gradually developing plaques, in these participants.
The findings of this study demonstrated that an increase in the smoking intensity and burden in current Himachali smokers significantly increased CIMT (P = .001) and the development of plaques (P = .001). These study results were comparable with Oshunbade et al, who reported that current cigarette smoking and smoking intensity were associated with a higher incidence of stroke and increased CIMT (carotid atherosclerosis), after adjusting for age and gender. 20
It was also observed that for every unit increase in the number of PY and duration of smoking, there was a 0.01 unit increase in mean CIMT among current smokers. The results obtained from this study were in agreement with Kianoush et al, 21 who noted the associations of cigarette smoking with subclinical inflammation and atherosclerosis. In the Brazilian longitudinal study of adult health, they concluded that CIMT was significantly higher among current smokers (β = 0.03; 95% confidence interval [CI], 0.02–0.04; P < .001) compared with nonsmokers. 21 They also observed that each 5-PY increase in smoking was associated with higher CIMT among ever smokers with increasing trends among current smokers. 21
In the present analysis on current smokers, mean CIMT values were significantly higher for those 45 years of age (P < .05) compared with nonsmokers. To some extent, the present observations matched Li et al 22 who revealed that if CIMT represents vascular age for an individual, current smokers were about 6 to 7 years older than nonsmokers in terms of their respective vascular ages (0.052–0.057 mm difference in CIMT between current smokers and nonsmokers divided by age-related change 0.008 mm/year in nonsmokers). 22 They highlighted that the adverse effects of age and metabolic syndrome on CIMT were intensified by cigarette smoking, such that the impact of age and metabolic syndrome on CIMT in current smokers was much greater than in nonsmokers. 22
In terms of hemodynamics, Barutcu et al had reported significant alterations in the pulsatility index (PI) and RI of CCA, 10 minutes after smoking and was probably a consequence of the enhanced adrenergic activity. 23 The RI is used to characterize an arterial waveform and both in vitro and in vivo studies showed that the RI is related to vascular resistance. 24 RI is a hemodynamic parameter that can be easily determined by Doppler and reflects local vessel wall extensibility and the related vascular resistance. Available literature shows a correlation between increasing RI values and both arteriosclerosis risk factors and clinical outcomes. 25 In contrast, these participants demonstrated no difference in overall RI, with both groups taken as a whole. In the study, they did demonstrate a statistically significant higher mean RI values (P < .05), which was seen in smokers, over 60 years of age.
The findings of the present study also demonstrated that an increase in smoking intensity and burden, among Himachali smokers, significantly increased the RI which in turn reflected an increase in blood flow volume within the CCA. This is likely due to increased adrenergic activity and was also reported by Alzimami et al. 26 These findings are also in line with Babiker’s findings, which showed a change in carotid hemodynamics in the form of a rise in both PSV and EDV in direct relation to frequency and duration of smoking. 27
Limitations of the Study
This cohort study was not without limitations. First, this study included only current smokers as participants. Second, since convenient sampling was used, it was only possible to consent 25% female participation as part of the study sample. The cross-sectional nature of this study does not allow for an evaluation of the progression of CIMT and RI changes caused by smoking. Thus, the findings of this study cannot be generalized to a larger population. A long-term follow-up study is recommended to evaluate this relationship.
Conclusion
This research would indicate that smoking has a structural impact on CIMT, in this particular cohort. It induced morphological alterations in the CCA of these participants, while the hemodynamic effect on the CCA is unclear, in these current smokers. The increase in CIMT and plaque formation for those current smokers, from Himachal Pradesh, could be attributed to smoking. The global importance of prevention and cessation of cigarette smoking cannot be overstated.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.