
Abstract
Variation in the origin of arteries is a fairly common occurrence. Some of these variations are considered inconsequential, whereas others can have serious implications for medical procedures. The authors present an unusual case demonstrating an anomalous branching of the superior thyroid artery from the distal common carotid artery.
Sonography, a proven imaging modality for evaluating the extracranial vascular network, is used extensively in examining the carotid arteries. These examinations include using B-mode imaging to evaluate the walls of the vessels and to look for areas of narrowing caused by various disease processes. Color Doppler is used to obtain a general idea of the hemodynamics of the blood flow within the vessels, and spectral Doppler is used to acquire detailed measurements of flow velocities. When used together, these sonographic imaging techniques provide the physician with accurate, reliable information on the structural integrity and the hemodynamics of normal and diseased vessels. The sonographers performing these examinations need extensive knowledge of the associated vascular anatomy and the more common and uncommon anatomical variants that may be encountered.
Case Report
A man in his early 70s presented to the sonography department of an outpatient medical clinic for evaluation of his carotid and vertebral arteries after experiencing recent episodes of dizziness and vertigo. Previous medical history was unremarkable.
Procedure
Evaluation of the carotid and vertebral arteries was performed using a Philips HD11XE (Bothell, Washington) scanning system with a 9.0-MHz linear array transducer. Gray-scale images were obtained in both the longitudinal and transverse anatomic planes, as well as Doppler assessment (spectral waveform analysis and color flow) of vessel hemodynamics.
Sonographic Findings
The peak systolic velocity was 105 cm/s for the right common carotid artery (CCA) and 88 cm/s for the right internal carotid artery (ICA). Possible retrograde flow was noted in the right vertebral artery. The peak systolic velocity was 94 cm/s for the left CCA and 107 cm/s for the left ICA, with atherosclerotic plaque of no overall hemodynamic significance seen in the left carotid bulb and at the origin of the left ICA. Antegrade flow was noted in the left vertebral artery. At the level of the distal right CCA, a branch of the artery was noted to follow a descending path toward the superior aspect of the right thyroid gland (Figure 1). Color and spectral Doppler interrogation of this anomalous artery demonstrated arterial blood flow directed toward the thyroid gland (Figures 2 and 3, respectively). A tentative diagnosis was an aberrant branching of the right superior thyroid artery from the right CCA, instead of the normal origin from the right external carotid artery (ECA). A computed tomography (CT) angiographic scan with contrast was recommended by the interpreting physician to corroborate the findings of the reversed flow in the right vertebral artery and to verify the aberrant origin of the right superior thyroid artery. The CT examination determined that the flow in the right vertebral artery was actually antegrade. In addition, the procedure confirmed the anomalous origin of the right superior thyroid artery from the right CCA (Figure 4).
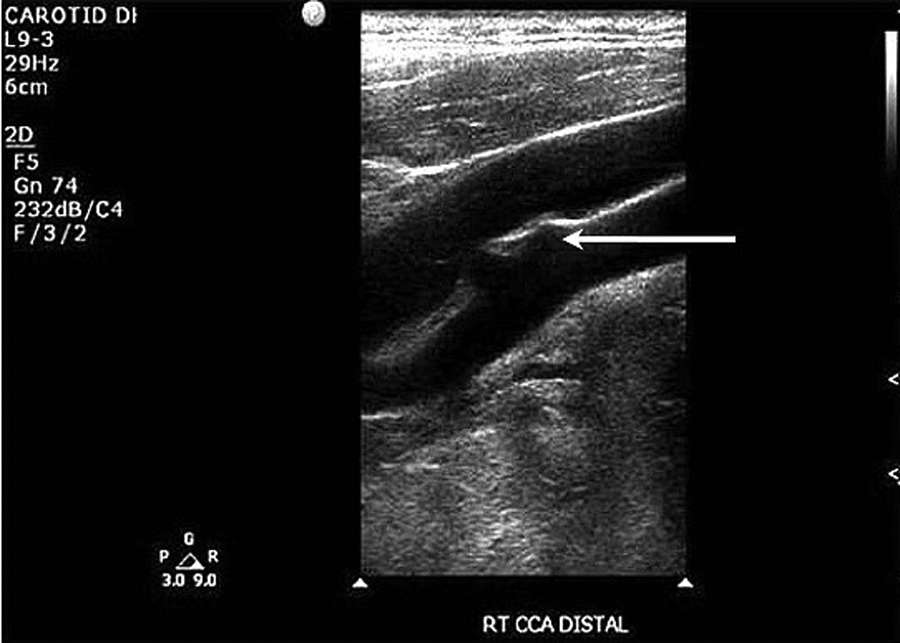
Longitudinal image of the right distal common carotid artery (CCA) demonstrating the anomalous origin of the superior thyroid artery.
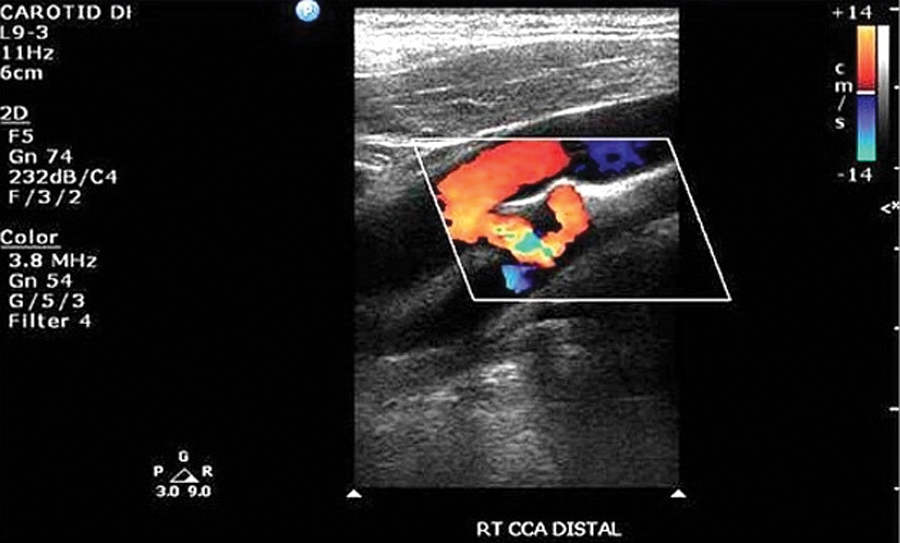
Color Doppler image showing flow in the right superior thyroid artery.
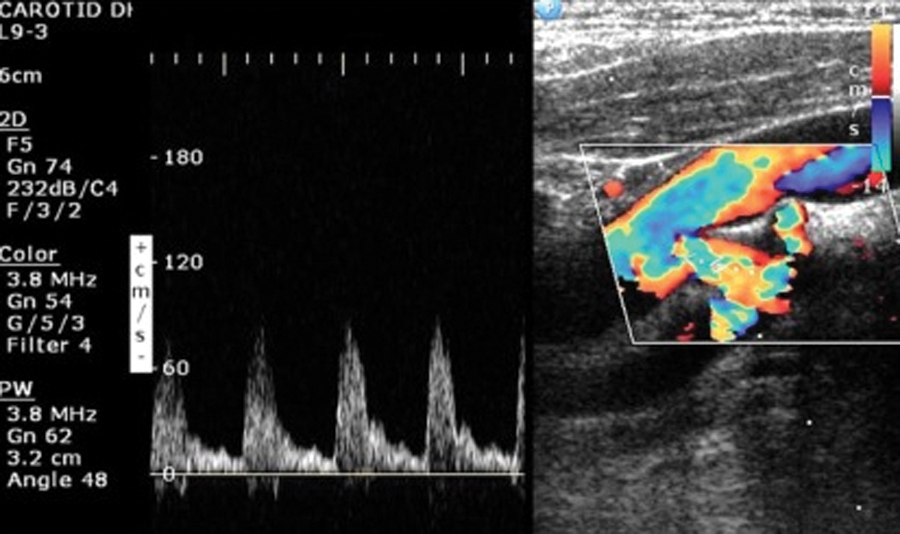
Spectral Doppler interrogation of the right superior thyroid artery demonstrating ample arterial blood flow.
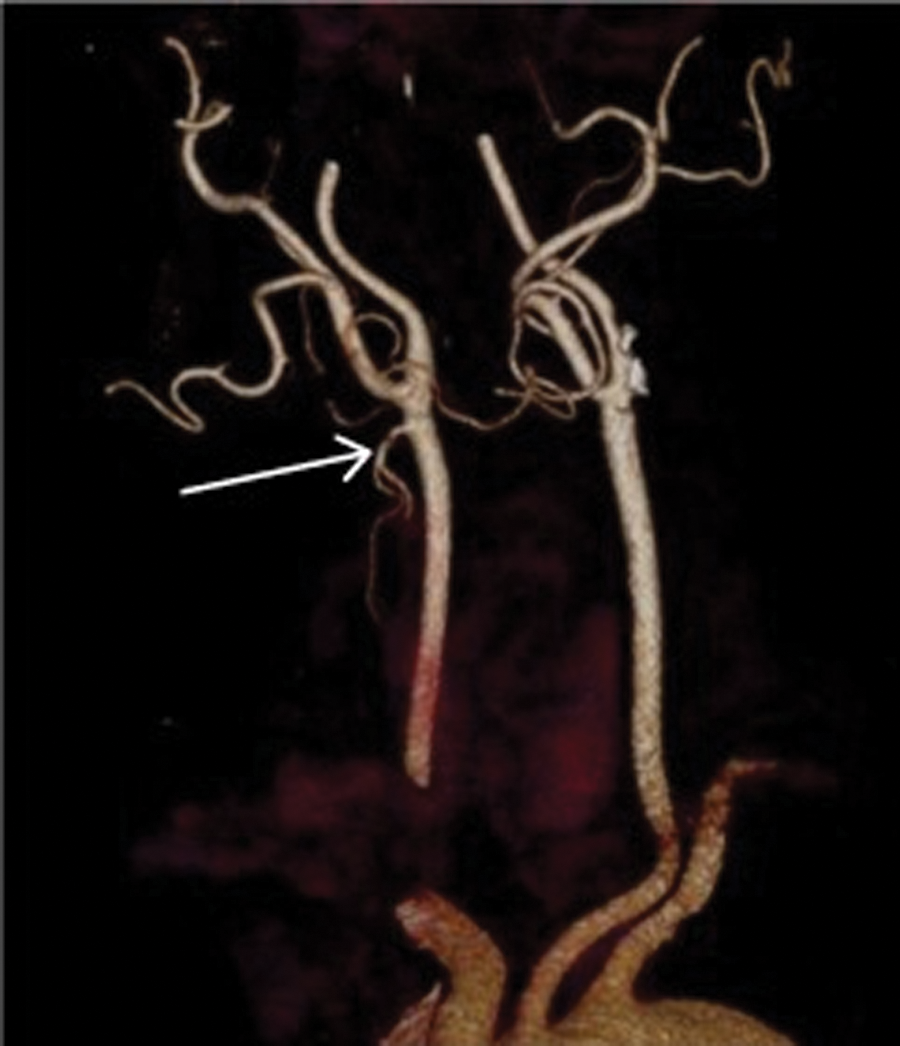
Computed tomography angiographic image clearly delineating the unusual origin of the right superior thyroid artery. This is an anterior view rotated approximately 40 degrees to the patient’s right.
Discussion
Understanding normal extracranial and intracranial vascular anatomy is essential for the vascular sonographer to perform imaging studies efficiently and successfully. In addition, because of the highly vascular nature of the neck’s anatomy, surgical procedures demand a detailed roadmap of the vascular systems to enable the surgeon to proceed with the best possible approach to avoid or minimize the risks of severe blood loss, especially in variations of the normal vasculature.
Arising from the aortic arch, the innominate artery gives rise to the right CCA and the right subclavian artery. The left CCA branches directly from the aortic arch. The right vertebral artery originates from the right subclavian artery, and the left vertebral artery branches from the left subclavian artery, which arises directly from the aortic arch. The common carotid arteries course superiorly in an oblique plane and bifurcate at the level of the fourth cervical vertebra, at which point the ICA and ECA provide blood flow to the brain and the face and portions of the neck, respectively. Although the CCA and extracranial portion of the ICA normally have no branches, the ECA begins to branch almost immediately from its takeoff, with the superior thyroid artery as the first branch, and an additional seven branches noted as part of the normal anatomy. 1
In its usual pathway, the superior thyroid artery initially courses superior and posterior for a short distance before traveling in its customary inferior and anterior course (Figure 5), where it ultimately provides the superior portions of the respective thyroid lobes with blood rich in nutrients and oxygen. 1 Aberrant or anomalous origins of the branches of the superior thyroid artery are uncommon, with the literature revealing origins from the ICA and CCA as the most common sites. Akyol et al 2 reported a case of the left superior thyroid artery arising from the left common carotid artery, which was discovered during neck surgery. Additional research at Akyol’s institution revealed a 1% occurrence of this anomaly in approximately 200 neck surgeries. Won et al 3 reported a rare case of bilateral origin of the superior thyroid arteries from the common carotid arteries. Anitha et al 4 dissected the necks of 50 cadavers and reported that 21% of the superior thyroid arteries demonstrated an anomalous origin. A similar dissection of 100 cadavers by Natis et al 5 revealed an atypical origin of the superior thyroid artery in 12% of the specimens.
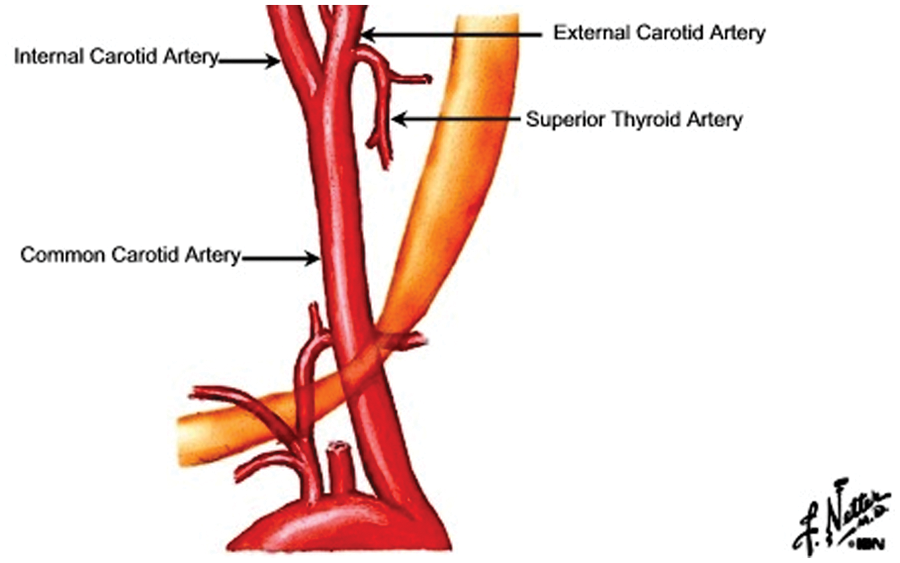
Anterior view of the origin of the superior thyroid artery. 9 Image reproduced with permission from Icon Learning Systems, LLC.
Although the focus of this case study is on the superior thyroid artery, this vessel is not the sole vascular structure that may have an aberrant origin when considering vascular structures of the neck. Knowledge of other variations in the neck’s vascular anatomy is very important for sonographers, physicians, and especially surgeons. Honardar and Meiches 6 reported a case in which the ascending pharyngeal arteries were noted to arise from the ICA in a patient being assessed for loss of consciousness and chest pain. Identification of the aberrant vessel in this case was confirmed by using the method of “tapping” the superficial temporal artery to produce oscillating variations in the spectral Doppler waveform of the ECA as it was being interrogated. Because of the inappropriateness of performing angiography on this particular patient, definite confirmation of the identity of the anomalous vessel, in this particular case, was not available.
In a separate case, Aggarwal et al 7 found aberrant origins of the occipital artery, superior thyroid artery, and ascending pharyngeal artery from the left ICA on an angiogram of the cerebral vasculature performed due to an acute subarachnoid hemorrhage. The bifurcation of the CCA in this case occurred at the level of the fifth cervical vertebra, making the length of the CCA shortened when compared with the average length of the CCA. The ICA giving rise to the anomalous branches was occluded at its origin. The initial segment of the ECA on the affected side revealed absence of any branches. Sonographic evaluation of the carotid system was not used in this case.
Assessment of the vertebral arteries with B-mode sonography, color Doppler, and spectral Doppler waveform analysis is a vital part of the complete carotid artery examination. In normal anatomy, the vertebral arteries course superiorly through the foramina of the transverse processes of the cervical spine at the level of either the fifth or sixth cervical vertebra. Vaiman and Beckerman 8 performed a retrospective study to evaluate vertebral artery anomalies that affected approaches to neck surgical procedures. Results of their study revealed that out of 400 examinations, 23 revealed anomalous vertebral artery anatomy. Although this retrospective study did not use sonography as the diagnostic imaging modality, vascular sonographers should be aware of the anatomical variations possible with the vertebral system as the surgical implications of these variations can be quite serious.
Conclusion
Anomalous branching of the carotid and vertebral arteries is uncommon but does occur. Even though the gold standard for identifying these aberrations is angiography, sonographic examinations are usually the first imaging procedures used for evaluating these systems because of its relatively low cost, lack of radiation exposure, and patient comfort. Practicing vascular sonographers should consider the possibilities of anomalous branching from not only the ICA but the CCA as well and look for signs that the vertebral arteries may have anomalous configurations to their normal path. Such findings indicate the need for further evaluation in patients undergoing surgery on the head and neck.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.