
Abstract
Cervical cancer is not considered to be a highly prevalent carcinoma, as there are more cases of pre-cancer detected than invasive cases. It is also on the decline due to the use of routine Papanicolaou (Pap) tests, and immunizations against Human Papilloma Virus (HPV) have also helped diminish the number of cases. A case is presented of a cervical mass with metastases into the bladder and hydronephrosis of the kidneys detected using computed tomography (CT) and further evaluated using sonography. These imaging modalities together were able to provide global visualization of the pathology, resulting in accurate diagnosis and plan for treatment.
Introduction
Cervical cancer can be detected early, if not prevented, by an annual Papanicolaou test (Pap smear) performed. 1 Women of older age, those with at least three normal Pap smears, and those who have had a hysterectomy with the removal of the uterus and cervix do not necessarily need annual Pap smears, unless the cervix was specifically removed for cervical cancer treatment. 2 However, early detection does not always occur, as many cases are detected incidentally by diagnostic imaging examinations performed for other reasons. In these cases, the cancer is typically more advanced and often more difficult to treat. A case of cervical cancer is presented with abnormalities extending to other organ systems. The role of sonography in complement with other imaging modalities is discussed.
Case Report
A 58-year-old female presented to the ultrasound department for sonographic evaluation of the abdomen and pelvis with a chief complaint of back and flank pain accompanied with hematuria. A computed tomogram (CT) with contrast of the abdomen and pelvis had already been done. The CT showed bilateral hydronephrosis, potential bilateral hydroureters, and a neoplasm in the cervix (Figure 1). Based on the CT findings, the abdominal and pelvic sonograms were ordered for further investigation.
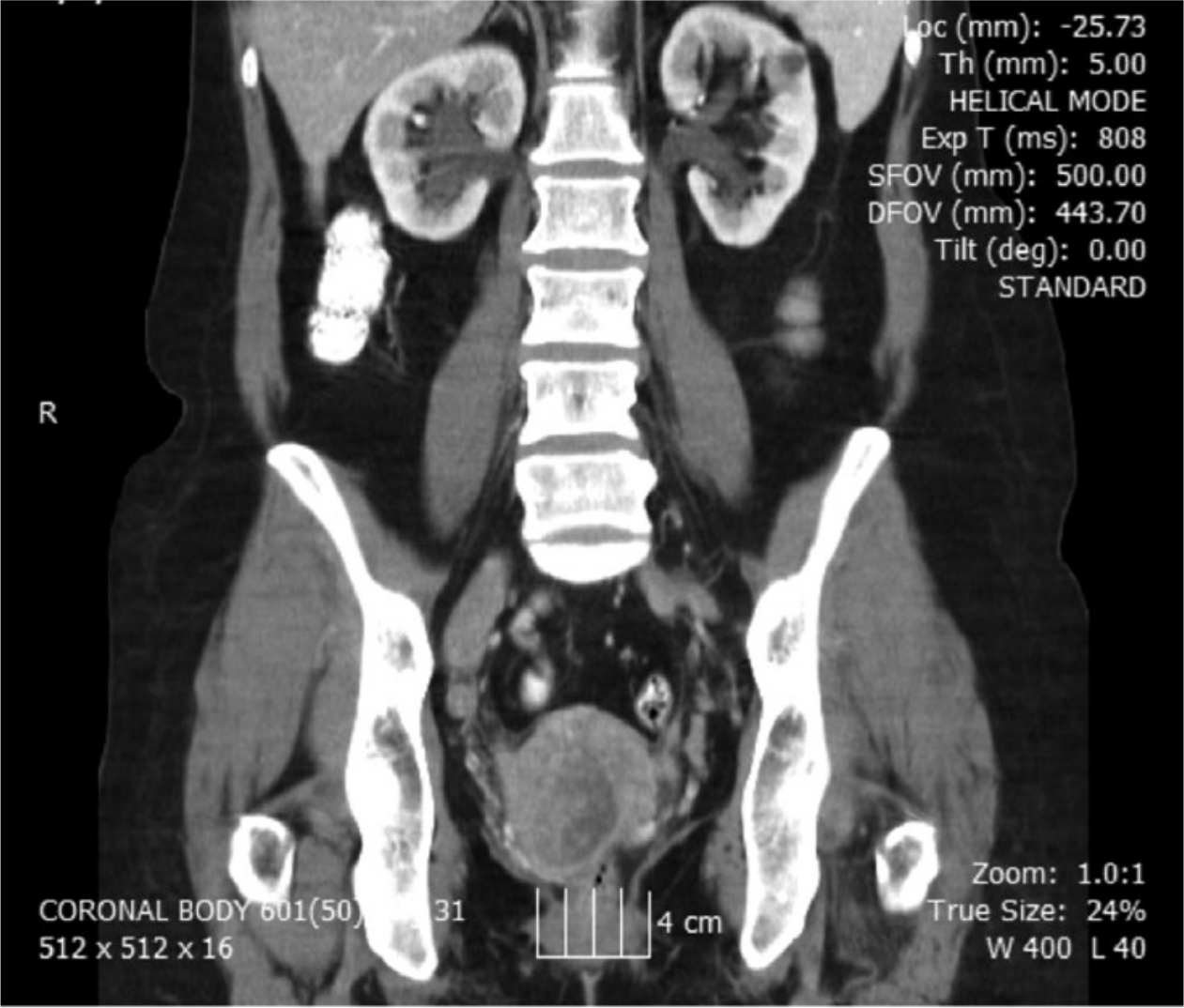
Coronal computed tomographic (CT) image of the abdomen and pelvis showing bilateral hydronephrosis, hydrouereters, and the presence of a cervical mass.
The complete abdominal sonogram was done using a 4 MHz curvilinear array transducer on a GE Logiq E9 ultrasound machine (General Electric Healthcare Ultrasound, Waukesha, Wisconsin, USA). The abdominal sonogram showed mild bilateral hydronephrosis (Figures 2 and 3) and bilateral hydroureters. The right hydroureter measured 1.08 cm at its widest point (Figure 4), and the left hydroureter measured 0.67 cm at its widest point (Figure 5). A small echogenic stone was seen in the distal right ureter measuring 0.32 cm (Figure 6). These findings were most concerning for the possibility of acute renal failure secondary to extrinsic obstruction.

Longitudinal gray-scale image of the right kidney showing mild hydronephrosis.
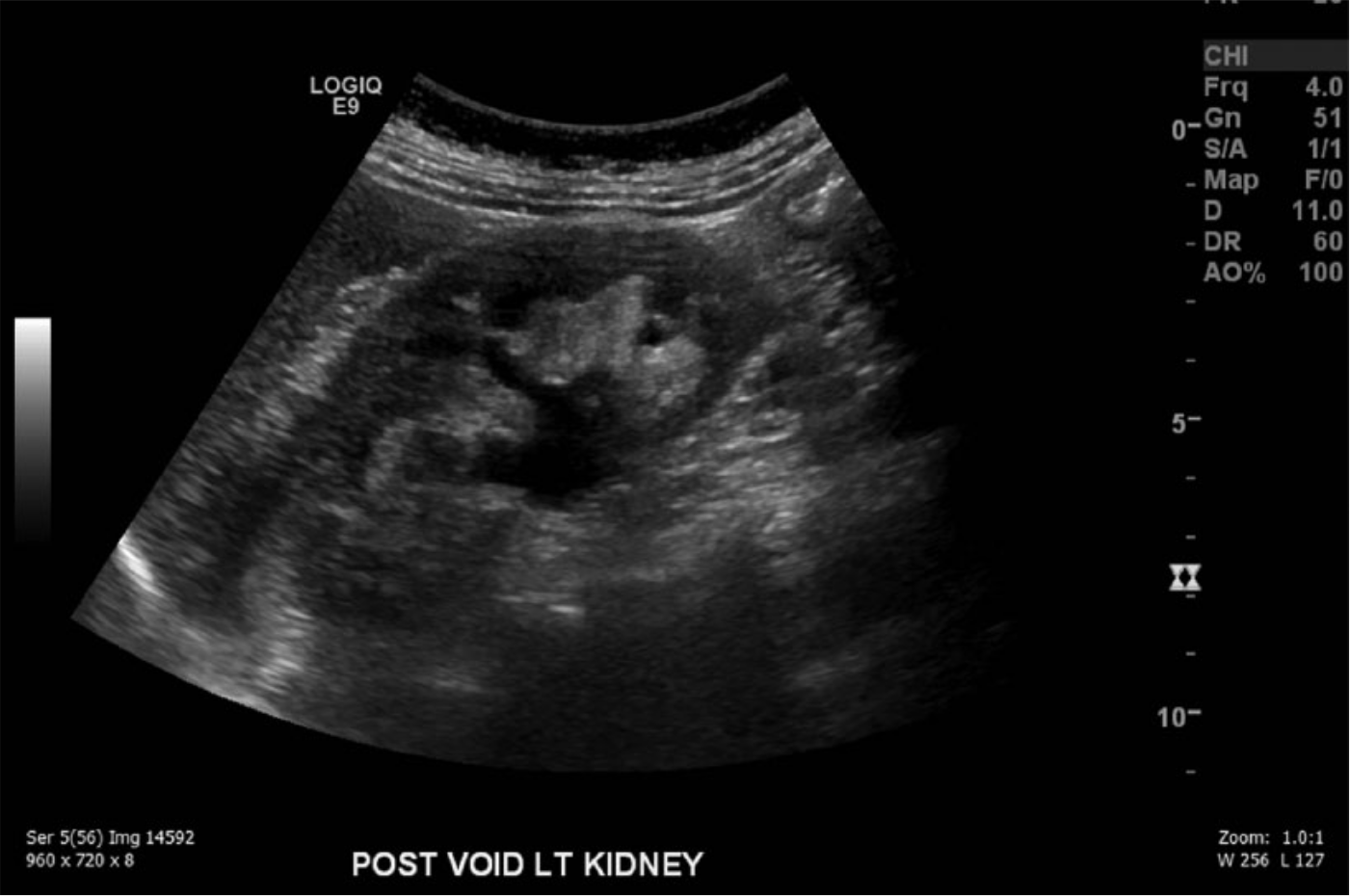
Longitudinal gray-scale image of the left kidney similarly showing mild hydronephrosis.
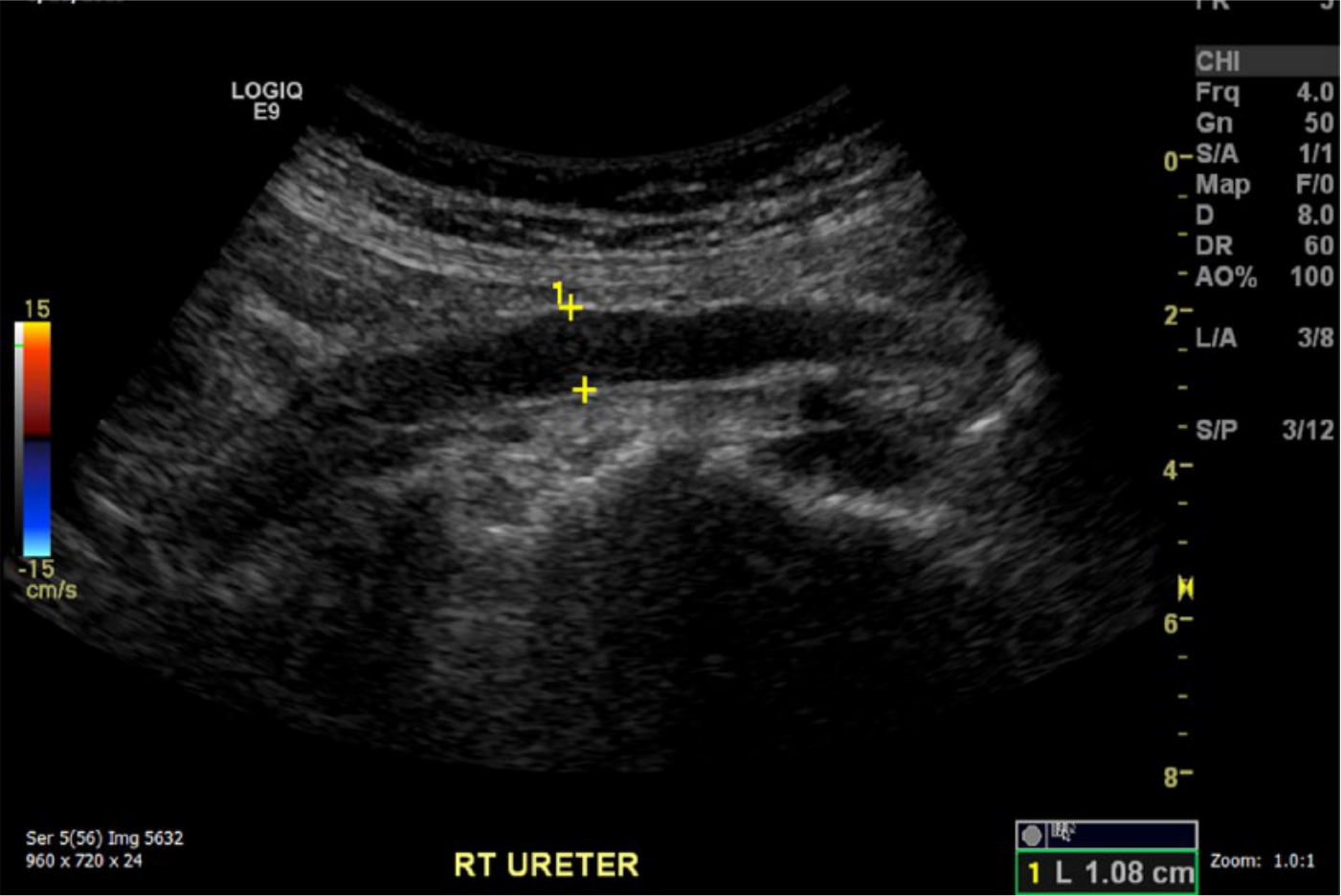
Sagittal gray-scale image showing a right hydroureter measuring 1.08 cm.
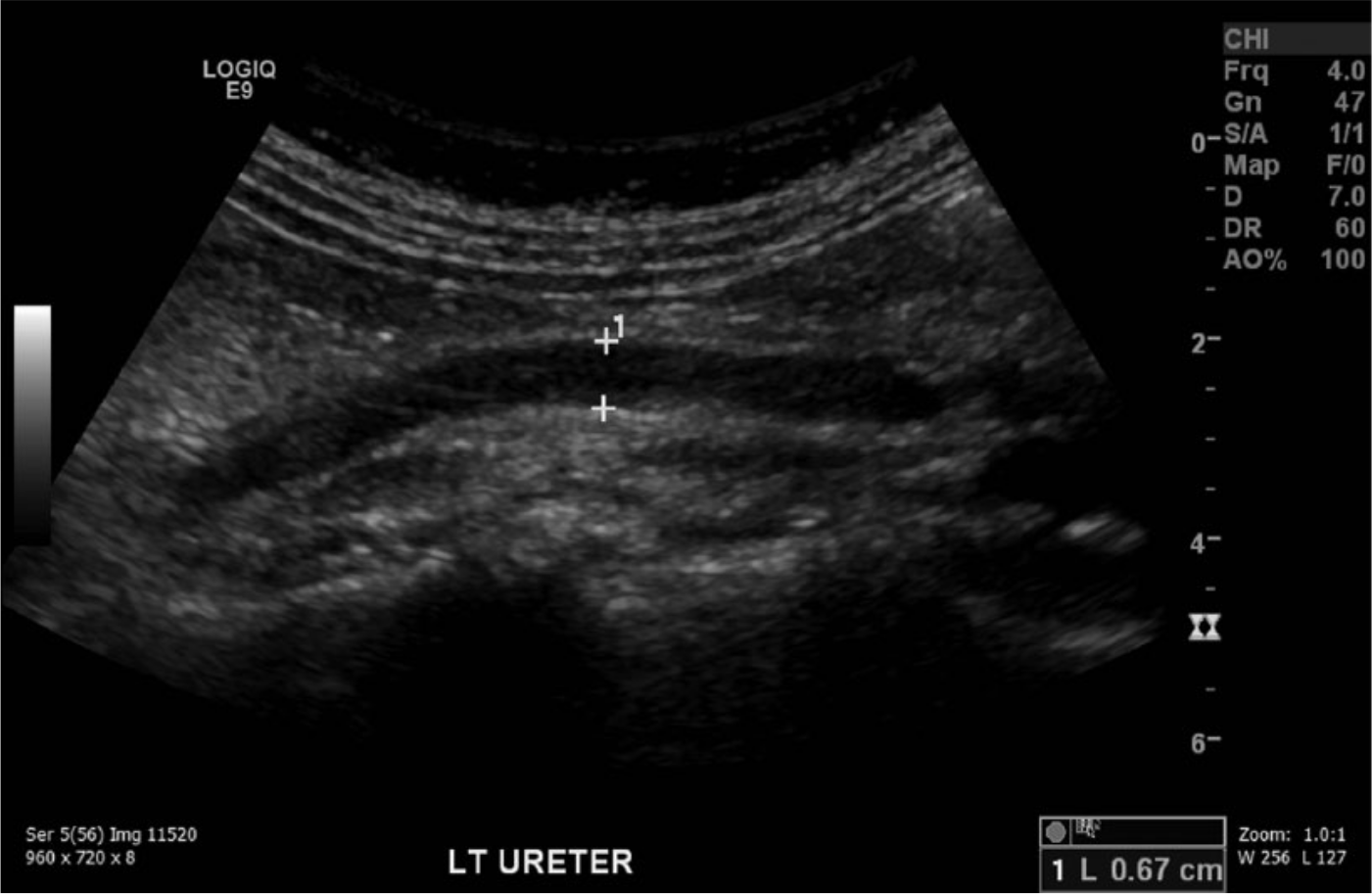
Sagittal gray-scale image showing a left hydroureter measuring 1.08 cm.
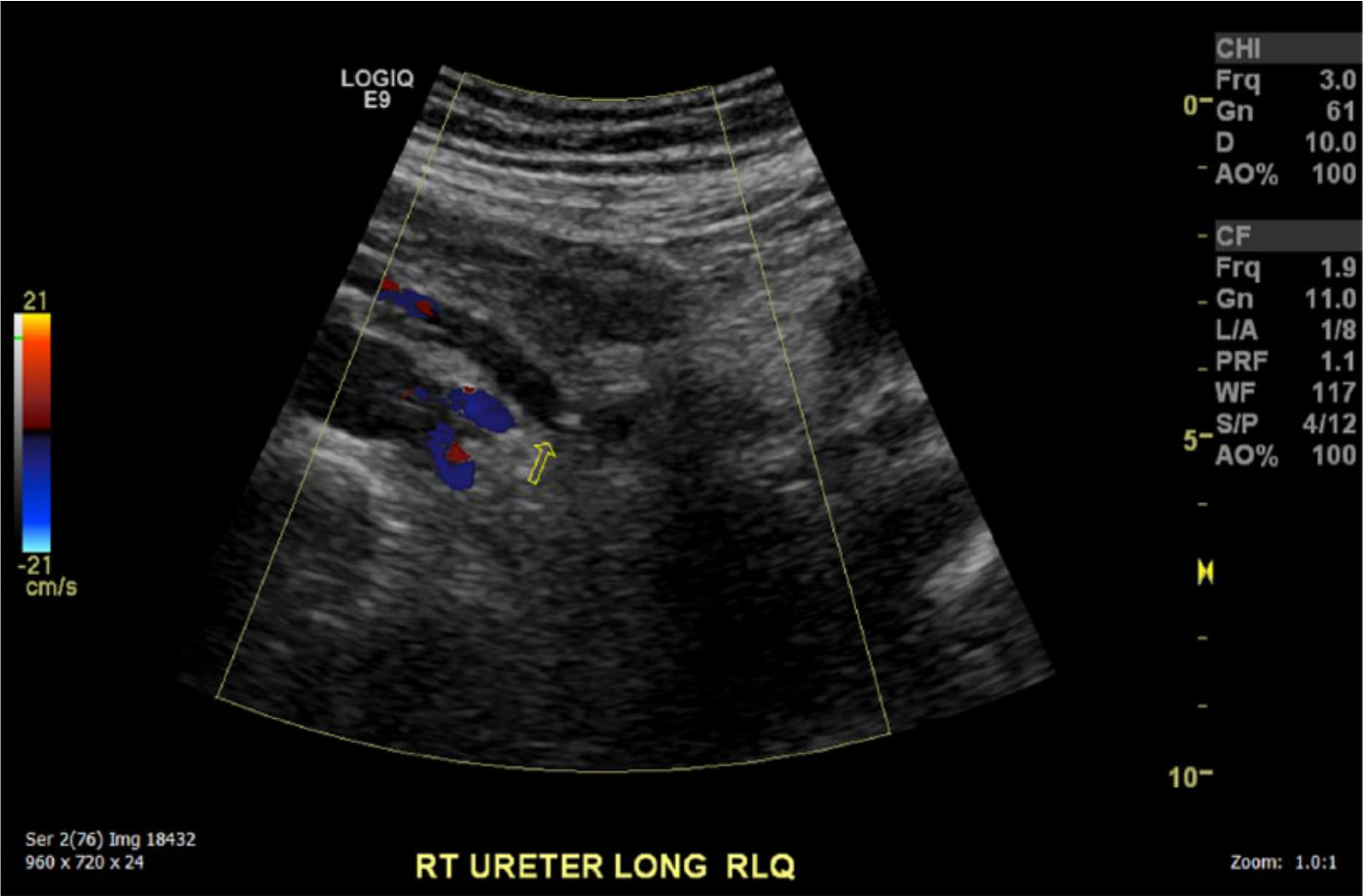
Transabdominal color Doppler sagittal image showing a stone in the right ureter.
A complete pelvic sonogram was then done using a combination of a transabdominal 4 MHz curvilinear array transducer and a transvaginal IC5-9-D transducer on the same Logiq E9 ultrasound machine. A hypoechoic cervical neoplasm was seen transabdominally posterior to the urinary bladder (Figure 7). The transvaginal approach provided better visualization of the cervical mass, which appeared irregular and fairly isoechoic and measured 5.4 × 4.7 × 4.6 cm (Figure 8). Evaluation of the urinary bladder pre-void showed hypoechoic poorly circumscribed masses extending from the cervix protruding into the bladder, consistent with metastases (Figure 9). These findings were considered consistent with advanced stage (stage IV) cervical cancer. Since this patient had a cervical neoplasm that was believed to be advanced stage cervical cancer, a biopsy was performed at a separate facility. The results were conclusive for cervical cancer. Sonography was again used to evaluate the renal system for level of renal failure, which again demonstrated mild hydronephrosis and hydroureters. Unfortunately, no further follow-up on outcome was available for this patient following referral to the outside facility.
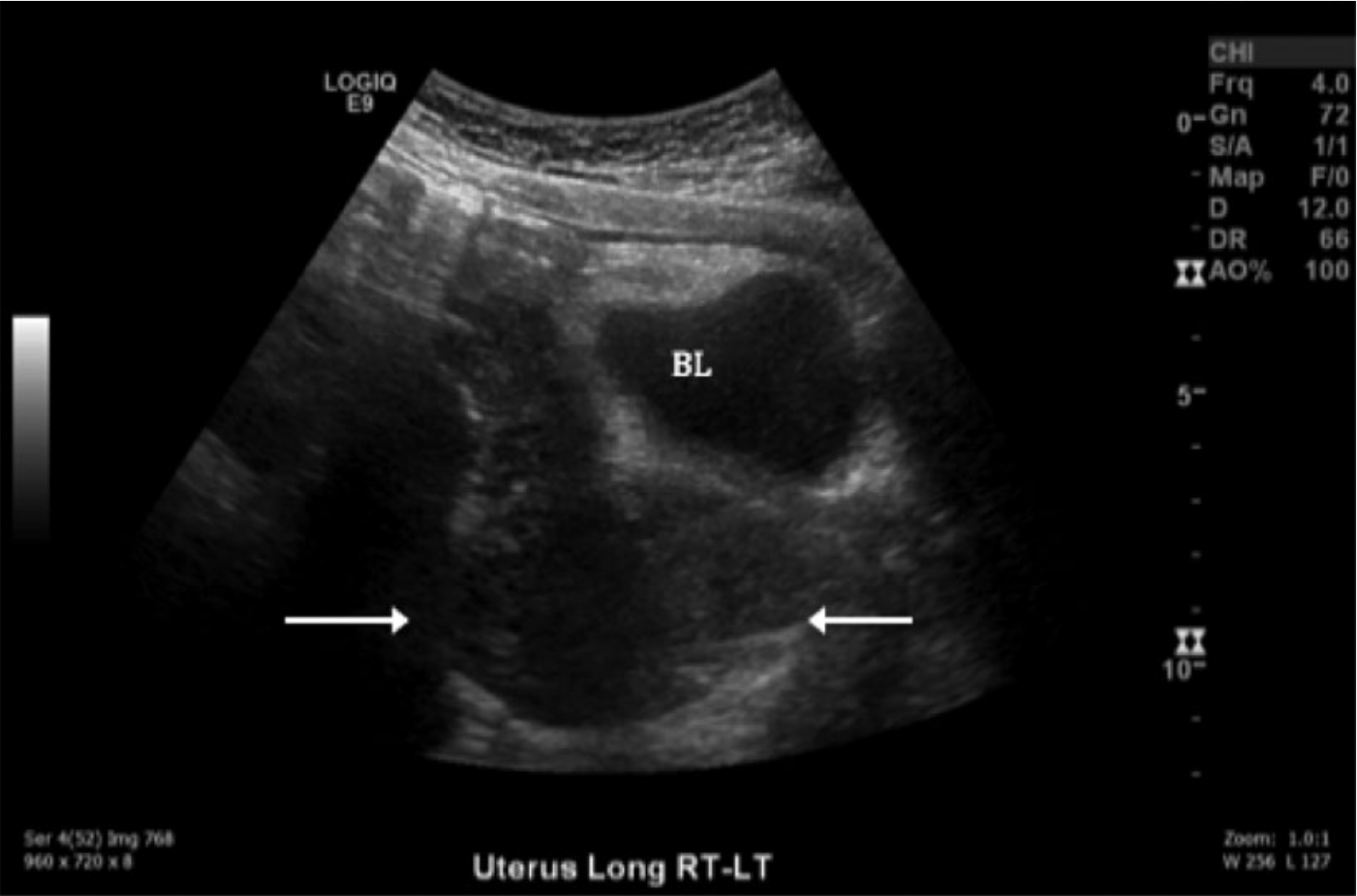
Transabdominal sagittal gray-scale image showing a cervical mass (arrows) located posterior to the urinary bladder (BL).
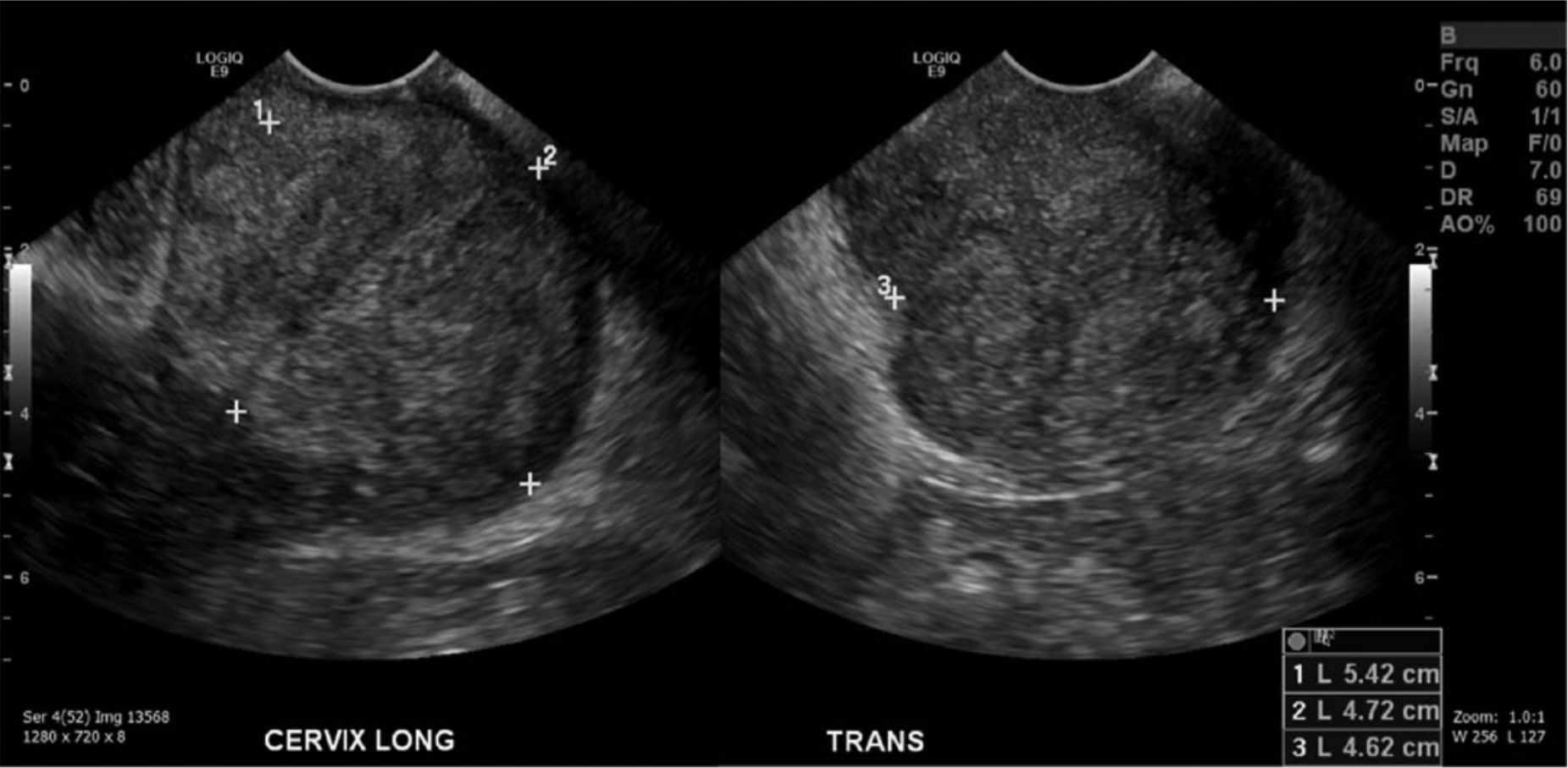
Transvaginal gray-scale sonograms showing a cervical neoplasm in the sagittal (LONG) and transverse (TRANS) planes.
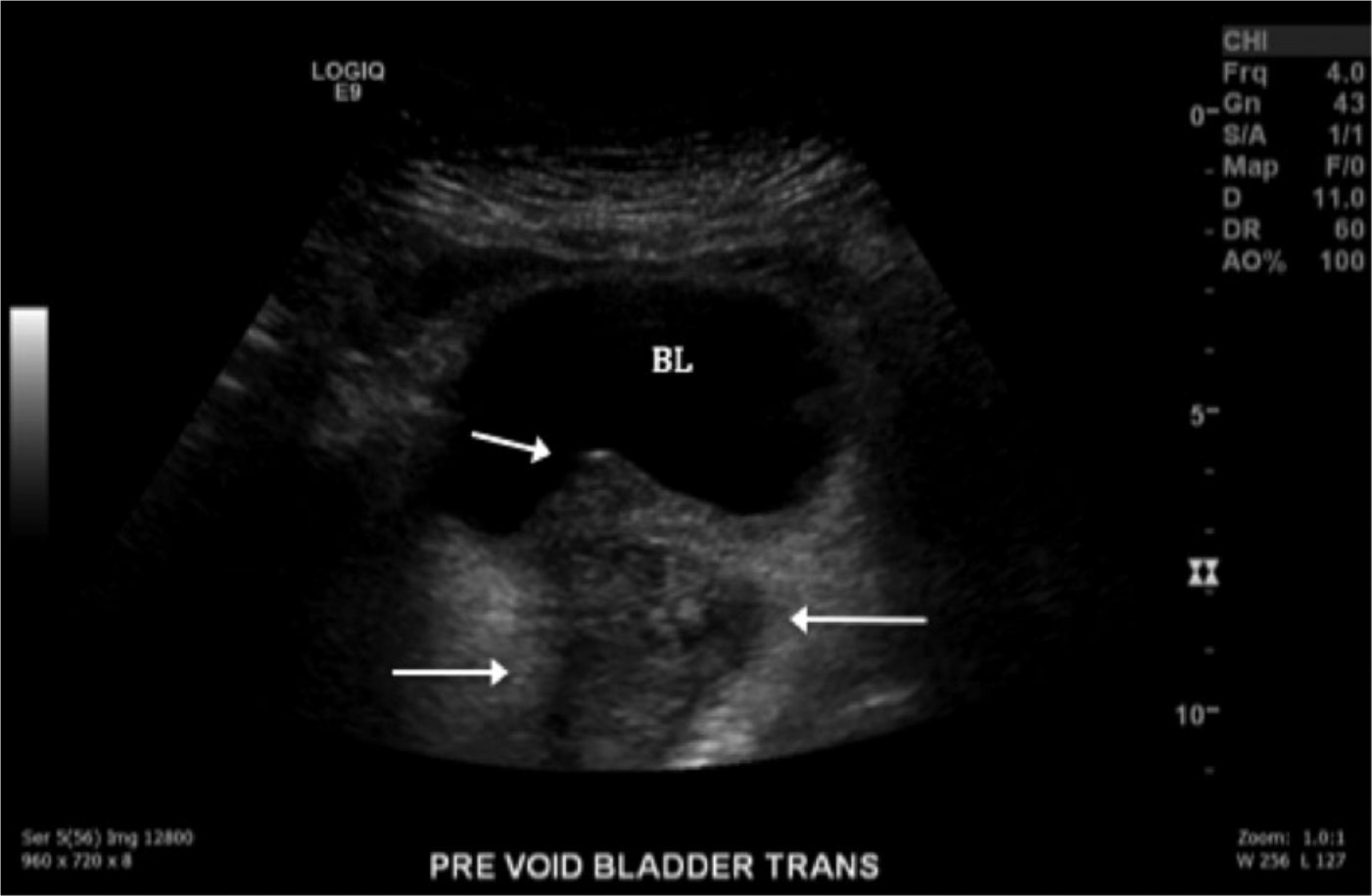
Transvaginal gray-scale sonogram showing metastases (arrows) within the bladder (BL) in the transverse plane.
Discussion
The majority of cervical cancers develop at the junction of the cervix where squamous cells and glandular cells meet, also known as the transformation zone. A large portion of cervical cancers are squamous cell carcinomas. 3 Human Papilloma Virus (HPV) can cause cervical cancer; however, different types of HPV may have an effect on the cancer itself. While a vaccination to prevent cervical cancer may greatly reduce the chances of developing the cancer, it does not enhance the survival rates of the cancer. 4 Cervical cancer usually is found in women under 50 years of age. As of 2015, the American Cancer Society predicts that 12 900 cases of cervical cancer will be detected and diagnosed annually. 5 An annual Pap test can evaluate for cervical cancer, as it often presents with no symptoms in earlier stages. If the cancer is detected before spread, there is greater chance of successful treatment and survival.
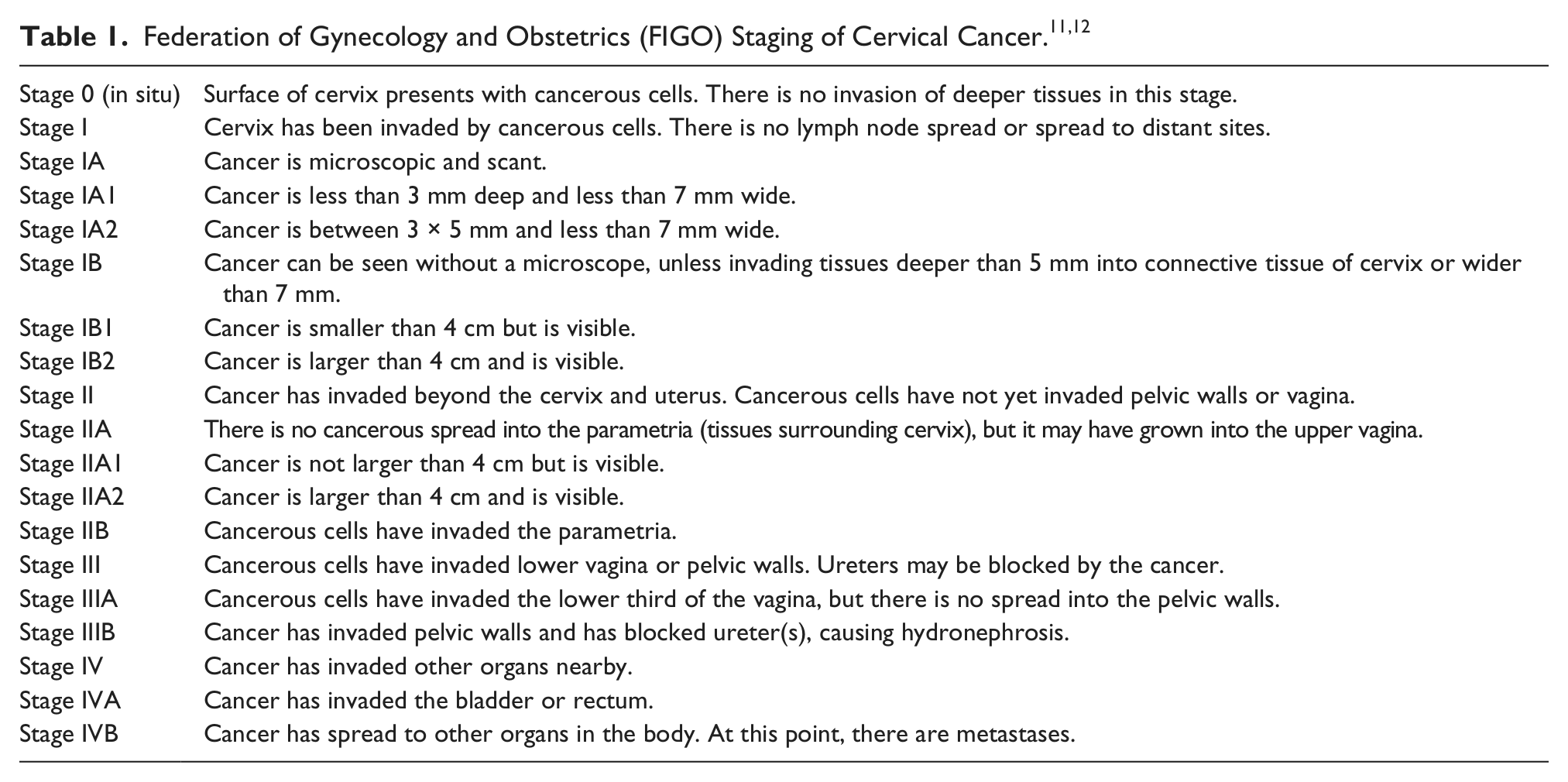
Cervical cancer usually begins in the transitional zone, where squamous and glandular cells meet. The cells become irregular and pre-cancerous, which may often lead to cancer if not treated and removed. After cancer is diagnosed, it is staged based on how voluminous the mass is, whether or not it has involved lymph nodes, and if it has spread to distant sites. Staging of cervical cancer is based on criteria from International Federation of Gynecology and Obstetrics (FIGO) and is also staged by the American Cancer Society (Table 1).6,7 It can be classified in stages zero through four. Stage 0 shows cancerous cells on the cervix surface without any invasion into deep tissues of the cervix. Stage I shows cancerous cells invading into the cervix; in this stage, the cells have not left the uterus (Figure 10a). In stage II, cancer has spread from the cervix and uterus; however, it has not spread to other parts of the pelvis. There is no lymph node involvement or distant metastases noted at this stage. During stage III, the cancer has spread into other parts of the pelvis and pelvis walls (Figure 10b). There is no lymph node involvement or metastases, but there can be blockage of ureters causing hydronephrosis. In stage IV, the cancer has spread to other regions of the body. In the case reported, metastases were found in the patient’s bladder.
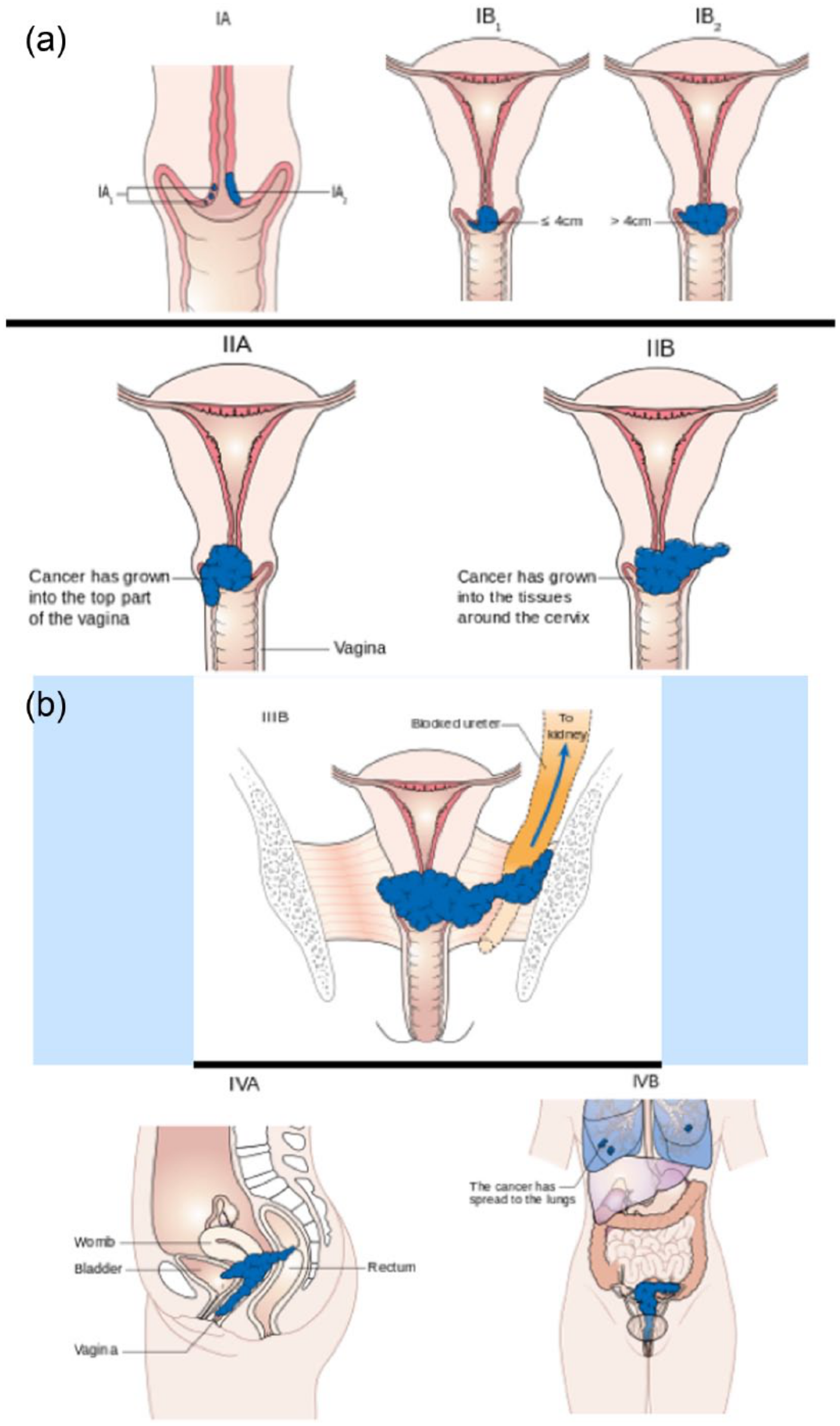
Schematic examples of the International Federation of Gynecology and Obstetrics (FIGO) and American Cancer Society systems for staging of cervical cancer. (a) Stages I and II. (b) Stages III and IV.
Computed tomography and sonography are routinely used to evaluate cervical masses that may be cancerous. In this particular case, a cervical mass was noted on CT and further investigated by sonography, both transabdominally and transvaginally. A CT with contrast was initially able to identify and localize the suspicious areas as well as the neoplasm. Sonography was able to confirm the CT findings as well as provide more detail regarding the region of interest and involvement with surrounding structures. Sonography was able to provide accurate measurements, characteristics of tissue appearance, and potential spread of the condition. This case clearly demonstrated the surrounding organ systems and how they can potentially be affected by the presence of cervical carcinoma.
There are several treatment options available for the various stages of cervical cancer. Surgery to remove the cancer described in this case likely would be difficult if at all possible because of the widespread metastases in the bladder. Other options for the patient include chemotherapy or radiation therapy. The type of drug used in chemotherapy can vary depending on the type of cancer and other medications the patient may currently be taking. For example, widely used chemotherapy drugs that can be used for cervical cancer are considered alkylating agents. These keep cancerous cells from reproducing by directly damaging the DNA of the cell. 8 In radiation therapy, the patient is subjected to high-energy radiation that target and kill actively dividing cancer cells, depending on the cancer’s radiosensitivity. A disadvantage to this treatment option is the fact that normal cell division is disrupted in the path of the radiation in addition to cancerous cell division. 9
According to the National Cancer Institute, approximately $1.3 billion was spent on cervical cancer care and treatment in the United States in 2010. 10 Some of this expenditure is being used to develop new treatment options based on HPV and tumor status. Studies are being done with adoptive T cell therapy involving the activation of stimulatory molecules for the blocking of inhibitory molecules to further allow anti-cancer T cell immune responses in the body. In these trials, T cells are taken from a patient and are treated to enhance the body’s response to the carcinoma. 11 There are personal preferences for treatment, depending on the side effects that patients are willing to cope with during and after treatment. Because the patient reported had stage IV cervical cancer, however, it is not clear that today’s clinical trials would prove useful or effective.
Metastases from cervical cancer can be distant or local. This particular case only showed fairly local metastases into the bladder, though there was an effect on the urinary system. The cervical mass was hypoechoic and dominated the cervical region. Hypoechoic and poorly circumscribed metastases were seen in the bladder as well. These findings are similar to other cases reported in the literature. Sonography typically shows a large, hypoechoic mass in the cervical region, usually with significant vascularity.12,13 Sonography has become a mainstay for evaluation of the mass because of its cost-effectiveness and availability.
Conclusion
Abdominal and pelvic sonography were used to assist in determining and characterizing the diagnosis of advanced stage cervical carcinoma. Computed tomography was able to give a global view of the problematic areas; sonography was then able to view the particular areas of focus, such as the cervix and urinary system. It initially noted the impairment of the renal system on the abdominal sonogram. The pelvic sonogram offered additional characterization of the cervical mass, along with documenting the presence of metastases into the bladder. Sonography, in combination with other imaging modalities, has been shown to be an advantageous and favorable evaluation method for analysis of ordinary anatomy as well as pathologic anatomy.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.